Wed, Apr 24, 2024
Volume 28, Issue 2 (3-2018)
JHNM 2018, 28(2): 129-135 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Rafiee A, Moradi Gomyek H, Haghighizade M H. Self-Treatment During Pregnancy and Its Related Factors. JHNM 2018; 28 (2) :129-135
URL: http://hnmj.gums.ac.ir/article-1-974-en.html
URL: http://hnmj.gums.ac.ir/article-1-974-en.html


1- Health Education (MSN), Instructor, School of Health, Ahvaz Jundishapur University of Medical Sciences, Ahvaz, Iran
2- Students Research Committee, Midwifery (BS.), School of Nursing and Midwifery, Ahvaz Jundishapur University of Medical Sciences, Ahvaz, Iran , m.hadis70@yahoo.com
3- Biostatistics (MSc.), Instructor, School of Health, Ahvaz Jundishapur University of Medical Sciences, Ahvaz, Iran
2- Students Research Committee, Midwifery (BS.), School of Nursing and Midwifery, Ahvaz Jundishapur University of Medical Sciences, Ahvaz, Iran , m.hadis70@yahoo.com
3- Biostatistics (MSc.), Instructor, School of Health, Ahvaz Jundishapur University of Medical Sciences, Ahvaz, Iran
Full-Text [PDF 513 kb]
(1348 Downloads)
| Abstract (HTML) (3188 Views)
The highest frequency of self-treatment with herbal drugs, according to the disease type, included colds (N=19; 33.3%), prevention of neonatal jaundice (N=15; 26.3%), and gastrointestinal diseases (N=14; 24.3%). The highest frequency of self-treatment with chemical medications included gastrointestinal diseases (N=24; 42.9%), headaches (N=19; 33.9%), and toothaches (N=8; 14.3%).
Assessing the use of herbal drugs based on the participants’ gestational ages showed that 45.6% used herbal drugs in the second trimester and 47.4% used these drugs in the third trimester. Assessing the use of chemical medications based on gestational age showed that 39.3% used these medications through self-treatment in the first trimester, 32.1% used them in the second, and 28.6% used them in the third trimester.
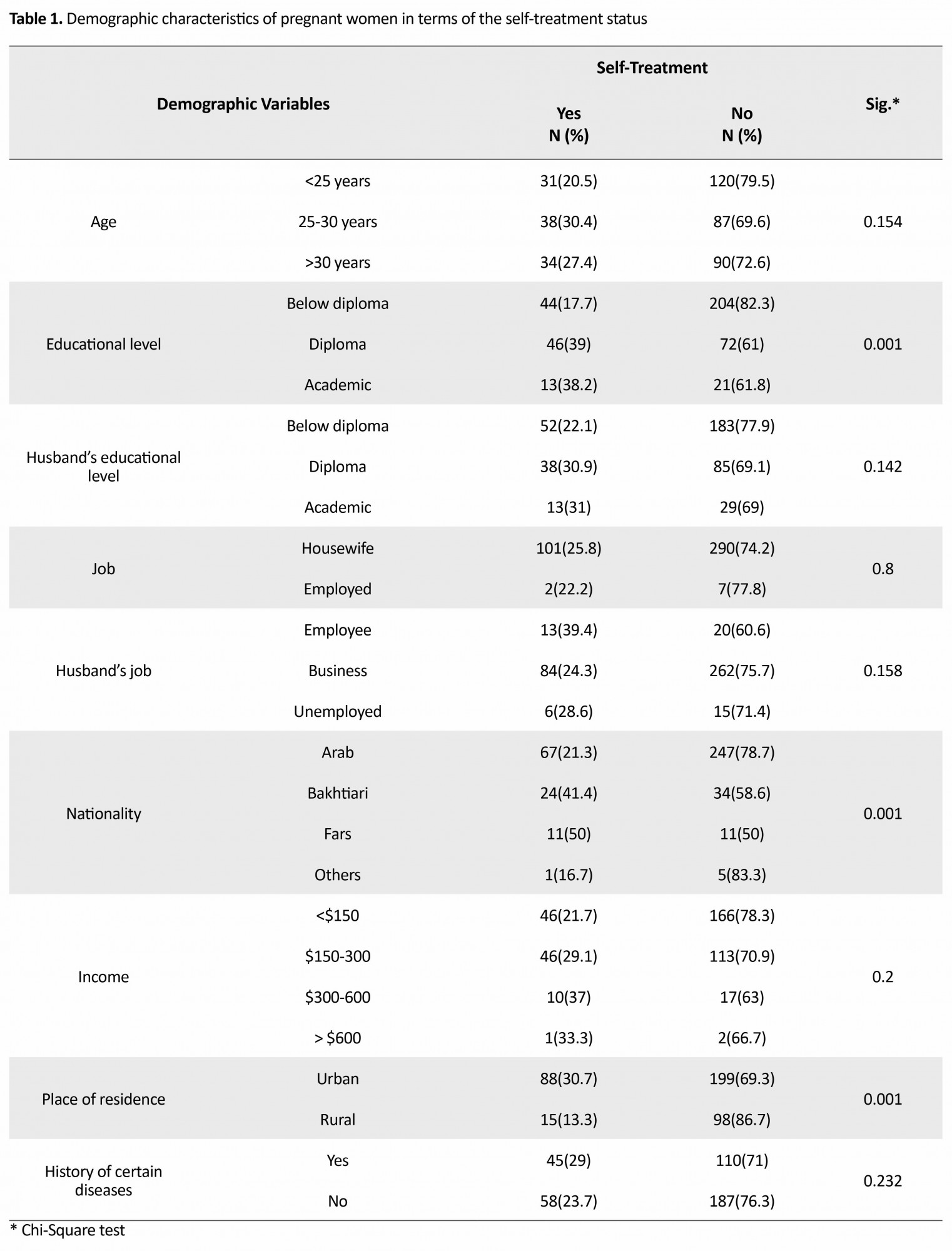
In this study, there was a significant relationship between self-medication and the variables, including the educational level and the place of residence of the pregnant women (P=0.05). However, there was no significant relationship between self-medication and age, ethnicity, the educational level of one’s spouse, the pregnant woman or her husband’s job, income, and a history of certain diseases (Table 1).
The most common causes of self-treatment (using medications without prescription of physician) in the pregnant women included believing in the treatment of the disease with medications alone (74.8%), safety of medications (74.8%), and the availability of medications at home (70.9%) (Table 2).

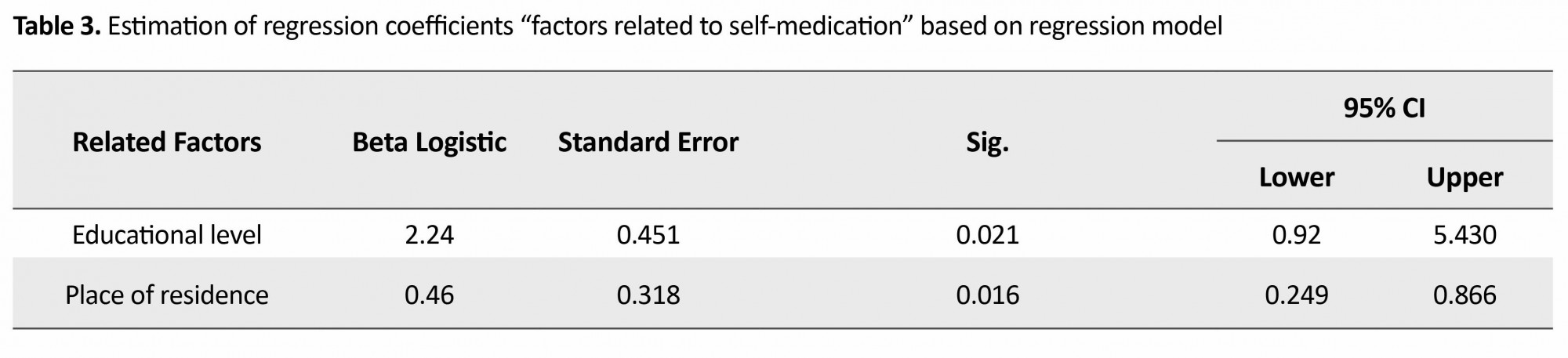
The results of logistic regression showed that the place of residence (95% CI=0.249-0.086; β=2.24) had the highest effect on self-treatment and after that, educational level (95% CI=0.92-5.43; β=0.46) affected self-medication (Table 3). The most frequent source of information on chemical medications in 39.3% of pregnant women was their own information and in 35.7% of pregnant women the source was a physician’s advice in previous referrals. In the context of herbal medicines, the most frequent source of information (57.9%) included family members, friends, and relatives.
Discussion
The results of this study showed that about one-fourth of the studied population underwent self-treatment, which is greater than the proportion of subjects reported in the study of Shamsi [18], almost equal to the proportion of subjects reported in the study of Ghanei [15], and less than the proportion of subjects reported in the studies of Pirzadeh in Isfahan, Alipoor in Qom, and Tabiei in Birjand [3, 11, 19], which could be due to the ethnic and cultural differences that govern different societies and the time differences between the studies.
In the present study, self-treatment was most common among in age group of 25-30 years old and it was the least common among the age group below 25 years. In the present study, the low rate of self-medication in the group younger than 25 could be due to the fact that this group of pregnant mothers had less experience of diseases and using medications than older mothers, so they could not use previous medications to treat their symptoms similar to those diseases. Nevertheless, in the study of Shamsi in Arak, the highest rate of self-treatment was observed in the age group of 20-25 years and the lowest rate of self-treatment was observed in the age group under 20 [18]. This difference can be due to the difference between the time of assessment in the present study and their survey, and the impact of warnings in mass media as well as the improvement of health status. In this study, the greatest rate of self-treatment was observed in pregnant women with high school diplomas and the lowest rate of self-treatment was observed in pregnant women with educational qualifications below the high-school level; in other words, less educated pregnant women may resort to less self-treatment due to the lack of information provided on the effects of medication on the pregnant body. This finding is consistent with the results of several studies [20, 21]. However, no significant statistical relationship was found between self-medication and educational level in the study by Ghanei [15].
In this study, there was a significant difference in the self-treatment rate between women living in urban and rural areas. In the study of Sharma et al. the prevalence of self-treatment in urban and rural areas of India was similar to results of the present study [22].
The most commonly reported instances of self-medication with chemical medication in the present study were observed for the treatment of gastrointestinal diseases, headaches, toothaches, and colds. The most commonly reported instances of self-medication with herbal drugs included colds, prevention of neonatal jaundice, and gastrointestinal diseases. In study of Shamsi, the most commonly reported self-treatment was for anemia, gastrointestinal diseases, respiratory diseases, and neurological diseases, respectively [18]. In Aeen Parast’s study, cold was the most commonly reported disease for self-medication [23].
In this study, the use of chemical and herbal drugs was approximately equal, while in Aeen Parast’s study, the use of chemical medications had a greater prevalence than other drugs [23]. In the study by Sereshty, more than half of the participants used herbal drugs during their pregnancy [24], while the rate of self-treatment with these medications (herbal drugs) was lower in the study of Sharma and colleagues [22]. In this study, more than one third of the samples used medications in the first trimester of pregnancy, the high-risk period for abnormalities, while in Dostdarsanaye’s study, only 8.5 percent of all women resorted to self-treatment in the first trimester of pregnancy [25]. Therefore, the whole society needs to be informed as soon as possible of the risks of inappropriate consumption of medications during pregnancy, which can lead to fetal complications; by the timely and the complete development of healthcare and treatment of diseases, the risks experienced by the vulnerable population, including women and their fetuses, can be prevented.
In this study, the most frequent sources of information on the use of chemical medications were pregnant women themselves and the advice of their doctors in previous visits. For women who consumed herbal medication, the most frequent sources of information included family members, friends, and relatives. Sereshti has also found that in most cases, the sources of information were the relatives of pregnant mothers [24]. Considering the widespread use of herbal drugs during pregnancy, it is necessary to train the staff in health centers about these products; since there is insufficient documentation about the safety of all herbal remedies during pregnancy, perinatal care providers should advise mothers not to endanger themselves and their fetuses to the possible risks.
The most common causes of self-treatment in this study included belief in the treatment of a disease via medication alone, the safety of medications, the availability of medications at home, and the inappropriate knowledge of the effects of medications. In contrast, in the study of Shamsi, ignoring the importance of diseases, the high cost of visiting doctors, lack of health insurance coverage, and previous experiences of disease were the most common causes [18]. Furthermore, the study of Alipour, Ghaneie, and Tabiei considered the lack of feeling the need to consult a physician during the disease was the most common cause of self-treatment [11, 12, 15]. Furthermore, in Moghaddamnia’s study, the accessibility of medication from the pharmacy without a physician’s prescription [26] was the most common cause of self-medication.
In general, it is recommended that medication suppliers should provide all the considerations, refuse to supply medications without a prescription, and provide training on the contraindications during pregnancy and lactation at the time of selling medications to customers. This issue can be an essential requirement in retraining courses for all the related occupational categories. Owing to the limited available sampling and selection of women who have gave birth at the hospital, it is not possible to generalize the results of this research.
Acknowledgements
The Deputy Chancellor of Research of Ahvaz Jundishapur University of Medical Sciences, who contributed with this research and provided the related costs is sincerely appreciated. All professors, authorities, and participants who devoted their valuable time to collaborate in this research and completed the questionnaires are also appreciated.
Conflict of Interest
No conflict of interest has been declared by the authors. All authors have agreed on the final version and meet at least one of the ICMJE authorship criteria, including substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data, drafting the article or revising it critically for important intellectual content.
References
Full-Text: (1497 Views)
Introduction
The overuse of medications and self-treatment, in general, is one of the greatest social and economic health problems in several countries, including Iran [1]. Medical specialists believe that the proper use of medications can treat diseases in most cases [2]. Today, we observe the higher accessibility that people to various medications, which results in a harmful social phenomenon: drug overuse or general self-treatment [3]. One of the most urgent cases that require a change of consumption pattern in the country is the pattern of drug use [4]. About 65 percent of the diseases in the country have been caused by an inappropriate consumption of mediations prescribed by physicians as well as illogical drug use. According to the World Health Organization (WHO), Iran is among the top 20 countries practicing drug consumption (it comes second in Asia-after China in terms of drug use) [5].
Self-treatment, defined as the use of herbal or synthetic drugs, is common in women and different medications are used to treat problems such as dysmenorrhea, menopausal symptoms, menstrual disorders, mood disorders, osteoporosis prevention, and pregnancy/lactation problems [6]. In particular, self-medication may increase in unwanted or undiagnosed pregnancies [7]. Studies conducted over the last few years show that the reasons for self-treatment include ignoring the importance of the disease, the high cost of visiting a doctor, no health insurance coverage, and previous experience of a similar disease. The most commonly used medications were antibiotics [8, 9].
Such issues led to self-treatment becoming a significant problem in the health system [10]. Self-medication is prevalent and on the rise throughout the world, especially antibiotics, which have become the most widely used type of medication around the world [11-13]. In the United States, various methods have been implemented to prevent self-medication, such as increasing people’s knowledge of the consequences of self-medication, training physicians and pharmacists on the proper administration of medications, and consulting consumers and providing them with brochures/catalogues [14]. Accordingly, paying attention to women has additional importance owing to the fundamental role of the mother in the Iranian family, especially while she is experiencing important periods in her life, such as pregnancy and lactation [15]. It can be stated that pregnancy in women is an event that can easily increase their use of medications and chemicals [16]. The results of the study by Leunge indicate that there is no difference in the rate of neonatal malformations between herbal and chemical medications [17]. Considering the increasing frequency of self-medication in the community and the direct role of individuals in the selection and the use of medication, this study aimed to determine the status of self-treatment and certain related factors in women.
Materials and Methods
The present descriptive-analytic study evaluates the status of self-medication of 400 women during pregnancy, who gave birth in educational hospitals in Ahwaz. Considering P=0.5, confidence interval (CI 95%, and d=0.05, the sample size was calculated based on the sample size formula of 400 people. In this study, the women who had vaginal or cesarean delivery were selected by the convenient sampling method and interviewed. For each hospital, two days a week were randomly selected, and the researcher referred to the hospitals to collect the data. Having a minimum gestational age of 20 weeks was considered as the inclusion criteria (this consideration was made based on the fact that abortion is the termination of pregnancy below 20 weeks).
The data collection method involved in-person interviews with the women who had given birth (normal and cesarean section) based on a checklist. Women signed the consent sheets they when were completely aware of their surroundings, and could remember and understand sharply. This study was conducted with the approval of the Ethics Committee by the code AJUMS.REC.1393.169. The interviews were conducted by one person and the research date was kept confidential.
The research instrument consisted of three parts: the first part included questions about the demographic characteristics of the studied women and their spouses; the second part included the women’s performance of self-treatment and questions about some of the diseases for which they would commonly resort to self-treatment; and the third part included questions about the medications that the pregnant women consumed and their views on the factors affecting the use of medication by self-treatment. The participants’ incomes were divided into four categories: poor, fair, medium, and high. Since pregnancy is limited to a short period of nine months and the use of even one dose of medication during pregnancy can have a negative effect on the fetus (especially in early pregnancy), even taking one dose of medication during pregnancy was considered as self-medication.
The instrument’s validity was tested by content validity analysis and in this questionnaire, the viewpoints of five gynecologists, and five midwifery and health faculty members of a medical university were used. According to the nature of the instrument, it was not necessary to determine the instrument’s reliability. The data were collected from October to November 2014 by interviews and through the completion of the questionnaires; then, the data were entered into the computer. Data on quantitative variables had normal distribution; thus, to describe the data, descriptive statistics tests were used, and to find the relationship between self-medication and other variables (self-treatment was considered as taking one or more medications without physician’s advice or prescription, except supplements of iron, folic acid, and multivitamins) the logistic regression test and the chi-square test were used. The data were analyzed using the SPSS software (version 21). P<0.05 were considered significant. The research project number of this article is 92s.41.
Results
All the 400 pregnant mothers studied were aged between 14 and 44 years. Women with high school diplomas had the highest rate of self-treatment (N=46; 39%). Other personal and social characteristics have been listed in the Table 1. In terms of healthcare delivery status, 388 patients received healthcare during pregnancy (97%). In this study, 103 pregnant women resorted to self-treatment during pregnancy (25.8%) and 297 pregnant women did not (74.2%). Of the women who conducted self-treatment, 47 used herbal agents (45.6%), 46 used chemical agents (44.7%), and 10 used both (9.7%). Of the 103 pregnant women who had resorted to self-treatment, 78(75.8%) were covered by insurance schemes and 25(24.3%) were not. Of the 297 patients who did not resort to self-treatment, 233(78.5%) were covered by insurance and 62(21%) were not.
The overuse of medications and self-treatment, in general, is one of the greatest social and economic health problems in several countries, including Iran [1]. Medical specialists believe that the proper use of medications can treat diseases in most cases [2]. Today, we observe the higher accessibility that people to various medications, which results in a harmful social phenomenon: drug overuse or general self-treatment [3]. One of the most urgent cases that require a change of consumption pattern in the country is the pattern of drug use [4]. About 65 percent of the diseases in the country have been caused by an inappropriate consumption of mediations prescribed by physicians as well as illogical drug use. According to the World Health Organization (WHO), Iran is among the top 20 countries practicing drug consumption (it comes second in Asia-after China in terms of drug use) [5].
Self-treatment, defined as the use of herbal or synthetic drugs, is common in women and different medications are used to treat problems such as dysmenorrhea, menopausal symptoms, menstrual disorders, mood disorders, osteoporosis prevention, and pregnancy/lactation problems [6]. In particular, self-medication may increase in unwanted or undiagnosed pregnancies [7]. Studies conducted over the last few years show that the reasons for self-treatment include ignoring the importance of the disease, the high cost of visiting a doctor, no health insurance coverage, and previous experience of a similar disease. The most commonly used medications were antibiotics [8, 9].
Such issues led to self-treatment becoming a significant problem in the health system [10]. Self-medication is prevalent and on the rise throughout the world, especially antibiotics, which have become the most widely used type of medication around the world [11-13]. In the United States, various methods have been implemented to prevent self-medication, such as increasing people’s knowledge of the consequences of self-medication, training physicians and pharmacists on the proper administration of medications, and consulting consumers and providing them with brochures/catalogues [14]. Accordingly, paying attention to women has additional importance owing to the fundamental role of the mother in the Iranian family, especially while she is experiencing important periods in her life, such as pregnancy and lactation [15]. It can be stated that pregnancy in women is an event that can easily increase their use of medications and chemicals [16]. The results of the study by Leunge indicate that there is no difference in the rate of neonatal malformations between herbal and chemical medications [17]. Considering the increasing frequency of self-medication in the community and the direct role of individuals in the selection and the use of medication, this study aimed to determine the status of self-treatment and certain related factors in women.
Materials and Methods
The present descriptive-analytic study evaluates the status of self-medication of 400 women during pregnancy, who gave birth in educational hospitals in Ahwaz. Considering P=0.5, confidence interval (CI 95%, and d=0.05, the sample size was calculated based on the sample size formula of 400 people. In this study, the women who had vaginal or cesarean delivery were selected by the convenient sampling method and interviewed. For each hospital, two days a week were randomly selected, and the researcher referred to the hospitals to collect the data. Having a minimum gestational age of 20 weeks was considered as the inclusion criteria (this consideration was made based on the fact that abortion is the termination of pregnancy below 20 weeks).
The data collection method involved in-person interviews with the women who had given birth (normal and cesarean section) based on a checklist. Women signed the consent sheets they when were completely aware of their surroundings, and could remember and understand sharply. This study was conducted with the approval of the Ethics Committee by the code AJUMS.REC.1393.169. The interviews were conducted by one person and the research date was kept confidential.
The research instrument consisted of three parts: the first part included questions about the demographic characteristics of the studied women and their spouses; the second part included the women’s performance of self-treatment and questions about some of the diseases for which they would commonly resort to self-treatment; and the third part included questions about the medications that the pregnant women consumed and their views on the factors affecting the use of medication by self-treatment. The participants’ incomes were divided into four categories: poor, fair, medium, and high. Since pregnancy is limited to a short period of nine months and the use of even one dose of medication during pregnancy can have a negative effect on the fetus (especially in early pregnancy), even taking one dose of medication during pregnancy was considered as self-medication.
The instrument’s validity was tested by content validity analysis and in this questionnaire, the viewpoints of five gynecologists, and five midwifery and health faculty members of a medical university were used. According to the nature of the instrument, it was not necessary to determine the instrument’s reliability. The data were collected from October to November 2014 by interviews and through the completion of the questionnaires; then, the data were entered into the computer. Data on quantitative variables had normal distribution; thus, to describe the data, descriptive statistics tests were used, and to find the relationship between self-medication and other variables (self-treatment was considered as taking one or more medications without physician’s advice or prescription, except supplements of iron, folic acid, and multivitamins) the logistic regression test and the chi-square test were used. The data were analyzed using the SPSS software (version 21). P<0.05 were considered significant. The research project number of this article is 92s.41.
Results
All the 400 pregnant mothers studied were aged between 14 and 44 years. Women with high school diplomas had the highest rate of self-treatment (N=46; 39%). Other personal and social characteristics have been listed in the Table 1. In terms of healthcare delivery status, 388 patients received healthcare during pregnancy (97%). In this study, 103 pregnant women resorted to self-treatment during pregnancy (25.8%) and 297 pregnant women did not (74.2%). Of the women who conducted self-treatment, 47 used herbal agents (45.6%), 46 used chemical agents (44.7%), and 10 used both (9.7%). Of the 103 pregnant women who had resorted to self-treatment, 78(75.8%) were covered by insurance schemes and 25(24.3%) were not. Of the 297 patients who did not resort to self-treatment, 233(78.5%) were covered by insurance and 62(21%) were not.
The highest frequency of self-treatment with herbal drugs, according to the disease type, included colds (N=19; 33.3%), prevention of neonatal jaundice (N=15; 26.3%), and gastrointestinal diseases (N=14; 24.3%). The highest frequency of self-treatment with chemical medications included gastrointestinal diseases (N=24; 42.9%), headaches (N=19; 33.9%), and toothaches (N=8; 14.3%).
Assessing the use of herbal drugs based on the participants’ gestational ages showed that 45.6% used herbal drugs in the second trimester and 47.4% used these drugs in the third trimester. Assessing the use of chemical medications based on gestational age showed that 39.3% used these medications through self-treatment in the first trimester, 32.1% used them in the second, and 28.6% used them in the third trimester.
In this study, there was a significant relationship between self-medication and the variables, including the educational level and the place of residence of the pregnant women (P=0.05). However, there was no significant relationship between self-medication and age, ethnicity, the educational level of one’s spouse, the pregnant woman or her husband’s job, income, and a history of certain diseases (Table 1).
The most common causes of self-treatment (using medications without prescription of physician) in the pregnant women included believing in the treatment of the disease with medications alone (74.8%), safety of medications (74.8%), and the availability of medications at home (70.9%) (Table 2).
The results of logistic regression showed that the place of residence (95% CI=0.249-0.086; β=2.24) had the highest effect on self-treatment and after that, educational level (95% CI=0.92-5.43; β=0.46) affected self-medication (Table 3). The most frequent source of information on chemical medications in 39.3% of pregnant women was their own information and in 35.7% of pregnant women the source was a physician’s advice in previous referrals. In the context of herbal medicines, the most frequent source of information (57.9%) included family members, friends, and relatives.
Discussion
The results of this study showed that about one-fourth of the studied population underwent self-treatment, which is greater than the proportion of subjects reported in the study of Shamsi [18], almost equal to the proportion of subjects reported in the study of Ghanei [15], and less than the proportion of subjects reported in the studies of Pirzadeh in Isfahan, Alipoor in Qom, and Tabiei in Birjand [3, 11, 19], which could be due to the ethnic and cultural differences that govern different societies and the time differences between the studies.
In the present study, self-treatment was most common among in age group of 25-30 years old and it was the least common among the age group below 25 years. In the present study, the low rate of self-medication in the group younger than 25 could be due to the fact that this group of pregnant mothers had less experience of diseases and using medications than older mothers, so they could not use previous medications to treat their symptoms similar to those diseases. Nevertheless, in the study of Shamsi in Arak, the highest rate of self-treatment was observed in the age group of 20-25 years and the lowest rate of self-treatment was observed in the age group under 20 [18]. This difference can be due to the difference between the time of assessment in the present study and their survey, and the impact of warnings in mass media as well as the improvement of health status. In this study, the greatest rate of self-treatment was observed in pregnant women with high school diplomas and the lowest rate of self-treatment was observed in pregnant women with educational qualifications below the high-school level; in other words, less educated pregnant women may resort to less self-treatment due to the lack of information provided on the effects of medication on the pregnant body. This finding is consistent with the results of several studies [20, 21]. However, no significant statistical relationship was found between self-medication and educational level in the study by Ghanei [15].
In this study, there was a significant difference in the self-treatment rate between women living in urban and rural areas. In the study of Sharma et al. the prevalence of self-treatment in urban and rural areas of India was similar to results of the present study [22].
The most commonly reported instances of self-medication with chemical medication in the present study were observed for the treatment of gastrointestinal diseases, headaches, toothaches, and colds. The most commonly reported instances of self-medication with herbal drugs included colds, prevention of neonatal jaundice, and gastrointestinal diseases. In study of Shamsi, the most commonly reported self-treatment was for anemia, gastrointestinal diseases, respiratory diseases, and neurological diseases, respectively [18]. In Aeen Parast’s study, cold was the most commonly reported disease for self-medication [23].
In this study, the use of chemical and herbal drugs was approximately equal, while in Aeen Parast’s study, the use of chemical medications had a greater prevalence than other drugs [23]. In the study by Sereshty, more than half of the participants used herbal drugs during their pregnancy [24], while the rate of self-treatment with these medications (herbal drugs) was lower in the study of Sharma and colleagues [22]. In this study, more than one third of the samples used medications in the first trimester of pregnancy, the high-risk period for abnormalities, while in Dostdarsanaye’s study, only 8.5 percent of all women resorted to self-treatment in the first trimester of pregnancy [25]. Therefore, the whole society needs to be informed as soon as possible of the risks of inappropriate consumption of medications during pregnancy, which can lead to fetal complications; by the timely and the complete development of healthcare and treatment of diseases, the risks experienced by the vulnerable population, including women and their fetuses, can be prevented.
In this study, the most frequent sources of information on the use of chemical medications were pregnant women themselves and the advice of their doctors in previous visits. For women who consumed herbal medication, the most frequent sources of information included family members, friends, and relatives. Sereshti has also found that in most cases, the sources of information were the relatives of pregnant mothers [24]. Considering the widespread use of herbal drugs during pregnancy, it is necessary to train the staff in health centers about these products; since there is insufficient documentation about the safety of all herbal remedies during pregnancy, perinatal care providers should advise mothers not to endanger themselves and their fetuses to the possible risks.
The most common causes of self-treatment in this study included belief in the treatment of a disease via medication alone, the safety of medications, the availability of medications at home, and the inappropriate knowledge of the effects of medications. In contrast, in the study of Shamsi, ignoring the importance of diseases, the high cost of visiting doctors, lack of health insurance coverage, and previous experiences of disease were the most common causes [18]. Furthermore, the study of Alipour, Ghaneie, and Tabiei considered the lack of feeling the need to consult a physician during the disease was the most common cause of self-treatment [11, 12, 15]. Furthermore, in Moghaddamnia’s study, the accessibility of medication from the pharmacy without a physician’s prescription [26] was the most common cause of self-medication.
In general, it is recommended that medication suppliers should provide all the considerations, refuse to supply medications without a prescription, and provide training on the contraindications during pregnancy and lactation at the time of selling medications to customers. This issue can be an essential requirement in retraining courses for all the related occupational categories. Owing to the limited available sampling and selection of women who have gave birth at the hospital, it is not possible to generalize the results of this research.
Acknowledgements
The Deputy Chancellor of Research of Ahvaz Jundishapur University of Medical Sciences, who contributed with this research and provided the related costs is sincerely appreciated. All professors, authorities, and participants who devoted their valuable time to collaborate in this research and completed the questionnaires are also appreciated.
Conflict of Interest
No conflict of interest has been declared by the authors. All authors have agreed on the final version and meet at least one of the ICMJE authorship criteria, including substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data, drafting the article or revising it critically for important intellectual content.
References
- Masoudi Alavi N, Izadi F, Ebadi A, Hajbagheri A. [Self treatment experience in diabetes mellitus type 2 (Persian)]. Iranian Journal of Endocrinology and Metabolism. 2009; 10(6):581-8.
- Palizvan MR, Rafiei M, Khazaee MR. [Assesment and comparison of drug use among medical and non-medical staff members in Markazi Province, Iran (Persian)]. Arak Medical University Journal. 2012; 15(61):27-34.
- Pirzadeh A, Gh S. [Knowledge and practice among women about self-medication based on health belief model (Persian)]. Journal of Gorgan University of Medical Science. 2012; 13(4):76-83.
- Hendrick B. Prescription drug use on the Rise in U.S. [Internet]. 2010 [Updated 2010 September 2]. Available from: https://www.webmd.com/mental-health/addiction/news/20100902/prescription-drug-use-on-the-rise-in-the-u-s#1
- Amani F, Shaker A, Mohaammadzadeh S, Sadegh M, Alaaf Akbari N, Sarrafe Smaeili S. [Drug use pattern between urban families in Ardabil city, Iran (Persian)]. Journal of Payavard Salamat. 2012; 5(5):36-45.
- Sharifi Rad GR, Mohebi S, Motalebi M. [Prevalence of self and modifiable factors affecting the health belief model in elderly Gonabad (Persian)]. Journal of Health System Research. 2011; 7(4):411-22.
- Jiménez E, Bosch F, López A, Costa J, Cos R, Baños JE. Patterns of regular drug use in Spanish childbearing women: changes elicited by pregnancy. European Journal of Clinical Pharmacology. 1998; 54(8):645–51. doi: 10.1007/s002280050528
- Parvan J, Ashna S, Pandya P, Mitul R. Knowledge, attitude and practice of self medication among under graduate MBBS students at tertiary care teaching hospital. International Journal of Health Sciences and Research. 2015; 5(7):192-197.
- Purreza A, Khalafi A, Ghiasi A, Mojahed F, Nurmohammadi M. [To identify self-medication practice among medical students of Tehran University of Medical Science (Persian)]. Iranian Journal of Epidemiology. 2013; 8(4):40-6.
- Ceremony A, Charmed F, Haqqani H. [Rates of self- medication factors in Tehran (Persian)]. Journal of Medicin and Purification. 2008; 15(1-2):14-19.
- Alipour Z, Eskandari N, Izadi Tamhe A, Faezipour A, Abedini Z, Khoramirad Rad A. [Relationship between personality characteristics and use of antibiotics (Persian)]. Journal of Holistic Nursing And Midwifery. 2015; 25(3):46-54.
- Tabiei S, Farajzadeh Z, Eizadpanah A. [Self-medicaton with drug amongst university students of Birjand (Persian)]. Modern Care Journal. 2012; 9(4):371-8.
- Patil SB, Vardhamane SH, Patil BV, Santoshkumar J, Binjawadgi AS, Kanaki AR. Self-medication practice and perceptions among undergraduate medical students: A cross-sectional study. Journal of clinical and diagnostic research. 2014; 8(12):HC20-3. doi: 10.7860/JCDR/2014/10579.5313
- Mycek MJ, Harvey RA, Champe PC. Lippincott’s illustrated reviews of pharmacology. Philadelphia: Williams & Wilkins ; 2000.
- Ghaneie R, Hemmati Maslakpak M, Baghi V. Self-medication in pregnant women. Journal of Research Development in Nursing and Midwifery. 2013; 10(1):92-98.
- Reiff-Eldridge R, Heffner CR, Ephross SA, Tennis PS, White AD, Andrews EB. Monitoring pregnancy outcomes after prenatal drug exposure through prospective pregnancy registries: A pharmaceutical company commitment. American Journal of Obstetrics and Gynecology. 2000; 182(1):159–63. doi: 10.1016/s0002-9378(00)70506-0
- Leung KY, Lee Yp, Chan HY, Lee CP, Hoi Yin MT. Are herbal medicinal products less teratogenic than Western pharmaceutical products. Age. 2002; 30(5.1):30-0.
- Shamsi M, Bayati A. [A survey of the prevalence of self-medication and the factors affecting it in pregnant mothers referring to health centers in Arak city (Persian)]. Journal of Jahrom University of Medical Sciences .2010; 3(7):34-41.
- Tabiei Sh, Farajzadeh Z, Eizadpanah A M. [Self-medication with drug amongst university students of Birjand (Persian)]. Modern Care: Scientific Quarterly of Birjand Nursing and Midwifery Faculty. 2012; 9(4):371-7.
- Tavakkoli R. Influences of educational status on self-medication: A comparative survey. Kowsar Medical Journal. 1996; 1(1):43-8.
- Lam CL, Catrativas MC, Munroc Launder IJ. Self medication by adolescence. Schweizerische medizinische Wochenschrift. 1998; 128(6):203-8.
- Sharma R, Verma U, Sharma C, Kapoor B. Self-medication among urban population of Jammu city. Indian Journal of Pharmacology. 2005; 37(1):40-3. doi: 10.4103/0253-7613.13856
- Aeen Parast A, Mafton F, Haghani H. [The Rate of self- treatment and other relating factor in Tehran City (Persian)]. Teb va Tazkiyeh. 2008; 16(1-2):14-19.
- Sereshti M, Azari P, Rafiean M. [Rate of consumer plan drug in women with pregnancy in korsedtan city (Persian)]. Journal of Shahrekord University of Medical Sciences. 2006; 2(3):82-6.
- Dosttar Sanaye M, Sobhani A. Pattern of drug consumption and its changes during the first trimester of pregnancy (Persian)]. Journal of Qazvin University of Medical Sciences. 2002; 5 (4) :55-61.
- Moghadamnia A, Ghadimi R. [Self medication in common cold in people in 15-45 years in Babol city (Persian)]. Scientific Journal of Babol University of Medical Sciences. 2001; 2(1):26-32.
Article Type : Research |
Subject:
Special
Received: 2018/03/19 | Accepted: 2018/03/19 | Published: 2018/03/19
Received: 2018/03/19 | Accepted: 2018/03/19 | Published: 2018/03/19
References
1. Masoudi Alavi N, Izadi F, Ebadi A, Hajbagheri A. [Self treatment experience in diabetes mellitus type 2 (Persian)]. Iranian Journal of Endocrinology and Metabolism. 2009; 10(6):581-8.
2. Palizvan MR, Rafiei M, Khazaee MR. [Assesment and comparison of drug use among medical and non-medical staff members in Markazi Province, Iran (Persian)]. Arak Medical University Journal. 2012; 15(61):27-34.
3. Pirzadeh A, Gh S. [Knowledge and practice among women about self-medication based on health belief model (Persian)]. Journal of Gorgan University of Medical Science. 2012; 13(4):76-83.
4. Hendrick B. Prescription drug use on the Rise in U.S. [Internet]. 2010 [Updated 2010 September 2]. Available from: https://www.webmd.com/mental-health/addiction/news/20100902/prescription-drug-use-on-the-rise-in-the-u-s#1
5. Amani F, Shaker A, Mohaammadzadeh S, Sadegh M, Alaaf Akbari N, Sarrafe Smaeili S. [Drug use pattern between urban families in Ardabil city, Iran (Persian)]. Journal of Payavard Salamat. 2012; 5(5):36-45.
6. Sharifi Rad GR, Mohebi S, Motalebi M. [Prevalence of self and modifiable factors affecting the health belief model in elderly Gonabad (Persian)]. Journal of Health System Research. 2011; 7(4):411-22.
7. Jiménez E, Bosch F, López A, Costa J, Cos R, Ba-os JE. Patterns of regular drug use in Spanish childbearing women: changes elicited by pregnancy. European Journal of Clinical Pharmacology. 1998; 54(8):645–51. doi: 10.1007/s002280050528 [DOI:10.1007/s002280050528]
8. Parvan J, Ashna S, Pandya P, Mitul R. Knowledge, attitude and practice of self medication among under graduate MBBS students at tertiary care teaching hospital. International Journal of Health Sciences and Research. 2015; 5(7):192-197.
9. Purreza A, Khalafi A, Ghiasi A, Mojahed F, Nurmohammadi M. [To identify self-medication practice among medical students of Tehran University of Medical Science (Persian)]. Iranian Journal of Epidemiology. 2013; 8(4):40-6.
10. Ceremony A, Charmed F, Haqqani H. [Rates of self- medication factors in Tehran (Persian)]. Journal of Medicin and Purification. 2008; 15(1-2):14-19.
11. Alipour Z, Eskandari N, Izadi Tamhe A, Faezipour A, Abedini Z, Khoramirad Rad A. [Relationship between personality characteristics and use of antibiotics (Persian)]. Journal of Holistic Nursing And Midwifery. 2015; 25(3):46-54.
12. Tabiei S, Farajzadeh Z, Eizadpanah A. [Self-medicaton with drug amongst university students of Birjand (Persian)]. Modern Care Journal. 2012; 9(4):371-8.
13. Patil SB, Vardhamane SH, Patil BV, Santoshkumar J, Binjawadgi AS, Kanaki AR. Self-medication practice and perceptions among undergraduate medical students: A cross-sectional study. Journal of clinical and diagnostic research. 2014; 8(12):HC20-3. doi: 10.7860/JCDR/2014/10579.5313 [DOI:10.7860/JCDR/2014/10579.5313]
14. Mycek MJ, Harvey RA, Champe PC. Lippincott's illustrated reviews of pharmacology. Philadelphia: Williams & Wilkins; 2000.
15. Ghaneie R, Hemmati Maslakpak M, Baghi V. Self-medication in pregnant women. Journal of Research Development in Nursing and Midwifery. 2013; 10(1):92-98.
16. Reiff-Eldridge R, Heffner CR, Ephross SA, Tennis PS, White AD, Andrews EB. Monitoring pregnancy outcomes after prenatal drug exposure through prospective pregnancy registries: A pharmaceutical company commitment. American Journal of Obstetrics and Gynecology. 2000; 182(1):159–63. doi: 10.1016/s0002-9378(00)70506-0 [DOI:10.1016/S0002-9378(00)70506-0]
17. Leung KY, Lee Yp, Chan HY, Lee CP, Hoi Yin MT. Are herbal medicinal products less teratogenic than Western pharmaceutical products. Age. 2002; 30(5.1):30-0.
18. Shamsi M, Bayati A. [A survey of the prevalence of self-medication and the factors affecting it in pregnant mothers referring to health centers in Arak city (Persian)]. Journal of Jahrom University of Medical Sciences .2010; 3(7):34-41.
19. Tabiei Sh, Farajzadeh Z, Eizadpanah A M. [Self-medication with drug amongst university students of Birjand (Persian)]. Modern Care: Scientific Quarterly of Birjand Nursing and Midwifery Faculty. 2012; 9(4):371-7.
20. Tavakkoli R. Influences of educational status on self-medication: A comparative survey. Kowsar Medical Journal. 1996; 1(1):43-8.
21. Lam CL, Catrativas MC, Munroc Launder IJ. Self medication by adolescence. Schweizerische medizinische Wochenschrift. 1998; 128(6):203-8.
22. Sharma R, Verma U, Sharma C, Kapoor B. Self-medication among urban population of Jammu city. Indian Journal of Pharmacology. 2005; 37(1):40-3. doi: 10.4103/0253-7613.13856 [DOI:10.4103/0253-7613.13856]
23. Aeen Parast A, Mafton F, Haghani H. [The Rate of self- treatment and other relating factor in Tehran City (Persian)]. Teb va Tazkiyeh. 2008; 16(1-2):14-19.
24. Sereshti M, Azari P, Rafiean M. [Rate of consumer plan drug in women with pregnancy in korsedtan city (Persian)]. Journal of Shahrekord University of Medical Sciences. 2006; 2(3):82-6.
25. Dosttar Sanaye M, Sobhani A. Pattern of drug consumption and its changes during the first trimester of pregnancy (Persian)]. Journal of Qazvin University of Medical Sciences. 2002; 5 (4) :55-61.
26. Moghadamnia A, Ghadimi R. [Self medication in common cold in people in 15-45 years in Babol city (Persian)]. Scientific Journal of Babol University of Medical Sciences. 2001; 2(1):26-32.
Send email to the article author
| Rights and permissions | |
 | This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Articles Copyright © The Author(s).
Owned by Guilan University of Medical Sciences.
Co-published by Negah Institute for Scientific Communication.
Contact Information
JHNM Office, Guilan University of Medical Sciences P.O.Box 41635-1873, Rasht, Iran
Journal Tel: +9813 33553202
Publisher Tel: +9821 453 55 555; +9821 453 55 000
Email: holisticnmj@gmail.com, nursjournal@gums.ac.ir
