

BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
URL: http://hnmj.gums.ac.ir/article-1-980-en.html



2- Associate Professor, Epidemiology, Department of Public Health, School of Health and Nutrition, Lorestan University of Medical Sciences, Khorramabad, Iran.
3- Associate Professor, Department of Midwifery and Reproductive health, School of Nursing and Midwifery, Isfahan University of Medical Sciences, Isfahan, Iran.
4- PhD. Candidate of Reproductive Health, Department of Midwifery, Faculty of Nursing and Midwifery, Rasht Branch, Islamic Azad University, Rasht, Iran.
Introduction
Marriage is a sacrament through which the family is formed, and the main and most important ground for the manifestation of the function and the effect of intimacy and social relationships where sexual satisfaction can be effective in improving mental health [1]. Since the purpose of marriage is to meet the needs of the parties, if they fail to reach a satisfactory solution to their needs, deprivation, stress, failure, frustration, anger, and eventually a lack of security can emerge [2].
According to the World Health Organization (WHO) definition, health is a complete mental, physical, and social well-being and not just a lack of disease or infirmity. Therefore, the health and well-being of women who constitute half of the population of a society have been introduced as one of the indicators of development today. It has not only been recognized as a human right, but also its effects on the health of the family and society have gained increasing importance [3].
Sexual health is an important component for the health and well-being of individuals and is one of the basic and important factors in maintaining marital life. A good sexual function is one of the most important factors in the health of couples [4]. It is a part of human life and behavior and is so intertwined with a personality that it is not possible to consider it as an independent phenomenon. Sexual desire is always the center of attention, interest, and curiosity of mankind, and has an undeniable impact on the quality of life of an individual and his/her sexual partner [5].
One of the recent theories of sexual function is presented by Rosen et al. according to them, the sexual function has six components: desire, arousal, lubrication, orgasm, satisfaction, and pain [6]. Sexual dysfunction is defined as inhibitions in sexual desire or psycho-physiological changes in the sexual response cycle that causes distress and individual problems [7]. For a better understanding of sexual relations and providing solutions to improve sexual function in females, different concepts are proposed. One of them is Emotional Intelligence (EI). Intelligence is an adaptive problem-solving behavior that is oriented towards facilitating functional goals and adaptive growth [8]. Today, EI is very important in people’s lives. It is reported that 80% of people’s success in life is related to EI, and only 20% is related to IQ. However, the relationship between emotional intelligence and sexual function in females is still unknown [9].
EI is a kind of emotional processing that includes an appraisal of emotions in the self and others, appropriate expression of emotions, and adaptive regulation of emotions in a way that can lead to a better life. In other words, it is the ability to recognize the meanings and emotions and their relationships and solving problems based on them [10, 11]. Although marital life is only partially related to sexual relations, it may be one of the most important causes of happiness or lack of happiness in marital life, since if it cannot be persuasive, it leads to a feeling of deprivation, failure, and lack of security (endangered mental health), and as a result, disintegration of the family [1]. A meta-analytic study in Iran shows that the prevalence of sexual dysfunction in Iranian females is high. Therefore, further studies to identify the key factors affecting these health outcomes, and implementing interventional and preventive measures seem necessary [12].
With regard to what was discussed, the importance of sexual problems in disintegration of the family foundation, the importance of EI in interpersonal communications, the role of sexual relations as one of the important factors in quality of life, and the limited studies conducted on the relationship between EI and sexual function in Iran, the current study aimed at evaluating the association between EI and sexual function of Iranian females referred to health centers in Rasht City, Iran in 2015. Emotional problems in females can be a threat to the mental health of the family and eventually to the mental health of the community.
Materials and Methods
This is an analytical and correlational study conducted to study the effect of EI on the sexual function of the women living in Rasht City, Iran. The cluster random sampling method was used to recruit 100 study samples. The inclusion criteria were as follows: aged between 18 and 40 years, Muslim and Iranian; living in Rasht City or its suburbs, married and living with spouse, having sexual intercourse within the past four weeks; completion of the written consent form; ability to read and write; no history of previous marriage; no sexual diseases or problems, no psychological disorders; no obvious personality disorders, no history of addiction, no history of visiting a psychiatrist or psychologist during the past year, no drug use or hospitalization due to mental illness, not having a disease that can affect sexual function (e.g. vasculitis, cardiovascular, mental, internal, and nervous system diseases, thyroid and cancers), taking medications that somehow affect sexual function (e.g. anticholinergic drugs, psychoactive drugs, cardiovascular, nerve and hormonal medications), and not experiencing stress due to infidelity, serious illness, or divorce or observing the symptoms in husband. All these criteria were according to subjects’ self-reporting and health files.
Sampling was conducted using cluster random sampling method. In this regard, Rasht was divided into four regions: North, South, East, and West. Then, from each of these four regions, four health centers were selected based on the random number table, and all clients of the centers who met the inclusion criteria were selected as samples. The sample size was estimated 100, considering the correlation coefficient of 0.39 reported in the study by Willi and Burri [13], 30% sample dropout, 90% test power, and 95% Confidence Interval (CI).
The data collection tools were as follows: 1. Demographic information, including age, level of education, duration of the marriage; 2. The Bar-On emotional intelligence inventory: It is a self-report measure. The Persian version of this questionnaire was standardized by Samoei [14] with 90 items, which is scored based on a 5-point Likert-type scale (1=completely agree, 2=agree, 3=neither agree nor disagree, 4=disagree, 5=completely disagree). It consists of five scales as intrapersonal (assertiveness, self-regard, self-actualization, independence, and emotional self-awareness), interpersonal (interpersonal relationships, social responsibility, and empathy), adaptability (problem solving, reality testing, and flexibility), stress management (impulse control and stress tolerance), and general mood (happiness and optimism) [14]; and 3. The Female Sexual Function Index (FSFI): it was developed by Rosen et al. with 19 items and measures six domains of female sexual function including desire, arousal, lubrication, orgasm, satisfaction, and pain. Items are scored based on a Likert-type scale range from 5 to 0 (almost always to nothing). The score of each domain is obtained by adding the scores obtained from its questions. The Persian version validity has been confirmed by Mohammadi et al. [15]. The total score ranges from 0 to 95; the scores higher than 95 indicate a good sexual function in females.
The obtained were analyzed in SPSS V. 16 using descriptive statistics (mean and standard deviation) and statistical tests (Pearson correlation test). Stepwise regression analysis was employed to explain the variance of sexual function based on components of EI. In this method, the components that had the highest correlation with sexual function were entered into the regression model. In this regard, Model 1 (stress management components), Model 2 (stress management and interpersonal components), Model 3 (stress management, interpersonal, and intrapersonal components), and Model 4 (stress management, interpersonal, intrapersonal, and general mood components) were formed in four steps. The significance level was set at 0.05 (P<0.05).
Results
The study participants (n=100) were in the age range of 20-28 years (23.21±5.3) and their mean duration of marriage was 5±3.6 years. In terms of education level, most of them had a high school diploma (67%). The lowest degree was guidance school certificate and the highest one was an undergraduate degree. According to the results, the women’s mean sexual satisfaction was 20.59±5.10 and their mean EI was 315.32±14.64.
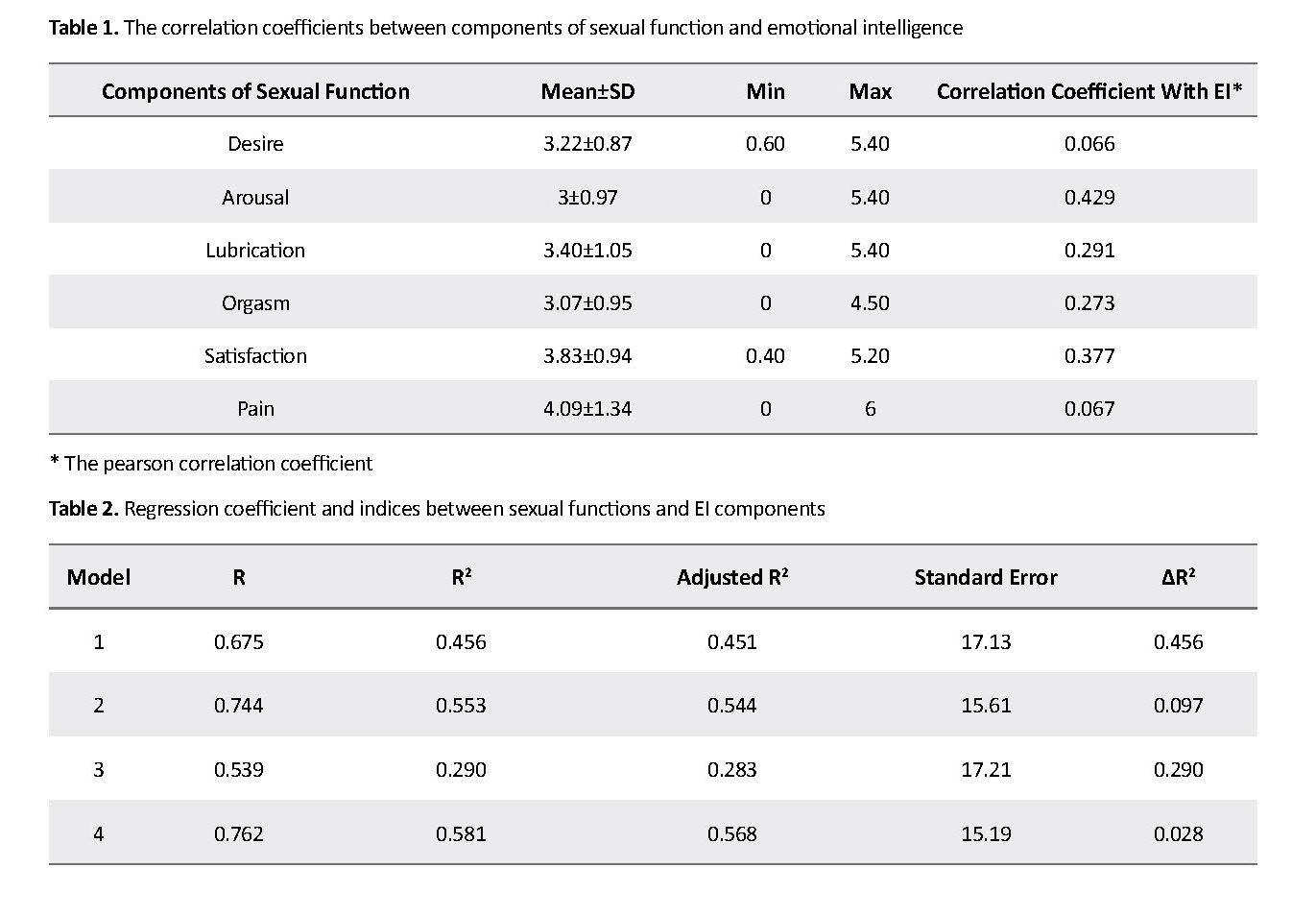
Table 1 shows that components of sexual function (desire, arousal, lubrication, orgasm, satisfaction, and pain) had a significant and positive correlation with EI. In examining the different dimensions of sexual function based on 98.5% cutoff point of the results, desire disorder was reported 12.5%; arousal disorder, 36%; problems in vaginal lubrication, 14%; orgasmic disorder, 16.5%; sexual dissatisfaction, 20%; and sexual pain disorder 12.5%.
Regression analysis results showed that the correlation between sexual function and EI in subjects was 0.60, and EI could predict 37% of the variance in female sexual function. The results of regression analyses were significant at 99% CI (P<0.001). In short, EI has a great role in explaining women’s sexual function.
In this study, we used stepwise regression analyses to explain sexual function variance based on the components of EI. So the components with the highest correlations with sexual functions were entered into the analysis. These are Model 1 (the component of stress management), Model 2 (interpersonal and stress management components), Model 3 (intrapersonal, interpersonal and stress management components), and Model 4 (general mood, intrapersonal, interpersonal and stress management components).
The regression coefficients indicated that EI and its components had a great role in explaining female sexual function as follows: 45% of sexual function was explained by stress management (Model 1); 54% by combination of stress management and interpersonal components (Model 2); 54% by combination of stress management, interpersonal, and intrapersonal components (Model 3); and 56% by combination of stress management, interpersonal, intrapersonal, and general mood components (Model 4). Moreover, the correlation between sexual function and Model 4 was 76% (Table 2).
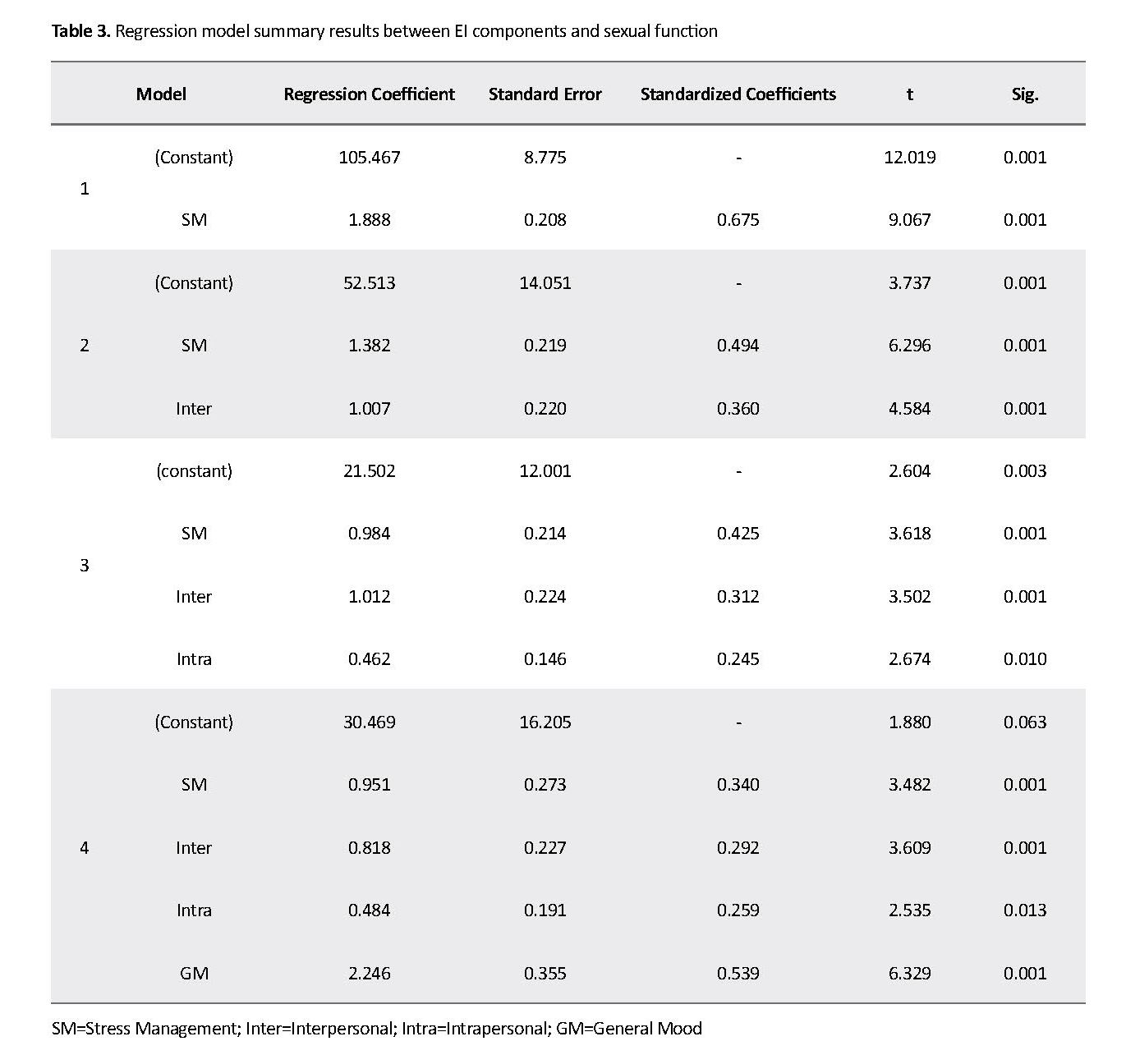
The summary of the regression model showed that Model 4 (stress management, interpersonal, intrapersonal and general mood components) had the highest power to predict changes in female sexual function (Table 3).
Discussion
The results of the current study revealed a significant and positive correlation between EI and sexual function components. In other words, females with higher EI can better understand their positive and negative emotions and their spouses, have higher ability to empathize and are more responsible, happier, and more optimistic. They also show more patience against the challenges of life, try to solve life problems in the best way, and are able to control themselves and cope with anger and frustration. The obtained results were in agreement with the findings of Jafaryazdi and Golzari [16]. According to their findings, high EI improves sexual function and subsequently increases marital satisfaction. Hasani et al. also showed that EI and effective emotional schema play a key role in marital satisfaction, which includes sexual satisfaction [17].
Based on studies, the importance of the relationship between EI and sexual function is that a large percentage of females have sexual dysfunction. In the study by Bakouei et al. for example, 19.2% of female subjects had sexual dysfunction [18].
In the other studies conducted by Palacios et al. in Spain and Zhang et al. in China, the prevalence of female sexual dysfunction was 40% and 56.8%, respectively [19, 20]. It seems that the prevalence of sexual dysfunction is high in females, but the observed differences in results of various studies may be due to the difference in demographic characteristics of subjects, the employed measurement tools, and the shame and embarrassment of females to express their sexual problems. Therefore, paying attention to EI and strengthening it in couples can promote sexual function and eliminate sexual disorders. In several studies, low sexual desire has been reported as the first and most commonly reported sexual complaint in females [21-24].
In the study by Safaei and Rajabzadeh, females had sexual disorders in all six domains where lubrication disorder showed the highest frequency, and the lowest prevalence of disorders was observed in the area of satisfaction [25]. However, in the current study, the most observed sexual disorder was related to sexual arousal, and the least reported sexual dysfunctions were sexual desire and pain. Perhaps the reason for this inconsistency is the difference in the age of subjects. Nicolson reported that sexual function and its components (except pain) had a significant correlation with marital adjustment [26].
Burri et al. studied EI and its association with orgasmic frequency in females and suggested that low EI was a significant risk factor for low orgasmic frequency, and it had a profound effect on females’ sexual function [27]. Likewise, Willi study results show that EI is the predictor of sexual function [13]. The current study results were also consistent with those of Silva et al. showing that EI plays a role in sexual functioning [28]. In the end, there is a significant and direct relationship between EI and components of sexual function.
The current study also reported a significant association between female sexual function and components of EI, since the combination of stress management, interpersonal, intrapersonal, and general mood scales showed the highest correlation with sexual function, where interpersonal scale (interpersonal relationships and empathy) had the highest correlation value. Empathy means understanding the emotions of others or according to some theorists the ability to perceive the mental experience, and sometimes share the emotions of another person [29]. These results were in agreement with the findings of Dokanei [30].
Studies conducted on females with higher EI show that they have the ability to regulate and understand their emotions such as fear and anger, and how to manage them. They can cope with the challenges and problems better, and strive for improving sexual relations and marital satisfaction. Overall, the current study concludes that EI plays an effective role in improving female sexual function. Therefore, using the findings of the study, it can be suggested that identifying emotional schemas can provide appropriate therapeutic, counseling, and educational interventions for a couple therapist. By laying the groundwork for increasing the EI of young couples and learning how to deal with the sex stresses and problems, a useful step can be taken to achieve satisfaction, promote sexual function and stability, and sustainability of marital life. These educational interventions are required in the consultations before and after marriage.
One of the limitations of the current study was that its results were limited to one city (Rasht, Iran), which may not be generalized to the whole population of females. In the current study, the self-report method was used and subjects may have reported higher scores for themselves. Therefore, further research is recommended using non-self-report measures. Also, the employment of other assessment tools along with other components that affect female sexual function can lead to interesting findings. Sexual dysfunction is highly prevalent among females and, given that EI has a direct and significant relationship with female sexual function, EI improvement in females can be considered as a therapeutic and counseling approach.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of Islamic Azad University, Rasht Branch (Ethical code: IR.IAU.RASHT.REC.1395.72).
Funding
The current study was approved by the Islamic Azad University of Rasht Branch.
Authors contributions
Designing, planning and implementing the study project, compiling and writing the article: Seyedeh Bahare Kamranpour; Guiding in compiling the proposal, methodology, and data analysis: Mohammad Javad Tarahi; Guiding in the selection of the study topic and compiling the proposal and final report: Shahnaz Kohan; and Contributing to all stages of the study and preparing the article: Shiva Alizadeh.
Conflict of interest
Authors declared no conflict of interest.
Acknowledgements
Authors would like to thank the Research Deputy of the University and Ms. Mahsa Shaeli for their valuable cooperation.
References
Morgan PC, Durtschi JA, Kimmes JG. Sexual and relationship satisfaction associated with shifts in dyadic trajectories of depressive symptoms in German couples across four years. Journal of Marital and Family Therapy. 2018; 44(4):655-70. [DOI:10.1111/jmft.12302] [PMID]
Aliakbari Dehkordi M. [Relationship between women sexual function and marital adjustment (Persian)]. Journal of Behavioral Sciences. 2010; 4(3):199-206.
Ahmadi B, Farzadi F, Alimohammadian M. [Policy challenges and implementation challenges for women's health and its promotion strategies: A qualitative approach based on experts' viewpoints (Persian)]. Payesh. 2010; 11(1):115-25.
Darvish-Mofrad-Kashani Z, Zafarghandi N, Raisi F, Aliasl J, Mokaberinejad R, Emaratkar E, et al. [A review of sexual health opinion from the perspective of Iranian traditional medicine (Persian)]. Medical History Journal. 2016; 8(27):73-90.
Nazarpour S, Simbar M, Ramezani Tehrani F, Alavi Majd H. [Relationship between sexual function and quality of life in post-menopausal Women (Persian)]. Journal of Mazandaran University of Medical Sciences. 2016; 26(143):90-8.
Rosson R. Woman sexual dysfunction: Revised and expanded definitions of woman's sexual dysfunction. The Journal of Sexual Medicine. 2004; 1(1):40-8. [DOI:10.1111/j.1743-6109.2004.10107.x] [PMID]
American Psychiatric Association. Diagnostic and Statistical Manual of mental disorders Text Revision) (DSM–IVTR). Washington D.C.: American Psychological Association; 2000.
Nesel DD. Spiritual orientation in relation to relation to spiritual intelligence: A consideration of traditional Christianity and new age individualistic spirituality [PhD. dissertation]. Australia: The University of South Australi; 2004.
Afkhami Aqda M, Abedini M, Serwat FL, Firozabadi Ardakan A, Nikokaran J. [A survey on the relation between EQ and marriage happiness of the married couples living in the City of Yazd (Persian)]. The Journal of Toloo-e-Behdasht. 2014; 13(4):57-65.
Bar-On R, Parker JDA. Handbook of emotional intelligence: Theory, development, assessment and application at home, school and in the workplace. San Francisco: Jossey-Bass; 2005 .
Lawance K, Sandra E. Sexual satisfaction in long-term heterosexual relationships: The interpersonal exchange model of sexual satisfaction. Personal Relationships. 1995; 2(4):267-85. [DOI:10.1111/j.1475-6811.1995.tb00092.x]
Ranjbaran M, Chizary M, Matory M. [Prevalence of female sexual dysfunction in Iran: Systematic review and meta-analysis (Persian)]. Journal of Sabzevar University of Medical Sciences. 2016; 22(7):1117-25.
Willi J, Burri A. Emotional intelligence and sexual functioning in a sample of Swiss men and women. The Journal of Sexual Medicine. 2015; 12(10):2051-60. [DOI:10.1111/jsm.12990] [PMID]
Tirgari AAK. [Emotional intelligence and mental health, approach, prevention strategies and programs to improve marriage (Persian)]. Journal of Research Social Welfare. 2004; 5(14):99-101.
Mohammadi Kh, Heydari M, Faghihzade S. [The Female Sexual Function Index (FSFI): Validation of the Iranian version (Persian)]. Payesh Journal. 2008; 7(3):269-78.
Jafaryazdi H, Golzari M. [Emotional intelligence and marital adjustment in married women employed in educational and training organization (Persian)]. Journal of Family Research. 2005; 1(4):379-92.
Hasani J, Naderi Y, Ramazanzadeh F, Pourabbass A. [The role of the emotional intelligence and emotional schema in women’s marital satisfaction (Persian)]. Journal of Family Research. 2014; 9(4):489-506.
Bakouei F, Omidvar SH, Nasiri F. [Prevalence of female sexual dysfunction in married women and its related factors (Babol 2006) (Persian)]. Journal of Babol University of Medical Sciences. 2007; 9(4):59-64.
Palacios S, Castaño R, Grazziotin A. Epidemiology of female sexual dysfunction. Maturitas. 2009; 63(2):119-23. [PMID]
Zhang AX, Pan LJ, Chen XY, Pan F, Kan YJ. An investigation on female sexual dysfunction among urban Chinese women in Nanjing. Zhonghua Nan Ke Xue. 2011; 17(6):488-91. [PMID]
Pastor Z. Female sexual desire disordersprevalence, classification and treatment possibilities. Ceska Gynekol. 2011; 76(1):59-64. [PMID]
Valadares AL, Pinto‐Neto AM, de Souza MH, Osis MJ, da Costa Paiva LH. The prevalence of the components of low sexual function and associated factors in middle‐aged women. The Journal of Sexual Medicine. 2011; 8(10):2851-8.
Goshtasbi A, Vahdaninia MAS, Rahimi Foroushani A, Mohammadi A. [Reproductive correlates of female sexual dysfunction in Kohgiluyeh-Boyerahmad Province (Persian)]. Payesh. 2008; 7(1):67-73.
Yeke Fallah L,Goodarzi M. [Prevalence of sexual dysfunction and related factors among married couples in Qazvin. The Journal of Qazvin University of Medical Sciences (Persian)]. 2009; 13(1):49-55.
Safaei M, Rajabzadeh S. [A Review of sexual functioning disorders amongst postmenopausal women referring to health centers of Torbat Heydariyeh in 2016 (Persian)]. Journal of Torbat Heydariyeh University of Medical Sciences. 2017; 4(4):23-28.
Nicolson P, Burr J. What is ‘normal’ about women's (hetero) sexual desire and orgasm? A report of an in-depth interview study. Social Science & Medicine. 2003; 57(9):1735-45. [DOI:10.1016/S0277-9536(03)00012-1]
Burri AV, Cherkas LM, Spector TD. Emotional intelligence and its association with orgasmic frequency in women. The Journal of Sexual Medicine. 2009; 6(7):1930-7. [DOI:10.1111/j.1743-6109.2009.01297.x] [PMID]
Silva P, Pereira H, Esgalhado G, Monteiro S, Afonso RM, Loureiro M. Emotional intelligence, sexual functioning, and subjective sexual well-being in Portuguese adults. British Journal of Education, Society & Behavioural Science. 2016; 15(1):1-11. [DOI:10.9734/BJESBS/2016/23481]
Sadock BJ, Sadock VA. Kaplan and Sadock’s pocket handbook of clinical psychiatry. Philadelphia: Lippincott Williams & Wilkins; 2010.
Dokanei Fard F, Behbodi M, Khayat M. [The evaluation of the share of emotional intelligence components in the prediction of the degree of Ilam female high school teachers' satisfaction, regarding their marriage (Persian)]. Educational Administration Research Quarterly. 2010; 2(1):61-82.
Received: 2018/10/22 | Accepted: 2019/01/29 | Published: 2019/04/1
| Rights and permissions | |
 | This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Articles Copyright © The Author(s).
Owned by Guilan University of Medical Sciences.
Co-published by Negah Institute for Scientific Communication.
Contact Information
JHNM Office, Guilan University of Medical Sciences P.O.Box 41635-1873, Rasht, Iran
Journal Tel: +9813 33553202
Publisher Tel: +9821 453 55 555; +9821 453 55 000
Email: holisticnmj@gmail.com, nursjournal@gums.ac.ir
