Fri, Apr 26, 2024
Volume 30, Issue 1 (1-2020)
JHNM 2020, 30(1): 53-59 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Dolatpanah A, Chehrzad M M, Shafipour S Z, Atrkar Roshan Z. Effect of an Integrated Training Program on the Mothers of Children With Eating Problems. JHNM 2020; 30 (1) :53-59
URL: http://hnmj.gums.ac.ir/article-1-734-en.html
URL: http://hnmj.gums.ac.ir/article-1-734-en.html



1- Nursing (MSN), School of Nursing and Midwifery, Guilan University of Medical Sciences, Rasht, Iran
2- Instructor, Department of Nursing, Social Determinants of Health Research Center (SDHRC), Guilan University of Medical Sciences, Rasht, Iran , chehrzad@gums.ac.ir
3- Instructor, Department of Nursing, School of Nursing and Midwifery, Guilan University of Medical Sciences, Rasht, Iran
4- Associate Professor, Department of Bio-Statistics, School of Medicine, Guilan University of Medical Sciences, Rasht, Iran
2- Instructor, Department of Nursing, Social Determinants of Health Research Center (SDHRC), Guilan University of Medical Sciences, Rasht, Iran , chehrzad@gums.ac.ir
3- Instructor, Department of Nursing, School of Nursing and Midwifery, Guilan University of Medical Sciences, Rasht, Iran
4- Associate Professor, Department of Bio-Statistics, School of Medicine, Guilan University of Medical Sciences, Rasht, Iran
Full-Text [PDF 472 kb]
(647 Downloads)
| Abstract (HTML) (2547 Views)
Full-Text: (645 Views)
Introduction
Childhood is a golden opportunity for biopsychological growth and evolution in children [1]. The most important criterion for identifying child health is to examine their growth and development [2]. Meanwhile, physical growth is the most salient and tangible aspect of children’s development. Various factors affect children’s physical growth, with nutrition, as the main factor [3]. Achieving a balanced and proper diet is among the most important health objectives in children’s early years [4]. Proper eating and nutrition contributes to the sound physical growth and appearance of humans. It is also effective in the emotions, mood, behavior, and perception of individuals about their environment and the world [5].
Studies indicated a close relationship between the nutrition habits of childhood and adulthood [6]. Among the children age groups, toddler years are of great significance. In this period, the child strives to acquire independence [7]. Particularly, 12-24 months of age is the period when the consumption of different foods begins, and food habits and preferences develop [8]. Furthermore, the diminished authority of parents over children, initiation of eating alone, and use of family table, are all new events in a toddler’s life [7]. Therefore, these changes during toddlerhood demand new behaviors, especially regarding the child’s nutrition [9].
Some challenges of parents are to establish appropriate nutrition in these ages, as well as their unfamiliarity about children’s proper nutrition [3]. Eating problems occur in the early years of life, and include improper behaviors during eating (e.g. throwing the food, throwing tantrum, and dirty eating), dependence in eating, eating limited food types, rejecting foods appropriate to their age, avoiding eating, rejecting any food type, developing stress during eating [5], holding foods in mouth for a long time, vomiting, and retching [10]. These behaviors complicate feeding the child [11].
They also affect the mother-child relationship and worries the mother [5]. A mother’s awareness about developing appropriate nutritional behaviors directly affects the child’s nutritional behavior [12]. Mothers often need to be trained about children’s appropriate nutrition-related behaviors [1]. Studies on training methods introduce integrated training as one of the best and most complete teaching methods. It considers integrated training as a fundamental and comprehensive method for constant and spontaneous training. It relies on the individual interests and characteristics of the learners [13].
Integrated training has been defined as a combination of in-person and electronic approach, in which information and communication technologies are used along with in-person sessions for learning. Integrated training has been among the most extensive learning methods in the past 10 years, and provided great success and approval [14]. Integrated training is a learning model that emphasizes on learning quality and employs information and communication technologies to conduct educational planning [13]. The modification and improvement of the nutritional status of children are among the top priorities of the health system programs of the country [2].
Additionally, preventing unsuitable nutrition and interventional programs should be initiated from childhood. Accordingly, training mothers, as the main responsible caregivers for children’s nutrition is a top priority in the health educational programs. Furthermore, nurses play a key role in assisting parents to meet the needs of this age group. Therefore, this study aimed to determine the effect of integrated training on the mothers of 1-3-year-old children with eating problems.
Materials and Methods
This was a two-group (control and intervention) quasi-experimental study with a pretest-posttest design. It involved 70 mothers of 1-3-year-old children with eating problems visiting the healthcare center. Due to the need for at least thirty samples for pilot interventional studies, 35 samples were included in each study group.
Among the healthcare centers of Rasht, the urban healthcare center was purposefully selected (due to socioeconomic and cultural discrepancies among the studied units). From the visitors of this center, 70 mothers of 1-3-year-old children with eating problems were assigned into the test and control groups (each group: 35 individuals), as random blocks. The case and control groups were coded A and B, respectively.The inclusion criteria were being a mother of a 1-3-year-old child with eating problems based on the questionnaire data, at least 9 grades of educations, having a cell phone, the absence of reflux disease in the child (as expressed by the mother), the absence of brain paralysis disease and mental retardation in the child, not consuming drugs affecting appetite by the child (as stated by the mother; e.g.ciproheptadine and similar drugs), not consuming antidepressant drugs by the mother according to their verbal statement, and mother’s willingness to participate in the research.
The data collection instruments included a demographic information questionnaire and Food Preference Questionnaire (FPQ). This scale investigates eating problems among 6-36-month-old children, and is completed by mother. This questionnaire was developed by Lewinson [15], and has been translated into Persian [11]. Its Persian version has 55 yes/no statements in 5 areas, including mother’s satisfaction with eating, eating different food types, the eating behavior, stress during eating, and eating-dependence physical signs. In most statements, yes represents score 1, while “no” is dedicated a zero score. Some statements have reverse scoring. Therefore, the questionnaire provides a total score of the sum of the questions entitled eating problems along with 5 scores of subscales. Higher scores indicate the existence of eating problems.
In the present study, the reliability of instrument, using Cronbach’s alpha coefficient, was obtained as 79%. For mother’s satisfaction with child’s eating, eating behavior, stress during eating, eating different foods, and eating-dependence physical signs, the values of Cronbach’s alpha coefficient were 80%, 67%, 68%, 70%, and 55%, respectively. After receiving written informed consent froms form the mothers, the demographic information and food problems questionnaires were completed by them. Next, the integrated training program was implemented on the test group.
The design of the integrated training program for the test group was based on valid scientific resources as well as the approval of the referees and professors in the Children Nursing Department and curriculum development group, as well as the principles of educational planning, in three sessions. Two in-person sessions were held once a week on an every other week basis. The training in the first session involved presenting an educational multimedia CD. Furthermore, a text message was sent to the mothers between the training sessions (in the second week); the training was performed through sending a text message by the researcher.
The test group, if required, was able to call the researcher by phone to resolve their problems and ambiguities. The designed integrated training program included training about eating problems, the proper pattern principles of feeding, the mother behavioral approaches during eating, appetite manipulation, positive attention, inattention, and the use of reward and deprivation techniques.
The questionnaire was re-completed by the intervention and control groups immediately and one month after the training. Data analysis was performed by mean, standard deviation, frequency, Independent Samples t-test, and Chi-squared test. To determine the effect of integrated training on the eating problems among the children in the test and control groups before and immediately as well as one month after the treatment, Independent Samples t-test and Paired Samples t-test were used, after the Kolmogorov-Smirnov test confirmed the normal distribution of the obtained data. To analyze the collected data, SPSS was used.
Results
The study findings indicated that the mean±SD age of children in the test and control groups were 26.8±6.22 and 25.29±6.35 years, respectively. In the test group, 54.3% and 45.7% were boys and girls, respectively, while in the control group, the same respective percentages were 62.8 and 37.2. Chi-squared test results suggested no significant difference in the age and gender of toddlers between the test and control groups. Therefore, the toddlers of both groups were similar in terms of age and gender.
Childhood is a golden opportunity for biopsychological growth and evolution in children [1]. The most important criterion for identifying child health is to examine their growth and development [2]. Meanwhile, physical growth is the most salient and tangible aspect of children’s development. Various factors affect children’s physical growth, with nutrition, as the main factor [3]. Achieving a balanced and proper diet is among the most important health objectives in children’s early years [4]. Proper eating and nutrition contributes to the sound physical growth and appearance of humans. It is also effective in the emotions, mood, behavior, and perception of individuals about their environment and the world [5].
Studies indicated a close relationship between the nutrition habits of childhood and adulthood [6]. Among the children age groups, toddler years are of great significance. In this period, the child strives to acquire independence [7]. Particularly, 12-24 months of age is the period when the consumption of different foods begins, and food habits and preferences develop [8]. Furthermore, the diminished authority of parents over children, initiation of eating alone, and use of family table, are all new events in a toddler’s life [7]. Therefore, these changes during toddlerhood demand new behaviors, especially regarding the child’s nutrition [9].
Some challenges of parents are to establish appropriate nutrition in these ages, as well as their unfamiliarity about children’s proper nutrition [3]. Eating problems occur in the early years of life, and include improper behaviors during eating (e.g. throwing the food, throwing tantrum, and dirty eating), dependence in eating, eating limited food types, rejecting foods appropriate to their age, avoiding eating, rejecting any food type, developing stress during eating [5], holding foods in mouth for a long time, vomiting, and retching [10]. These behaviors complicate feeding the child [11].
They also affect the mother-child relationship and worries the mother [5]. A mother’s awareness about developing appropriate nutritional behaviors directly affects the child’s nutritional behavior [12]. Mothers often need to be trained about children’s appropriate nutrition-related behaviors [1]. Studies on training methods introduce integrated training as one of the best and most complete teaching methods. It considers integrated training as a fundamental and comprehensive method for constant and spontaneous training. It relies on the individual interests and characteristics of the learners [13].
Integrated training has been defined as a combination of in-person and electronic approach, in which information and communication technologies are used along with in-person sessions for learning. Integrated training has been among the most extensive learning methods in the past 10 years, and provided great success and approval [14]. Integrated training is a learning model that emphasizes on learning quality and employs information and communication technologies to conduct educational planning [13]. The modification and improvement of the nutritional status of children are among the top priorities of the health system programs of the country [2].
Additionally, preventing unsuitable nutrition and interventional programs should be initiated from childhood. Accordingly, training mothers, as the main responsible caregivers for children’s nutrition is a top priority in the health educational programs. Furthermore, nurses play a key role in assisting parents to meet the needs of this age group. Therefore, this study aimed to determine the effect of integrated training on the mothers of 1-3-year-old children with eating problems.
Materials and Methods
This was a two-group (control and intervention) quasi-experimental study with a pretest-posttest design. It involved 70 mothers of 1-3-year-old children with eating problems visiting the healthcare center. Due to the need for at least thirty samples for pilot interventional studies, 35 samples were included in each study group.
Among the healthcare centers of Rasht, the urban healthcare center was purposefully selected (due to socioeconomic and cultural discrepancies among the studied units). From the visitors of this center, 70 mothers of 1-3-year-old children with eating problems were assigned into the test and control groups (each group: 35 individuals), as random blocks. The case and control groups were coded A and B, respectively.The inclusion criteria were being a mother of a 1-3-year-old child with eating problems based on the questionnaire data, at least 9 grades of educations, having a cell phone, the absence of reflux disease in the child (as expressed by the mother), the absence of brain paralysis disease and mental retardation in the child, not consuming drugs affecting appetite by the child (as stated by the mother; e.g.ciproheptadine and similar drugs), not consuming antidepressant drugs by the mother according to their verbal statement, and mother’s willingness to participate in the research.
The data collection instruments included a demographic information questionnaire and Food Preference Questionnaire (FPQ). This scale investigates eating problems among 6-36-month-old children, and is completed by mother. This questionnaire was developed by Lewinson [15], and has been translated into Persian [11]. Its Persian version has 55 yes/no statements in 5 areas, including mother’s satisfaction with eating, eating different food types, the eating behavior, stress during eating, and eating-dependence physical signs. In most statements, yes represents score 1, while “no” is dedicated a zero score. Some statements have reverse scoring. Therefore, the questionnaire provides a total score of the sum of the questions entitled eating problems along with 5 scores of subscales. Higher scores indicate the existence of eating problems.
In the present study, the reliability of instrument, using Cronbach’s alpha coefficient, was obtained as 79%. For mother’s satisfaction with child’s eating, eating behavior, stress during eating, eating different foods, and eating-dependence physical signs, the values of Cronbach’s alpha coefficient were 80%, 67%, 68%, 70%, and 55%, respectively. After receiving written informed consent froms form the mothers, the demographic information and food problems questionnaires were completed by them. Next, the integrated training program was implemented on the test group.
The design of the integrated training program for the test group was based on valid scientific resources as well as the approval of the referees and professors in the Children Nursing Department and curriculum development group, as well as the principles of educational planning, in three sessions. Two in-person sessions were held once a week on an every other week basis. The training in the first session involved presenting an educational multimedia CD. Furthermore, a text message was sent to the mothers between the training sessions (in the second week); the training was performed through sending a text message by the researcher.
The test group, if required, was able to call the researcher by phone to resolve their problems and ambiguities. The designed integrated training program included training about eating problems, the proper pattern principles of feeding, the mother behavioral approaches during eating, appetite manipulation, positive attention, inattention, and the use of reward and deprivation techniques.
The questionnaire was re-completed by the intervention and control groups immediately and one month after the training. Data analysis was performed by mean, standard deviation, frequency, Independent Samples t-test, and Chi-squared test. To determine the effect of integrated training on the eating problems among the children in the test and control groups before and immediately as well as one month after the treatment, Independent Samples t-test and Paired Samples t-test were used, after the Kolmogorov-Smirnov test confirmed the normal distribution of the obtained data. To analyze the collected data, SPSS was used.
Results
The study findings indicated that the mean±SD age of children in the test and control groups were 26.8±6.22 and 25.29±6.35 years, respectively. In the test group, 54.3% and 45.7% were boys and girls, respectively, while in the control group, the same respective percentages were 62.8 and 37.2. Chi-squared test results suggested no significant difference in the age and gender of toddlers between the test and control groups. Therefore, the toddlers of both groups were similar in terms of age and gender.
A total of 42.85% of the mothers in the test group aged 31-35 years. Moreover, 62.8% had a high-school diploma, and 62.8% were housewives. In the control group, 37.14% of mothers aged 21-25 years. Among them, 54.3% had diploma, and 54.2% were housewives. Chi-squared test results revealed no significant difference in the age, educational level and occupation of mothers between the test and control groups.
Regarding the fathers, 45.7% of them in the test group aged 31-35 years, 40 had diploma and 48.5% had buziness. In the control group, 40% of fathers aged 26-30 years, 51.4% had diploma, and 40% had buziness. The Chi-squared test results indicated no significant difference in the age, educational level, and occupation of fathers between the two study groups.
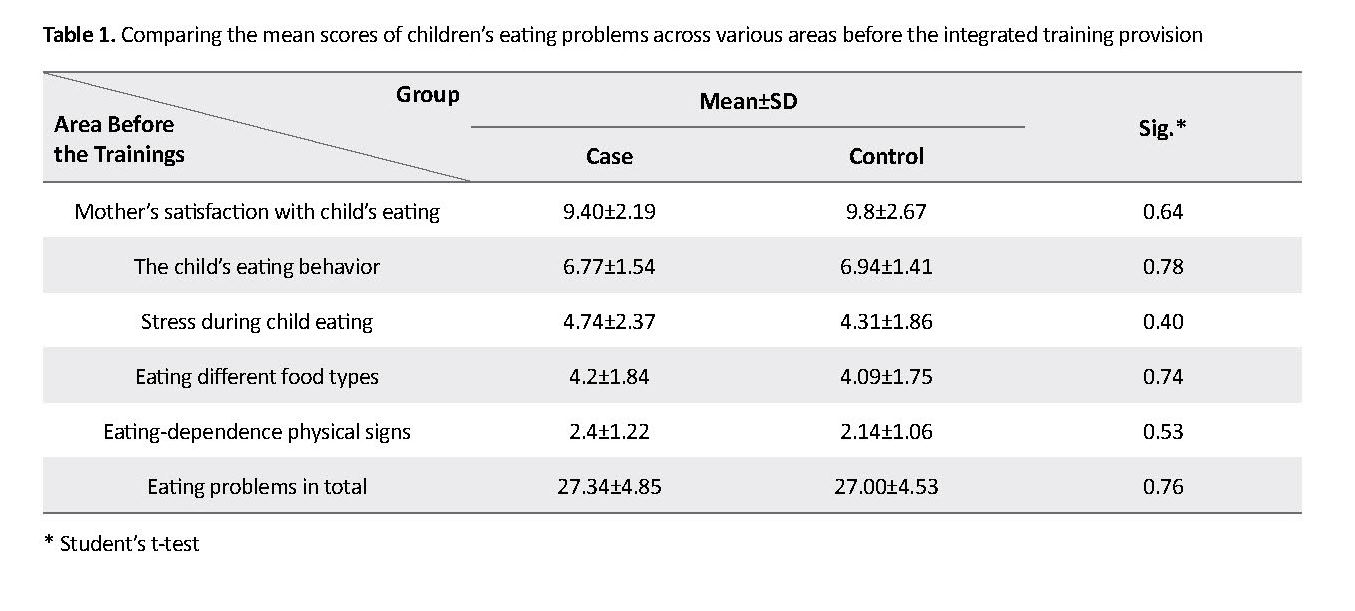
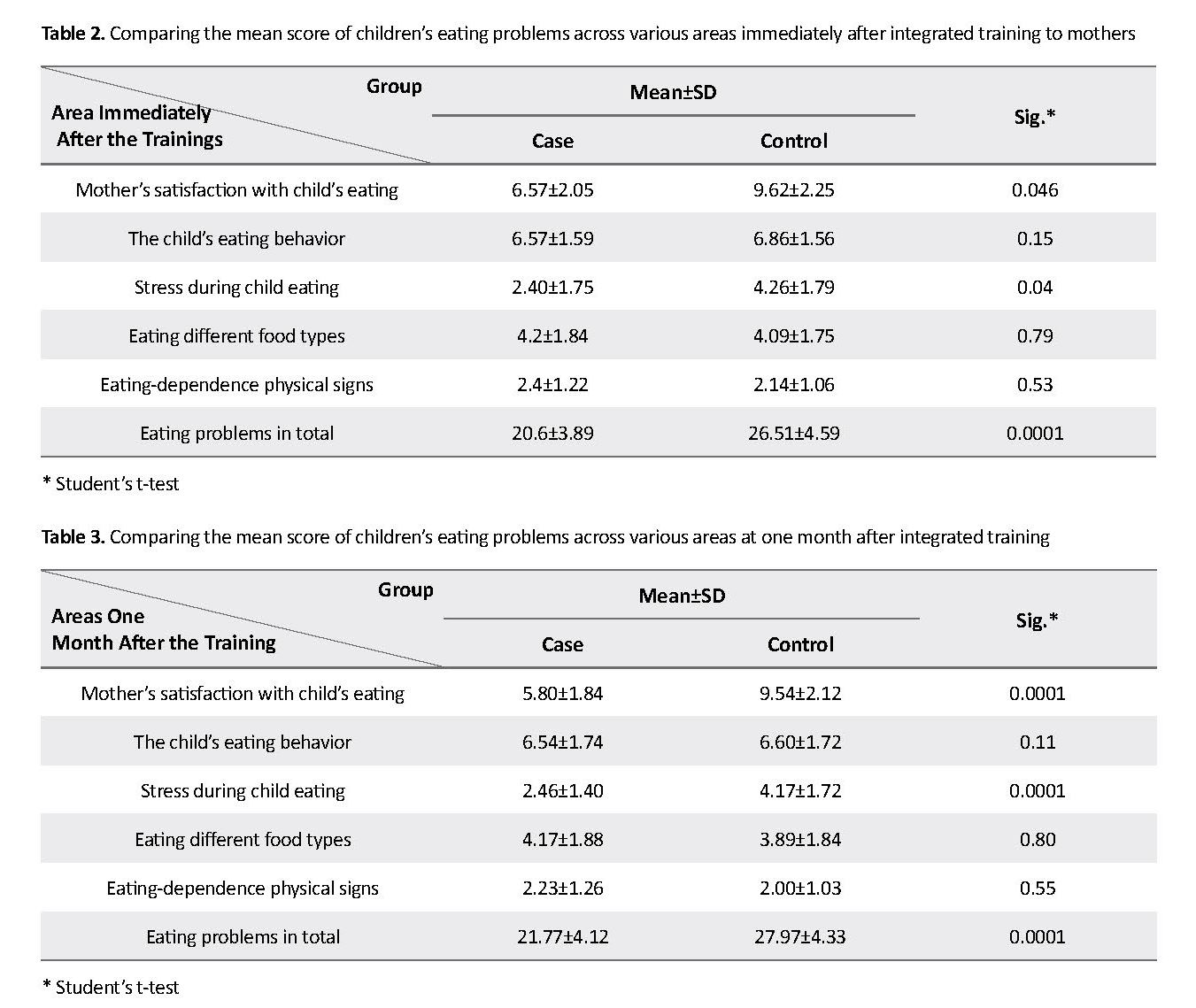
There was no significant difference in the mean score of eating problems across the studied units in various areas before conducting the integrated training (Table 1). However, a significant difference was observed in the mean score of eating problems in the domain of mother satisfaction with child eating by t-test (P=0.046), stress during child eating (P=0.04), and eating problems in total (P=0.0001) immediately after the integrated training in the intervention group. In addition, the level of eating problems significantly reduced in the intervention group (Table 2).
Regarding the fathers, 45.7% of them in the test group aged 31-35 years, 40 had diploma and 48.5% had buziness. In the control group, 40% of fathers aged 26-30 years, 51.4% had diploma, and 40% had buziness. The Chi-squared test results indicated no significant difference in the age, educational level, and occupation of fathers between the two study groups.
There was no significant difference in the mean score of eating problems across the studied units in various areas before conducting the integrated training (Table 1). However, a significant difference was observed in the mean score of eating problems in the domain of mother satisfaction with child eating by t-test (P=0.046), stress during child eating (P=0.04), and eating problems in total (P=0.0001) immediately after the integrated training in the intervention group. In addition, the level of eating problems significantly reduced in the intervention group (Table 2).
Furthermore, a significant statistical difference (by Paired t-test) was observed in the intervention group in the mean score of eating problems in mother satisfaction with child eating (P=0.0001), stress during child eating (P=0.0001), and eating problems in total (P=0.0001) one month after conducting the integrated training (Table 3).
Discussion
The present study findings indicated no significant difference between the two study groups before the training. In this regard, Baghdari et al. indicated no significant difference between the intervention and control groups before the intervention [4]. The results of our study were in line of that study. Immediately after the training, there was significant difference in the mean score of eating problems between the test and control groups.
Such difference was in terms of the mother’s satisfaction with the child’s eating, stress during eating, and eating problems in total. In this regard, the results obtained by two similar study also indicated a significant difference between the mean score of eating problems in the test and the control groups in different areas, immediately after the training [1, 16]. Another study [17] also reported that training mothers in the test group improved their nutritional knowledge and approach. Furthermore, another study [18] suggested that nutrition training provided to mothers has reduced the consumption of unhealthy and energetic foods as well as snacks by children in the test group.
One month after the training, the mean score of eating problems in the test and control groups demonstrated a significant difference in terms of mother’s satisfaction with eating, stress during eating, and eating problems in total. Inconsistent with the present study and above mentioned investigations, one study [19] revealed that after training, the dietary habits and extent of fast food consumption did not significantly differ in the children of the control and test groups. Furthermore, an experimental study [20] reported that training the mothers of toddlers with the pattern of nutritional behavior improved the consumption of some nutritious foods.
In this regard, it has been documented [4] that training mothers through group discussion and newsletter has been effective in the quality of nutrition of children, mother awareness, and the score of healthy nutrition index in the test group. However, no significant difference was observed between the newsletter recipients and discussion groups.
Providing nutrition training to mothers has improved their awareness and function and developed better dietary habits in their children. As the directly responsible person for the child’s nutrition, mother plays a significant role in developing appropriate dietary habits in children. Modifying and improving the nutritional status of children is among the top priorities of the country’s health system. In addition, preventing inappropriate nutrition and developing relevant interventional programs should begin from the childhood period. In this respect, training mother, as the main responsible caregiver for the child nutrition, is a top priority in the health education programs.
The complexity of urban life and shortage of time have limited access to educational materials, spending time, and cost to be lower than the major criteria for choice and preference of educational methods by people. An integrated training can be more effective than other educational methods to solve this issue. In spite of the training offered by healthcare centers to parents regarding children’s eating, there are eating problems, diminished anthropometric criteria, and the involvement of parents in feeding their children. Probably, by changing the training approach, one can take effective steps to mitigate this problem.
Some study limitations were telephone data collection in the third stage, as well as time limitation, and the cross-sectional nature of this research to evaluate all areas of eating problems. It is suggested that further studies be conducted with a longer time interval to investigate eating problems across all related areas. It is also suggested that studies with the concurrent presence of mother, father, and other family members be conducted to equalize the proper treatment of children during eating and to support appropriate dietary habits in children. Another limitation of the study was the follow-up duration. Thus, studies with longer follow-up periods are recommended. In addition, all study outcomes have been collected using a questionnaire and the obtained data might not be exactly accurate. Eventually, with respect to the sample size of this pilot study, it is suggested that future studies be conducted with a larger sample size.
The present study revealed that providing an integrated training to mothers can improve eating problems in their toddlers. It also resulted in diminished stress during eating and mother’s satisfaction with the child’s eating. Nutrition is highly essential during toddler years in terms of developing nutritional habits in later years. Moreover, mothers play important roles in feeding the child. Thus, by presenting a new training style, one can take an important step for the proper development of dietary habits in toddlers. Furthermore, it could promote growth and development as well as health in children.
Ethical Considerations
Compliance with ethical guidelines
This study has permission of the Ethics Committee under registration number Code: 912215 and was approved by the Research Ethics Committee of Guilan Universi-ty of Medical Sciences and registered by the Iranian Reg-istry of Clinical Trials (Code: IRCT2014121812990N5).
Funding
This paper was derived from a MSc. thesis of the first author in children nursing approved by the Research Committee of Guilan University of Medical Sciences, Rasht, Iran. also This work was financially supported by Guilan University of Medical Sciences.
Authors contributions
The study plan: Akram Dolatpanah and Minoo Mitra Chehrzad; Manuscript drafting: Seyedeh Zahra Shafipour; The essential revision: Zahra Atrkar Roshan.
Conflict of interest
The authors declared no conflicts of interest.
Acknowledgements
The authors highly appreciate the support of the Social Determinants of Health Research Center (SDHRC), Guilan University of Medical Sciences, and the faculty members of the Nursing Department at Guilan Univercity of Medical Sciences, as well as the employees of the urban healthcare center.
References
Salvati Ghasemi Sh, Cheragui F, Hasan Tehrani T, Moghimbeigi A. [The effect of mothers’ feeding behavior education on eating habits of their toddler children in Hamadan kindergartens (Persian)]. Iranian Journal of Pediatric Nursing. 2015; 2(2):68-79.
Kliegman RM, Stanton B, J St. Geme, Schor NF. Nelson textbook of pediatrics. 20th Ed. Elsevier Health Sciences: London; 2015.
Hockenberry M, Wilson D. Wong's essentials of pediatric nursing. 9th Ed. St. Louis: Mosby; 2012.
Baghdari N, Bahrami Morghmaleki A, Norozi A, Karimi Monghi H. [Comparison of the effect of mathernal education via newsletter and group discussion on the nutritional quality of preschoolers (Persian)]. Evidence Based Care. 2014; 3(4):75-84.
Zeinali Sh. [Investigating the efficacy of parent management training in reducing children’s feeding problems (Persian)] [MSc. thesis]. Tehran: Shahid Beheshti University; 2011.
Oliveira A, Jones L, de Lauzon-Guillain B, Emmett P, Moreira P, Charles MA, et al. Early problematic eating behaviours are associated with lower fruit and vegetable intake and less dietary variety at 4-5 years of age. A prospective analysis of three European birth cohorts. British Journal of Nutrition. 2015; 114(5):763-71. [DOI:10.1017/S0007114515002287] [PMID]
Hockenberry MJ, Wilson D. Wong's Nursing Care of Infants and Children Multimedia Enhanced Version. 9th ed. Philadelphia: Elsevier Health Sciences; 2015.
Birch LL, Doub AE. Learning to eat: Birth to age 2 y. The American Journal of Clinical Nutrition. 2014; 99(3):723S-8S. [DOI:10.3945/ajcn.113.069047] [PMID]
Kral TV, Rauh EM. Eating behaviors of children in the context of their family environment. Physiology & Behavior. 2010; 100(5):567-73. [DOI:10.1016/j.physbeh.2010.04.031] [PMID] [PMCID]
Örün E, Erdil Z, Çetinkaya S, Tufan N, Yalçın S. Problematic eating behavior in Turkish children aged 12-72 months: Characteristics of mothers and children. Central European Journal of Public Health. 2012; 20(4):257-61. [DOI:10.21101/cejph.a3748]
Zeinali Sh, Mazaheri MA, Sadeghi MS, Jabari M. [The relationships of mother’s attachment to infant and mothers’ psychological characteristics to feeding problem in infants (Persian)]. Journal of Developmental Psychology: Iranian Psychologists. 2011; 8(29):55-66.
Sobko T, Tse M, Kaplan M. A randomized controlled trial for families with preschool children - promoting healthy eating and active playtime by connecting to nature. BMC Public Health. 2016; 16:505. [DOI:10.1186/s12889-016-3111-0] [PMID] [PMCID]
Jafari M. [Comparison of lecture and blended teaching methods on learning and satisfaction of medical students in biochemistry course (Persian)]. Iranian Journal of Medical Education. 2012; 12(7):488-97.
Khazaei Sh, Rashedi E, Barati E. [Approaches of at modulative education in medical sciences: A review (Persian)]. Pajouhan Scientific Journal. 2012; 11(1):6-11.
Lewinsohn PM, Holm-Denoma JM, Gau JM, Joiner TE, Striegel-Moore R, Bear P, et al. Problematic eating and feeding behaviors of 36-month-old children. International Journal of Eating Disorders. 2005; 38(3):208-19. [DOI:10.1002/eat.20175] [PMID] [PMCID]
Hamel LM, Robbins LB. Computer-and web-based interventions to promote healthy eating among children and adolescents: A systematic review. Journal of Advanced Nursing. 2013; 69(1):16-30. [DOI:10.1111/j.1365-2648.2012.06086.x] [PMID] [PMCID]
Fahmida U, Kolopaking R, Santika O, Sriani S, Umar J, Htet MK, et al. Effectiveness in improving knowledge, practices, and intakes of “key problem nutrients” of a complementary feeding intervention developed by using linear programming: Experience in Lombok, Indonesia. American Journal of Clinical Nutrition. 2015; 101(3):455-61. [DOI:10.3945/ajcn.114.087775] [PMID]
Hu C, Ye D, Li Y, Huang Y, Li L, Gao Y, et al. Evaluation of a kindergarten-based nutrition education intervention for pre-school children in China. Public Health Nutrition. 2010; 13(2):253-60. [DOI:10.1017/S1368980009990814] [PMID]
Gao Y, Huang Y, ZhangY, Liu F, Feng CX, Liu T, et al. Evaluation of fast food behavior in pre-school children and parents following a one-year intervention with nutrition education. International Journal of Environmental Research and Public Health. 2014; 11(7):6780-90. [DOI:10.3390/ijerph110706780] [PMID] [PMCID]
Sadat Hosseini A, Samiee S, Razaghee N. [The effect of nutritional behavior pattern education to toddler mothers on the nutritional pattern improvement of toddlers & mothers performance (Persian)]. Journal of Hayat. 2008; 13(4):33-44.
Discussion
The present study findings indicated no significant difference between the two study groups before the training. In this regard, Baghdari et al. indicated no significant difference between the intervention and control groups before the intervention [4]. The results of our study were in line of that study. Immediately after the training, there was significant difference in the mean score of eating problems between the test and control groups.
Such difference was in terms of the mother’s satisfaction with the child’s eating, stress during eating, and eating problems in total. In this regard, the results obtained by two similar study also indicated a significant difference between the mean score of eating problems in the test and the control groups in different areas, immediately after the training [1, 16]. Another study [17] also reported that training mothers in the test group improved their nutritional knowledge and approach. Furthermore, another study [18] suggested that nutrition training provided to mothers has reduced the consumption of unhealthy and energetic foods as well as snacks by children in the test group.
One month after the training, the mean score of eating problems in the test and control groups demonstrated a significant difference in terms of mother’s satisfaction with eating, stress during eating, and eating problems in total. Inconsistent with the present study and above mentioned investigations, one study [19] revealed that after training, the dietary habits and extent of fast food consumption did not significantly differ in the children of the control and test groups. Furthermore, an experimental study [20] reported that training the mothers of toddlers with the pattern of nutritional behavior improved the consumption of some nutritious foods.
In this regard, it has been documented [4] that training mothers through group discussion and newsletter has been effective in the quality of nutrition of children, mother awareness, and the score of healthy nutrition index in the test group. However, no significant difference was observed between the newsletter recipients and discussion groups.
Providing nutrition training to mothers has improved their awareness and function and developed better dietary habits in their children. As the directly responsible person for the child’s nutrition, mother plays a significant role in developing appropriate dietary habits in children. Modifying and improving the nutritional status of children is among the top priorities of the country’s health system. In addition, preventing inappropriate nutrition and developing relevant interventional programs should begin from the childhood period. In this respect, training mother, as the main responsible caregiver for the child nutrition, is a top priority in the health education programs.
The complexity of urban life and shortage of time have limited access to educational materials, spending time, and cost to be lower than the major criteria for choice and preference of educational methods by people. An integrated training can be more effective than other educational methods to solve this issue. In spite of the training offered by healthcare centers to parents regarding children’s eating, there are eating problems, diminished anthropometric criteria, and the involvement of parents in feeding their children. Probably, by changing the training approach, one can take effective steps to mitigate this problem.
Some study limitations were telephone data collection in the third stage, as well as time limitation, and the cross-sectional nature of this research to evaluate all areas of eating problems. It is suggested that further studies be conducted with a longer time interval to investigate eating problems across all related areas. It is also suggested that studies with the concurrent presence of mother, father, and other family members be conducted to equalize the proper treatment of children during eating and to support appropriate dietary habits in children. Another limitation of the study was the follow-up duration. Thus, studies with longer follow-up periods are recommended. In addition, all study outcomes have been collected using a questionnaire and the obtained data might not be exactly accurate. Eventually, with respect to the sample size of this pilot study, it is suggested that future studies be conducted with a larger sample size.
The present study revealed that providing an integrated training to mothers can improve eating problems in their toddlers. It also resulted in diminished stress during eating and mother’s satisfaction with the child’s eating. Nutrition is highly essential during toddler years in terms of developing nutritional habits in later years. Moreover, mothers play important roles in feeding the child. Thus, by presenting a new training style, one can take an important step for the proper development of dietary habits in toddlers. Furthermore, it could promote growth and development as well as health in children.
Ethical Considerations
Compliance with ethical guidelines
This study has permission of the Ethics Committee under registration number Code: 912215 and was approved by the Research Ethics Committee of Guilan Universi-ty of Medical Sciences and registered by the Iranian Reg-istry of Clinical Trials (Code: IRCT2014121812990N5).
Funding
This paper was derived from a MSc. thesis of the first author in children nursing approved by the Research Committee of Guilan University of Medical Sciences, Rasht, Iran. also This work was financially supported by Guilan University of Medical Sciences.
Authors contributions
The study plan: Akram Dolatpanah and Minoo Mitra Chehrzad; Manuscript drafting: Seyedeh Zahra Shafipour; The essential revision: Zahra Atrkar Roshan.
Conflict of interest
The authors declared no conflicts of interest.
Acknowledgements
The authors highly appreciate the support of the Social Determinants of Health Research Center (SDHRC), Guilan University of Medical Sciences, and the faculty members of the Nursing Department at Guilan Univercity of Medical Sciences, as well as the employees of the urban healthcare center.
References
Salvati Ghasemi Sh, Cheragui F, Hasan Tehrani T, Moghimbeigi A. [The effect of mothers’ feeding behavior education on eating habits of their toddler children in Hamadan kindergartens (Persian)]. Iranian Journal of Pediatric Nursing. 2015; 2(2):68-79.
Kliegman RM, Stanton B, J St. Geme, Schor NF. Nelson textbook of pediatrics. 20th Ed. Elsevier Health Sciences: London; 2015.
Hockenberry M, Wilson D. Wong's essentials of pediatric nursing. 9th Ed. St. Louis: Mosby; 2012.
Baghdari N, Bahrami Morghmaleki A, Norozi A, Karimi Monghi H. [Comparison of the effect of mathernal education via newsletter and group discussion on the nutritional quality of preschoolers (Persian)]. Evidence Based Care. 2014; 3(4):75-84.
Zeinali Sh. [Investigating the efficacy of parent management training in reducing children’s feeding problems (Persian)] [MSc. thesis]. Tehran: Shahid Beheshti University; 2011.
Oliveira A, Jones L, de Lauzon-Guillain B, Emmett P, Moreira P, Charles MA, et al. Early problematic eating behaviours are associated with lower fruit and vegetable intake and less dietary variety at 4-5 years of age. A prospective analysis of three European birth cohorts. British Journal of Nutrition. 2015; 114(5):763-71. [DOI:10.1017/S0007114515002287] [PMID]
Hockenberry MJ, Wilson D. Wong's Nursing Care of Infants and Children Multimedia Enhanced Version. 9th ed. Philadelphia: Elsevier Health Sciences; 2015.
Birch LL, Doub AE. Learning to eat: Birth to age 2 y. The American Journal of Clinical Nutrition. 2014; 99(3):723S-8S. [DOI:10.3945/ajcn.113.069047] [PMID]
Kral TV, Rauh EM. Eating behaviors of children in the context of their family environment. Physiology & Behavior. 2010; 100(5):567-73. [DOI:10.1016/j.physbeh.2010.04.031] [PMID] [PMCID]
Örün E, Erdil Z, Çetinkaya S, Tufan N, Yalçın S. Problematic eating behavior in Turkish children aged 12-72 months: Characteristics of mothers and children. Central European Journal of Public Health. 2012; 20(4):257-61. [DOI:10.21101/cejph.a3748]
Zeinali Sh, Mazaheri MA, Sadeghi MS, Jabari M. [The relationships of mother’s attachment to infant and mothers’ psychological characteristics to feeding problem in infants (Persian)]. Journal of Developmental Psychology: Iranian Psychologists. 2011; 8(29):55-66.
Sobko T, Tse M, Kaplan M. A randomized controlled trial for families with preschool children - promoting healthy eating and active playtime by connecting to nature. BMC Public Health. 2016; 16:505. [DOI:10.1186/s12889-016-3111-0] [PMID] [PMCID]
Jafari M. [Comparison of lecture and blended teaching methods on learning and satisfaction of medical students in biochemistry course (Persian)]. Iranian Journal of Medical Education. 2012; 12(7):488-97.
Khazaei Sh, Rashedi E, Barati E. [Approaches of at modulative education in medical sciences: A review (Persian)]. Pajouhan Scientific Journal. 2012; 11(1):6-11.
Lewinsohn PM, Holm-Denoma JM, Gau JM, Joiner TE, Striegel-Moore R, Bear P, et al. Problematic eating and feeding behaviors of 36-month-old children. International Journal of Eating Disorders. 2005; 38(3):208-19. [DOI:10.1002/eat.20175] [PMID] [PMCID]
Hamel LM, Robbins LB. Computer-and web-based interventions to promote healthy eating among children and adolescents: A systematic review. Journal of Advanced Nursing. 2013; 69(1):16-30. [DOI:10.1111/j.1365-2648.2012.06086.x] [PMID] [PMCID]
Fahmida U, Kolopaking R, Santika O, Sriani S, Umar J, Htet MK, et al. Effectiveness in improving knowledge, practices, and intakes of “key problem nutrients” of a complementary feeding intervention developed by using linear programming: Experience in Lombok, Indonesia. American Journal of Clinical Nutrition. 2015; 101(3):455-61. [DOI:10.3945/ajcn.114.087775] [PMID]
Hu C, Ye D, Li Y, Huang Y, Li L, Gao Y, et al. Evaluation of a kindergarten-based nutrition education intervention for pre-school children in China. Public Health Nutrition. 2010; 13(2):253-60. [DOI:10.1017/S1368980009990814] [PMID]
Gao Y, Huang Y, ZhangY, Liu F, Feng CX, Liu T, et al. Evaluation of fast food behavior in pre-school children and parents following a one-year intervention with nutrition education. International Journal of Environmental Research and Public Health. 2014; 11(7):6780-90. [DOI:10.3390/ijerph110706780] [PMID] [PMCID]
Sadat Hosseini A, Samiee S, Razaghee N. [The effect of nutritional behavior pattern education to toddler mothers on the nutritional pattern improvement of toddlers & mothers performance (Persian)]. Journal of Hayat. 2008; 13(4):33-44.
Article Type : Research |
Subject:
General
Received: 2019/10/13 | Accepted: 2019/12/2 | Published: 2020/01/1
Received: 2019/10/13 | Accepted: 2019/12/2 | Published: 2020/01/1
Send email to the article author
| Rights and permissions | |
 | This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Articles Copyright © The Author(s).
Owned by Guilan University of Medical Sciences.
Co-published by Negah Institute for Scientific Communication.
Contact Information
JHNM Office, Guilan University of Medical Sciences P.O.Box 41635-1873, Rasht, Iran
Journal Tel: +9813 33553202
Publisher Tel: +9821 453 55 555; +9821 453 55 000
Email: holisticnmj@gmail.com, nursjournal@gums.ac.ir
