Thu, Apr 25, 2024
Volume 29, Issue 2 (4-2019)
JHNM 2019, 29(2): 82-89 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Nasirizad Moghadam K, Reza Masouleh S, Chehrzad M M, Kazemnezhad Leili E. The Mental Workload and Its Correlated Factors in Nurses Working in Intensive Care Units. JHNM 2019; 29 (2) :82-89
URL: http://hnmj.gums.ac.ir/article-1-694-en.html
URL: http://hnmj.gums.ac.ir/article-1-694-en.html
Kolsoom Nasirizad Moghadam1 

 , Shademan Reza Masouleh * 2, Minoo Mitra Chehrzad3 , Ehsan Kazemnezhad Leili4
, Shademan Reza Masouleh * 2, Minoo Mitra Chehrzad3 , Ehsan Kazemnezhad Leili4
, Shademan Reza Masouleh * 2, Minoo Mitra Chehrzad3 , Ehsan Kazemnezhad Leili4
1- Nursing (MSN), School of Nursing and Midwifery, Guilan University of Medical Sciences, Rasht, Iran.
2- Instructor, Department of Nursing, School of Nursing and Midwifery, Social Determinants of Health Research Center (SDHRC), Guilan University of Medical Sciences, Rasht, Iran. , srezamasouleh@gmail.com
3- Instructor, Department of Nursing, School of Nursing and Midwifery, Social Determinants of Health Research Center (SDHRC), Guilan University of Medical Sciences, Rasht, Iran.
4- Associate Professor, Social Determinants of Health Research Center (SDHRC), Bio-Statistics, Guilan University of Medical Sciences, Rasht, Iran.
2- Instructor, Department of Nursing, School of Nursing and Midwifery, Social Determinants of Health Research Center (SDHRC), Guilan University of Medical Sciences, Rasht, Iran. , srezamasouleh@gmail.com
3- Instructor, Department of Nursing, School of Nursing and Midwifery, Social Determinants of Health Research Center (SDHRC), Guilan University of Medical Sciences, Rasht, Iran.
4- Associate Professor, Social Determinants of Health Research Center (SDHRC), Bio-Statistics, Guilan University of Medical Sciences, Rasht, Iran.
Full-Text [PDF 526 kb]
(1149 Downloads)
| Abstract (HTML) (3177 Views)
Discussion
In the current study, the Mean±SD MW of ICU nurses was reported 70.21±12.4. In the studies of Hoonakker et al. [2], Zakerian et al. [3], and Malekpour et al. [16], the mean MW was higher, while Giahi et al. [5] and Sarsangi et al. [10] reported lower values compared with those of the current study. All the mentioned studies used the same study tools like ours. Every occupation has a specific mean of MW, and the obtained results indicate the existence of MW in the nursing profession, especially in the ICUs, which can be due to the nature of this profession and the work environment of the nurses.
Another point to consider is that in the current study, the mental workload was studied and not the workload. Hence, the nurses that reported high mental workload may not necessarily have a high workload. Their high mental workload may be due to their perceptions or the psychological state and familial conflicts as well as their personality. Regarding the comparison of MW dimensions, it was revealed that the dimension of “physical demand” had the highest weight, rate, and scores compared with other dimensions. In the study by Malekpour et al. [16], the dimension of frustration had the highest weight, while in the study by Kazemi et al. [9], it was the mental demand dimension, and in the studies by Sarsangi et al. [10] and Zakerian et al. [3], dimension of effort had the highest weight. Regarding the rate of dimensions, Kazemi et al. showed that frustration had the highest rate values and other studies reported no results about the rates and scores of MW dimensions.
This difference between the results of the current study and those of similar studies may be related to different environmental conditions, sampling, and implementation. For example, in the current study, the MW of nurses was investigated in three separate work shifts using its average value for comparison, while in the mentioned studies it was examined in one work shift. Obviously, examining an MW variable in three work shifts increases the likelihood of obtaining more accurate results. It is possible that factors outside the workplace influence MW and its subscales.
Results of the current study also showed that MW had a significant association with the age factor in ICU nurses where nurses aged less than 30 years had the highest MW level and the ones more than 40 years had the lowest MW scores. It was consistent with the findings of Kazemi et al. [9] and Sarsangi et al. [10] reporting a significant correlation between MW and age. In the study by Kazemi et al. the age group of 22-30 years had the lowest MW level and the age group of >50 years showed the highest MW scores. However, in the study by Hoonakker et al. [2] no significant difference was reported between MW and age factor except in physical demand dimension.
Malekpour et al. [16] reported no significant correlation between them, either. Since studies show a significant relationship between MW and occupational stress [17, 18], probably with increasing age, due to increased control over the environment and working conditions, many occupational stresses are eliminated, and as a result, the MW level decreases. On the other hand, due to the nature of the nursing profession and the work environment of the nurses, long-term nursing is a tedious and stressful job and increases the MW of older nurses, which justifies the results of studies inconsistent with the current study results.
Based on the results of the current study, MW of ICU nurses had a significant relationship with the type of ICU, where the nurses of general ICU of hospital No.3 and cardiac surgery ICU had the highest and lowest MW levels, respectively. In the study by Hoonakker et al. [2] among adult ICU, internal/surgical ICU, burn unit, neurosurgical ICU, neonatal ICU, pediatric ICU, cardiac ICU, and surgical ICU, nurses of adult and cardiac ICUs had higher MW than the ones in neurosurgical and neonatal ICUs. The difference in MW of nurses in various types of ICUs can be due to the type of hospitalized patients, as well as internal rules regarding the allocation of manpower and the number of patients in such sectors.
In the current study, the nurse-to-patient ratio in surgical ICU was 1:1 and the shift manager was not responsible for the care of any patient, while in general ICU the ratio was 1:2 and 1:3 and the shift manager, in addition to direct patient care, was responsible for managerial tasks. Clearly, with the increase in the number of patients under the care and managerial tasks, the responsibility of nurses becomes heavier, which can increase their MW in this section.
The current study found no significant association between MW and the type of work shift. Malekpour et al. [16] reported a higher MW level in the evening and night shifts compared to morning and rotating shifts. In the study by Hoonakker et al. a significant difference was observed between MW and type of work shift where nurses of 12-h shifts (day and night) had a higher overall workload, physical demands, and frustration compared with those of an 8-h shift (morning or evening). Overall workload, temporal demands, and efforts were higher in 12-h day-shifts than in 12-h night shifts. Sarsangi et al. [10] also reported a significant correlation between MW and work shift. This inconsistency in results may be due to the difference in the sampling method.
A significant association was reported in the current study between MW of ICU nurses and the number of patients under their care in each work shift, in such a way that with the increase in their number, MW of nurses increased. It was in agreement with the results of Kazemi et al. [9] and Malekpour et al. [16]. Regarding this finding, it can be explained that as the number of patients under care increases, the responsibilities and hence MW of nurses increases.
According to the results of the current study, MW of nurses in the ICU of hospital No. 1 was high. According to the significant relationship between MW and the type of ICU, the age of nurses, and the number of patients under care in each shift, and the effect of intra-sectoral and intra-hospital rules on MW, it is necessary to employ interventional strategies to reduce the MW level in this group. In units with higher MW, the number of patients under the care of each nurse should be reduced by appropriate distribution of human resources. Since the MW has a significant relationship with occupational stress [17, 18], with proper training, especially in younger staff (who has fewer skills to overcome stressful factors in the workplace), many tensions and consequently mental workload can be reduced in nurses, and the effects of excessive mental workload on nurses and patients can be prevented.
Uncontrolled mental status and familial conflicts of nurses during filling in the questionnaires and their personality type were among the limitations of the current study. It should also be considered that the current study evaluated the mental workload of the ICU nurses and not their workload. Therefore, the subjects that reported a high mental workload may not necessarily have a high workload, and their high mental workload may be due to their perceptions.
Ethical Considerations
Compliance with ethical guidelines
The current study was approved by the Social Determinants of Health Research Center of Guilan University of Medical Sciences (Registration No. 94070714) and also the Ethics Committee of the University (Ethical code: IR.GUMS.REC.1394.286).
Funding
This study was financially supported by Guilan University of Medical Sciences.
Authors contributions
Conceptualization and supervision: Shadman Reza Masule, Mino Mitra Chehrzad; Conceptualization and data analysis: Ehsan Kazemi Nejhad Leili; and Contributing to all stages of research implementation: Kolsom Nasirizad Moghadam.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgements
Authors would like to thank the Deputy of Research and Technology of the Guilan University of Medical Sciences.
References
Quinn LW. Throughput and nurses’ workloads: influences on nurse and patient outcomes [PhD. dissertation]. Philadelphia, Pennsylvania: University of Pennsylvania; 2013.
Hoonakker P, Carayan P, Gurses A, Brown R, McGuire K, Khunlertkit A, et al. Measuring workload of ICU nurses with a questionnaire survey: The NASA task Load Index. IISE Transactions on Healthcare Systems Engineering. 2011; 1(2):131-43. [DOI:10.1080/19488300.2011.609524] [PMID] [PMCID]
Zakerian A, Abasi Nia M, Mohammadin F, Fathi A, Rahmani A, Ahmadnezhad I, et al. [The relationship between workload and quality of life among hospital staffs (Persian)]. Journal of Ergonomics. 2013; 1(1):43-56.
Myny D, Van Heck A, De Bacquer D, Verhaeeghe S, Gobert M, Defloor T, et al. Determining a set of measurable and relevant factors affecting nursing workload in the acute care hospital setting: A cross sectional study. International Journal of Nursing Studies. 2012; 2012(49):427-36. [DOI:10.1016/j.ijnurstu.2011.10.005] [PMID]
Giahi O, Darvishi E, Akbarzadeh M, Shahsavari S. [Assessment of the relationship of the risk of subjective work load to musculoskeletal disorders in bank staff in Kurdistan Province (Persian)]. Scientific Journal of Kurdistan University of Medical Sciences. 2014; 19(4):36-45.
Galy E, Paxion J, Berthelon C. Measuring mental workload with the NASA-TLX needs to examine each dimension rather than relying on the global score: An example with driving. Ergonomics. 2018; 61(4):517-27. [DOI:10.1080/00140139.2017.1369583] [PMID]
Ozkan A, Ozdevecioglu M, Kaga Y, Ozsahin Koc F. Effect of mental workloads on depression-anger symptoms and interpersonal sensitivities of accounting professionals. Revista de Contabilidad- Spanish Accounting Review. 2015; 18(2):194-99. [DOI:10.1016/j.rcsar.2014.06.005]
Safari S, Akbari J, Kazemi M, AminMououdi M, Mahaki B. Personnel’s health surveillance at work: Effect of age, Body Mass Index, and shift work on mental workload and work ability index. Hindawi Publishing Corporation Journal of Environmental and Public Health. 2013; 2013:289498. [DOI:10.1155/2013/289498] [PMID] [PMCID]
Safari Sh, Mohammadi Bolban Abadi H, Kazemi M. [Evaluation mental work load in nursing critical care unit with National Aeronautics and Space Administration Task Load Index (NASATLX) (Persian)]. Health System Research Journal. 2013; 9(6):613-9.
Sarsangi V, Saberi H, Hannani M, Honarjoo F, Salim Abadi M, Goroohi M, et al. [Mental workload and its affected factors among nurses in Kashan Province during 2014 (Persian)]. Journal of Rafsanjan University of Medical Sciences. 2015; 14(1):25-36.
Young G, Zavelina L, Hooper V. Assessment of workload using NASA task load index in Perianesthesia nursing. Journal of PeriAnesthesia Nursing. 2008; 23(2):102-10. [DOI:10.1016/j.jopan.2008.01.008] [PMID]
Mohammadi M, Mazlomi A, Nasl Seraji J, Zeraati h. [Designing questionnaire of assessing mental workload and determine its validity and reliability among ICUs nurses in one of the TUMS’s hospitals (Persian)]. Scientific Journal of School of Public Health and Institute of Public Health Research. 2012; 11(2):87-96.
Kamfiruzi A. National aeronautics and space administration task load index [Internet]. 2019 [Updated 2019 March 6]. Available from: http://humansystems.arc.nasa.gov/groups/tlx/computer.php .http://earmin.com/nasa-tlx-fa/
Khandan M, Roshan Zamir S, Maghsoudipour M. [Survey of workload and job satisfaction relationship in a heavy mental manufacturing company (Persian)]. Iran Occupational Health. 2012; 9(1):30-6.
Tubbs-Cooley HL, Mara CA, Carle AC, Gurses AP. The NASA Task Load Index as a measure of overall workload among neonatal, paediatric and adult intensive care nurses. Intensive and Critical Care Nursing. 2018; 46:64-9. [DOI:10.1016/j.iccn.2018.01.004] [PMID]
Malekpour F, Mohammadian Y, Malekpour A, Mohammadpour Y, Sheikh Ahmadi A, Shakarami A. [Assessment of mental workload in nursing by using NASA-TLX (Persian)]. Journal of Urmia Nursing and Midwifery Faculty. 2014; 11(11):892-9.
Gholam Nejad H, Nikpeyma N. [Occupational stressors in nursing (Persian)]. Iran Occupational Health. 2009; 6(1):22-7.
Bahrami A, Akbari H, Mousavi G, Hannani M, Ramezani Y. [Job stress among the nursing staff of Kashan hospital (Persian)]. Feyz. 2011; 15(4):366-73.
Full-Text: (1543 Views)
Introduction
In the past two decades, the intensity of nursing care and nursing workload increased due to the increased patients’ awareness and reduced hospitalization stay [1]. The increased workload is one of the most important concerns in healthcare and especially in Intensive Care Units (ICUs) that can have a negative impact on nurses and patients [2]. The workload is one of the influential factors on patient’s safety and the quality of nursing care [3]. Nowadays, because of the advancement of modern technology, work environments have changed, and as a result, many of them impose more cognitive needs compared to the physical needs of individuals. Therefore, depending on the type of profession, there is a concept called “mental workload” used in Ergonomics as a general concept. Nursing is one of the professions where this concept can be used. The workload is not limited to the physical tasks of nurses; their cognitive tasks (mental workload) are also a complex part of the overall workload of nurses [3, 4].
Although there is no universally accepted definition of Mental Workload (MW), and it is often considered by analogy to the physical workload [5, 6], it can be said that MW refers to all mental activities such as estimation, decision making, communication, identification and search, and is defined as the relationship between the mental resources required to perform a task and the ability of individuals to use these resources. MW is a subjective concept, which cannot be measured directly or be considered an absolute value. However given that the human mind can process the information at a limited rate, then MW is the percentage of the capacity used at any time point [7].
It is simply the amount of mental effort that one puts into a task [5, 8, 9], and requires actions such as concentration, reminder, decision making, and attention [8], and is essentially related to the individual’s mental abilities and how the information is received and processed, and at the end leads to decision making and action [5]. In other words, MW is a level of cognitive need or an analytical effort required by an individual to fulfill the physical, spatial, and environmental demands of a specific task [10].
Various studies show that in professions where MW is high, due to fatigue and inappropriate scheduling, the efficiency decreases, which reduces memory, damages the thinking process, causes irritability, and reduces learning [11, 12]. Tired people are more likely to choose risky behaviors such as doing shortcuts to perform tasks [12]. Nurses working in specific departments, such as ICUs, are subject to severe MW since they are always making important decisions that relate to the lives of patients. On the other hand, ICU nurses should be continuously responsive to the needs of their patients or the patients’ companions and are usually faced with the most severe emotional aspects of patients [12]. Accordingly, Hoonakker et al. [2] study results indicate high MW among ICU nurses.
Increased MW is reported as a major source of stress and burnout in nurses, which can have direct and indirect impacts on nurses and patients. Its direct impacts on patient care may be related to the insufficient time for caring duties, which increases the mortality rate of patients. Its indirect impacts on patient’s safety are via affecting communication, reducing job satisfaction and motivation, and causing burnout in nurses [10]. MW is associated with depression, anger, and interpersonal sensitivities [7]. Since MW has a direct relationship with the person’s performance and is one of the factors affecting the health, safety, and comfort of individuals, the concept of MW and its effects are one of the main topics of organizational behavior [10]. In this regard, the current study aimed at evaluating MW and its related factors in nurses working in the ICUs.
Materials and Methods
The current analytical study with the cross-sectional design was conducted in 2015 on 105 nurses working in ICUs of educational and medical centers in Rasht City, Iran. They were selected using the census method from nurses working in five ICUs in Rasht who have at least a BS degree and one year of experience. To collect data, a two-part questionnaire was used. The first part included individual and occupational characteristics of the study subjects (gender, age, marital status, work experience, education, type of ICU, number of patients under care, weekly working hours, working shift, resting period before and after the work shift, and working at the other centers). The second part was the National Aeronautics and Space Administration-Task Load Index (NASA-TLX) [2, 13].
It is one of the known tools to evaluate the MW from the individual point of view developed by Hart in 1998 at NASA’s Ames Research Center to measure subjective workload in aircraft simulation, and then extended by the Human Performance Group at NASA by conducting more than 40 experiments in three years. It is employed in more 550 research studies and recently used in many other professions, including healthcare [2, 14, 15].
Different studies verified the validity and reliability of this tool [2, 14]. Validity and reliability of its Persian version were verified in special units by Mohammadi et al. [12]. It has six subscales of mental demand, physical demand, temporal demand, performance, effort, and frustration. Each task is scored within a 100-point range based on a 5-point style. After reading descriptions for each scale, nurses give a score to each one from 0 to 100. This step is called “weighting”. In the next step, called “rating”, there are 15 two-choice items and individuals should choose the factor that plays the most important role in each item.
The weighted score is multiplied by the rated score and then divided by 15 to get an MW score for each subscale. By summing subscale scores, total MW score is obtained. This tool is compared and interpreted based on the mean difference between different groups (e.g. between hospitals, units, or staff). The group with the highest mean is reported to have a higher MW related to other groups.
The method of calculating the mental load of work can be performed either manually or with the help of NASA’s application [13]. In the current study, a portion of the information was calculated through the application and partly performed manually. Each questionnaire received a specific code. Since each nurse had to be examined in three work shifts, according to the monthly program of each unit, the next work shift of each nurse was found out and the necessary arrangements were made with the nurses to attend the study. Written informed consent was obtained from all participants.
To determine the MW score, first, the MW data of each nurse was transferred into the software and the weight and rate of the load for 6 subscales and the total MW score were calculated. Since the software does not give the MW score for each of the subscales, their scores were manually multiplied by their rated score and then divided by 15. Thus, for each nurse, three total MW values, three weighted values, three rated values, and three scores for each of the 6 subscales were obtained in three working shifts. In the end, the mean of these values was calculated in three work shifts and used for analysis. The data analysis was performed with SPSS version 21.
Descriptive statistics (Mean and SD) were used to compare total MW, weights, rates, and scores of NASA-TLX subscales. To examine the correlation of MW with the resting period before and after each shift, the number of patients under care, work experience, and weekly working hours, the Pearson correlation coefficient was calculated. The t-test was used to compare MW based on gender, marital status, level of education, and being employed at the other centers. To compare MW load in terms of age, type of ICU, and type of work shift, one-way ANOVA was employed.
Results
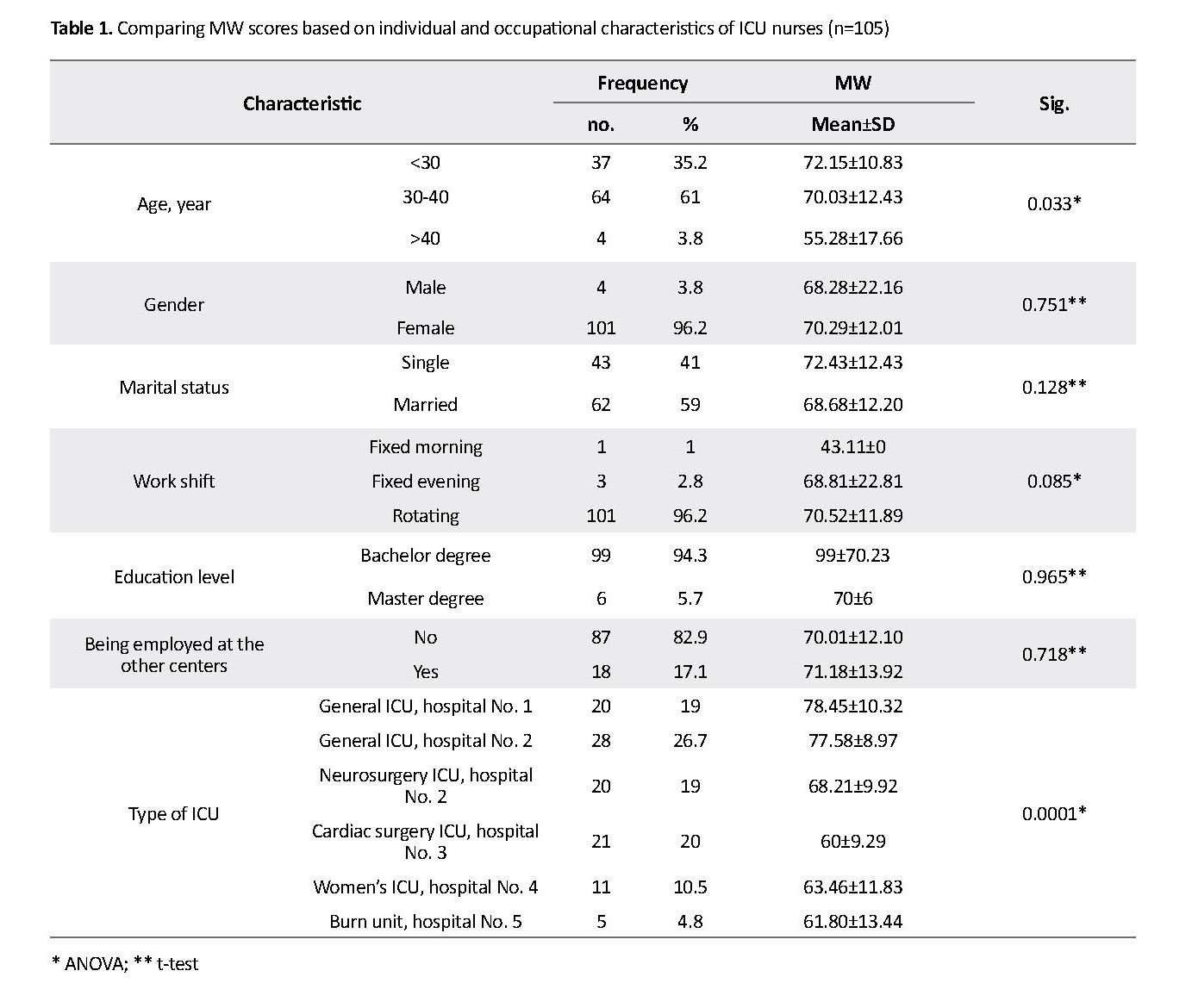
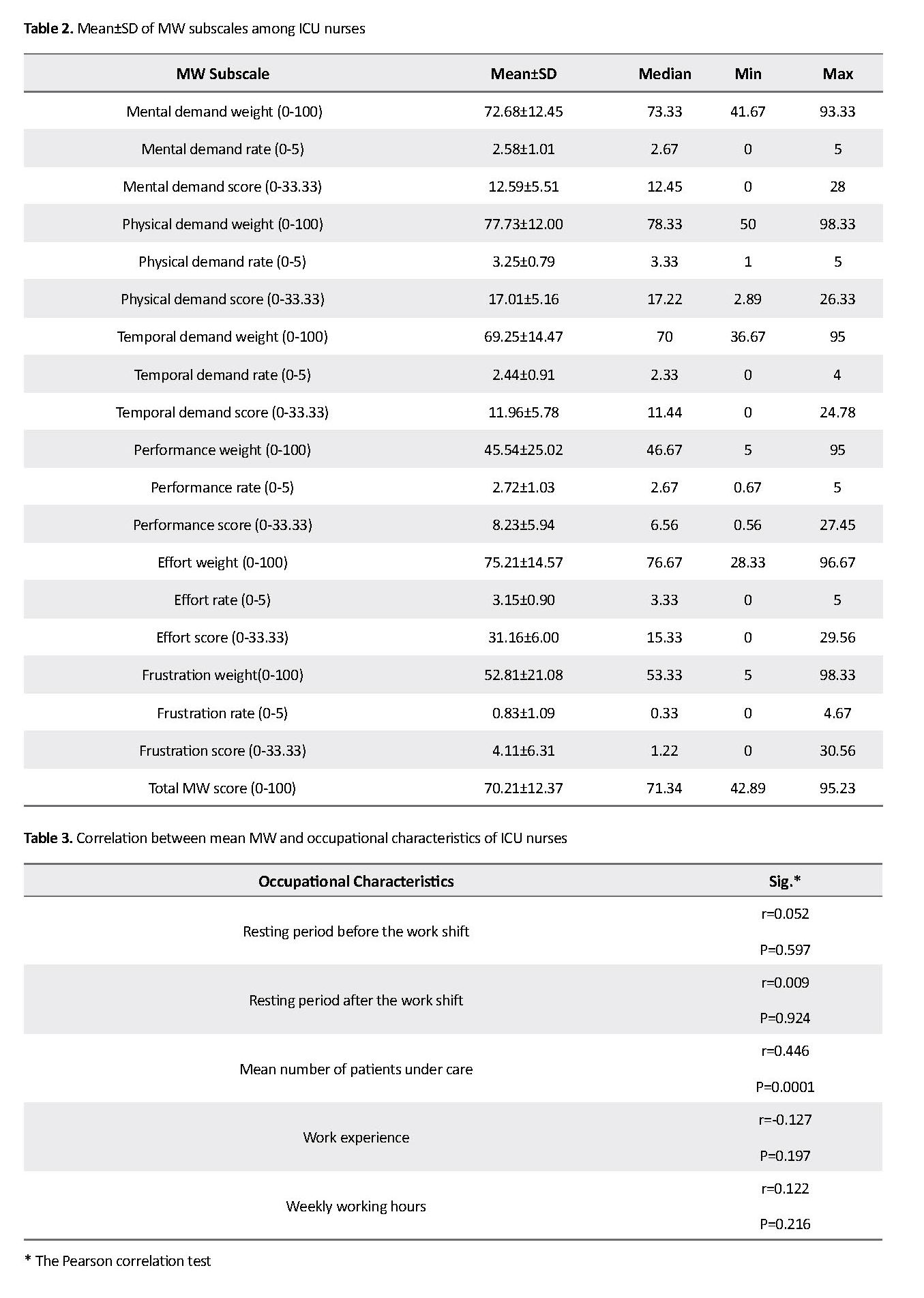
The obtained results reported that most of the participants were female (96.2%), married (59%), had a bachelor degree (94.3%), rotating work shifts (96.2%), and with an average age of 30-40 years (61%) (Table 1). The mean MW was 70.21±12.4, where physical demand dimension had the highest scores compared to other MW dimensions (Mean±SD weight: 77.73±12; Mean rate: 3.25; Mean score: 17.01) (Table 2).
In the past two decades, the intensity of nursing care and nursing workload increased due to the increased patients’ awareness and reduced hospitalization stay [1]. The increased workload is one of the most important concerns in healthcare and especially in Intensive Care Units (ICUs) that can have a negative impact on nurses and patients [2]. The workload is one of the influential factors on patient’s safety and the quality of nursing care [3]. Nowadays, because of the advancement of modern technology, work environments have changed, and as a result, many of them impose more cognitive needs compared to the physical needs of individuals. Therefore, depending on the type of profession, there is a concept called “mental workload” used in Ergonomics as a general concept. Nursing is one of the professions where this concept can be used. The workload is not limited to the physical tasks of nurses; their cognitive tasks (mental workload) are also a complex part of the overall workload of nurses [3, 4].
Although there is no universally accepted definition of Mental Workload (MW), and it is often considered by analogy to the physical workload [5, 6], it can be said that MW refers to all mental activities such as estimation, decision making, communication, identification and search, and is defined as the relationship between the mental resources required to perform a task and the ability of individuals to use these resources. MW is a subjective concept, which cannot be measured directly or be considered an absolute value. However given that the human mind can process the information at a limited rate, then MW is the percentage of the capacity used at any time point [7].
It is simply the amount of mental effort that one puts into a task [5, 8, 9], and requires actions such as concentration, reminder, decision making, and attention [8], and is essentially related to the individual’s mental abilities and how the information is received and processed, and at the end leads to decision making and action [5]. In other words, MW is a level of cognitive need or an analytical effort required by an individual to fulfill the physical, spatial, and environmental demands of a specific task [10].
Various studies show that in professions where MW is high, due to fatigue and inappropriate scheduling, the efficiency decreases, which reduces memory, damages the thinking process, causes irritability, and reduces learning [11, 12]. Tired people are more likely to choose risky behaviors such as doing shortcuts to perform tasks [12]. Nurses working in specific departments, such as ICUs, are subject to severe MW since they are always making important decisions that relate to the lives of patients. On the other hand, ICU nurses should be continuously responsive to the needs of their patients or the patients’ companions and are usually faced with the most severe emotional aspects of patients [12]. Accordingly, Hoonakker et al. [2] study results indicate high MW among ICU nurses.
Increased MW is reported as a major source of stress and burnout in nurses, which can have direct and indirect impacts on nurses and patients. Its direct impacts on patient care may be related to the insufficient time for caring duties, which increases the mortality rate of patients. Its indirect impacts on patient’s safety are via affecting communication, reducing job satisfaction and motivation, and causing burnout in nurses [10]. MW is associated with depression, anger, and interpersonal sensitivities [7]. Since MW has a direct relationship with the person’s performance and is one of the factors affecting the health, safety, and comfort of individuals, the concept of MW and its effects are one of the main topics of organizational behavior [10]. In this regard, the current study aimed at evaluating MW and its related factors in nurses working in the ICUs.
Materials and Methods
The current analytical study with the cross-sectional design was conducted in 2015 on 105 nurses working in ICUs of educational and medical centers in Rasht City, Iran. They were selected using the census method from nurses working in five ICUs in Rasht who have at least a BS degree and one year of experience. To collect data, a two-part questionnaire was used. The first part included individual and occupational characteristics of the study subjects (gender, age, marital status, work experience, education, type of ICU, number of patients under care, weekly working hours, working shift, resting period before and after the work shift, and working at the other centers). The second part was the National Aeronautics and Space Administration-Task Load Index (NASA-TLX) [2, 13].
It is one of the known tools to evaluate the MW from the individual point of view developed by Hart in 1998 at NASA’s Ames Research Center to measure subjective workload in aircraft simulation, and then extended by the Human Performance Group at NASA by conducting more than 40 experiments in three years. It is employed in more 550 research studies and recently used in many other professions, including healthcare [2, 14, 15].
Different studies verified the validity and reliability of this tool [2, 14]. Validity and reliability of its Persian version were verified in special units by Mohammadi et al. [12]. It has six subscales of mental demand, physical demand, temporal demand, performance, effort, and frustration. Each task is scored within a 100-point range based on a 5-point style. After reading descriptions for each scale, nurses give a score to each one from 0 to 100. This step is called “weighting”. In the next step, called “rating”, there are 15 two-choice items and individuals should choose the factor that plays the most important role in each item.
The weighted score is multiplied by the rated score and then divided by 15 to get an MW score for each subscale. By summing subscale scores, total MW score is obtained. This tool is compared and interpreted based on the mean difference between different groups (e.g. between hospitals, units, or staff). The group with the highest mean is reported to have a higher MW related to other groups.
The method of calculating the mental load of work can be performed either manually or with the help of NASA’s application [13]. In the current study, a portion of the information was calculated through the application and partly performed manually. Each questionnaire received a specific code. Since each nurse had to be examined in three work shifts, according to the monthly program of each unit, the next work shift of each nurse was found out and the necessary arrangements were made with the nurses to attend the study. Written informed consent was obtained from all participants.
To determine the MW score, first, the MW data of each nurse was transferred into the software and the weight and rate of the load for 6 subscales and the total MW score were calculated. Since the software does not give the MW score for each of the subscales, their scores were manually multiplied by their rated score and then divided by 15. Thus, for each nurse, three total MW values, three weighted values, three rated values, and three scores for each of the 6 subscales were obtained in three working shifts. In the end, the mean of these values was calculated in three work shifts and used for analysis. The data analysis was performed with SPSS version 21.
Descriptive statistics (Mean and SD) were used to compare total MW, weights, rates, and scores of NASA-TLX subscales. To examine the correlation of MW with the resting period before and after each shift, the number of patients under care, work experience, and weekly working hours, the Pearson correlation coefficient was calculated. The t-test was used to compare MW based on gender, marital status, level of education, and being employed at the other centers. To compare MW load in terms of age, type of ICU, and type of work shift, one-way ANOVA was employed.
Results
The obtained results reported that most of the participants were female (96.2%), married (59%), had a bachelor degree (94.3%), rotating work shifts (96.2%), and with an average age of 30-40 years (61%) (Table 1). The mean MW was 70.21±12.4, where physical demand dimension had the highest scores compared to other MW dimensions (Mean±SD weight: 77.73±12; Mean rate: 3.25; Mean score: 17.01) (Table 2).
A significant relationship was observed between MW and age of the nurses where the ones under 30 years had the highest MW and the ones aged above 40 years reported lower MW scores. A significant correlation was also observed between MW and type of ICU (Table 3), where nurses of cardiac surgery ICU reported the lowest MW score. The MW had a direct and significant relationship with the number of patients under care in each work shift, but no significant relationship was observed between MW of nurses and gender, marital status, level of education, type of work shift, being employed at the other centers, resting period before and after shift, work experience, and weekly working hours.
Discussion
In the current study, the Mean±SD MW of ICU nurses was reported 70.21±12.4. In the studies of Hoonakker et al. [2], Zakerian et al. [3], and Malekpour et al. [16], the mean MW was higher, while Giahi et al. [5] and Sarsangi et al. [10] reported lower values compared with those of the current study. All the mentioned studies used the same study tools like ours. Every occupation has a specific mean of MW, and the obtained results indicate the existence of MW in the nursing profession, especially in the ICUs, which can be due to the nature of this profession and the work environment of the nurses.
Another point to consider is that in the current study, the mental workload was studied and not the workload. Hence, the nurses that reported high mental workload may not necessarily have a high workload. Their high mental workload may be due to their perceptions or the psychological state and familial conflicts as well as their personality. Regarding the comparison of MW dimensions, it was revealed that the dimension of “physical demand” had the highest weight, rate, and scores compared with other dimensions. In the study by Malekpour et al. [16], the dimension of frustration had the highest weight, while in the study by Kazemi et al. [9], it was the mental demand dimension, and in the studies by Sarsangi et al. [10] and Zakerian et al. [3], dimension of effort had the highest weight. Regarding the rate of dimensions, Kazemi et al. showed that frustration had the highest rate values and other studies reported no results about the rates and scores of MW dimensions.
This difference between the results of the current study and those of similar studies may be related to different environmental conditions, sampling, and implementation. For example, in the current study, the MW of nurses was investigated in three separate work shifts using its average value for comparison, while in the mentioned studies it was examined in one work shift. Obviously, examining an MW variable in three work shifts increases the likelihood of obtaining more accurate results. It is possible that factors outside the workplace influence MW and its subscales.
Results of the current study also showed that MW had a significant association with the age factor in ICU nurses where nurses aged less than 30 years had the highest MW level and the ones more than 40 years had the lowest MW scores. It was consistent with the findings of Kazemi et al. [9] and Sarsangi et al. [10] reporting a significant correlation between MW and age. In the study by Kazemi et al. the age group of 22-30 years had the lowest MW level and the age group of >50 years showed the highest MW scores. However, in the study by Hoonakker et al. [2] no significant difference was reported between MW and age factor except in physical demand dimension.
Malekpour et al. [16] reported no significant correlation between them, either. Since studies show a significant relationship between MW and occupational stress [17, 18], probably with increasing age, due to increased control over the environment and working conditions, many occupational stresses are eliminated, and as a result, the MW level decreases. On the other hand, due to the nature of the nursing profession and the work environment of the nurses, long-term nursing is a tedious and stressful job and increases the MW of older nurses, which justifies the results of studies inconsistent with the current study results.
Based on the results of the current study, MW of ICU nurses had a significant relationship with the type of ICU, where the nurses of general ICU of hospital No.3 and cardiac surgery ICU had the highest and lowest MW levels, respectively. In the study by Hoonakker et al. [2] among adult ICU, internal/surgical ICU, burn unit, neurosurgical ICU, neonatal ICU, pediatric ICU, cardiac ICU, and surgical ICU, nurses of adult and cardiac ICUs had higher MW than the ones in neurosurgical and neonatal ICUs. The difference in MW of nurses in various types of ICUs can be due to the type of hospitalized patients, as well as internal rules regarding the allocation of manpower and the number of patients in such sectors.
In the current study, the nurse-to-patient ratio in surgical ICU was 1:1 and the shift manager was not responsible for the care of any patient, while in general ICU the ratio was 1:2 and 1:3 and the shift manager, in addition to direct patient care, was responsible for managerial tasks. Clearly, with the increase in the number of patients under the care and managerial tasks, the responsibility of nurses becomes heavier, which can increase their MW in this section.
The current study found no significant association between MW and the type of work shift. Malekpour et al. [16] reported a higher MW level in the evening and night shifts compared to morning and rotating shifts. In the study by Hoonakker et al. a significant difference was observed between MW and type of work shift where nurses of 12-h shifts (day and night) had a higher overall workload, physical demands, and frustration compared with those of an 8-h shift (morning or evening). Overall workload, temporal demands, and efforts were higher in 12-h day-shifts than in 12-h night shifts. Sarsangi et al. [10] also reported a significant correlation between MW and work shift. This inconsistency in results may be due to the difference in the sampling method.
A significant association was reported in the current study between MW of ICU nurses and the number of patients under their care in each work shift, in such a way that with the increase in their number, MW of nurses increased. It was in agreement with the results of Kazemi et al. [9] and Malekpour et al. [16]. Regarding this finding, it can be explained that as the number of patients under care increases, the responsibilities and hence MW of nurses increases.
According to the results of the current study, MW of nurses in the ICU of hospital No. 1 was high. According to the significant relationship between MW and the type of ICU, the age of nurses, and the number of patients under care in each shift, and the effect of intra-sectoral and intra-hospital rules on MW, it is necessary to employ interventional strategies to reduce the MW level in this group. In units with higher MW, the number of patients under the care of each nurse should be reduced by appropriate distribution of human resources. Since the MW has a significant relationship with occupational stress [17, 18], with proper training, especially in younger staff (who has fewer skills to overcome stressful factors in the workplace), many tensions and consequently mental workload can be reduced in nurses, and the effects of excessive mental workload on nurses and patients can be prevented.
Uncontrolled mental status and familial conflicts of nurses during filling in the questionnaires and their personality type were among the limitations of the current study. It should also be considered that the current study evaluated the mental workload of the ICU nurses and not their workload. Therefore, the subjects that reported a high mental workload may not necessarily have a high workload, and their high mental workload may be due to their perceptions.
Ethical Considerations
Compliance with ethical guidelines
The current study was approved by the Social Determinants of Health Research Center of Guilan University of Medical Sciences (Registration No. 94070714) and also the Ethics Committee of the University (Ethical code: IR.GUMS.REC.1394.286).
Funding
This study was financially supported by Guilan University of Medical Sciences.
Authors contributions
Conceptualization and supervision: Shadman Reza Masule, Mino Mitra Chehrzad; Conceptualization and data analysis: Ehsan Kazemi Nejhad Leili; and Contributing to all stages of research implementation: Kolsom Nasirizad Moghadam.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgements
Authors would like to thank the Deputy of Research and Technology of the Guilan University of Medical Sciences.
References
Quinn LW. Throughput and nurses’ workloads: influences on nurse and patient outcomes [PhD. dissertation]. Philadelphia, Pennsylvania: University of Pennsylvania; 2013.
Hoonakker P, Carayan P, Gurses A, Brown R, McGuire K, Khunlertkit A, et al. Measuring workload of ICU nurses with a questionnaire survey: The NASA task Load Index. IISE Transactions on Healthcare Systems Engineering. 2011; 1(2):131-43. [DOI:10.1080/19488300.2011.609524] [PMID] [PMCID]
Zakerian A, Abasi Nia M, Mohammadin F, Fathi A, Rahmani A, Ahmadnezhad I, et al. [The relationship between workload and quality of life among hospital staffs (Persian)]. Journal of Ergonomics. 2013; 1(1):43-56.
Myny D, Van Heck A, De Bacquer D, Verhaeeghe S, Gobert M, Defloor T, et al. Determining a set of measurable and relevant factors affecting nursing workload in the acute care hospital setting: A cross sectional study. International Journal of Nursing Studies. 2012; 2012(49):427-36. [DOI:10.1016/j.ijnurstu.2011.10.005] [PMID]
Giahi O, Darvishi E, Akbarzadeh M, Shahsavari S. [Assessment of the relationship of the risk of subjective work load to musculoskeletal disorders in bank staff in Kurdistan Province (Persian)]. Scientific Journal of Kurdistan University of Medical Sciences. 2014; 19(4):36-45.
Galy E, Paxion J, Berthelon C. Measuring mental workload with the NASA-TLX needs to examine each dimension rather than relying on the global score: An example with driving. Ergonomics. 2018; 61(4):517-27. [DOI:10.1080/00140139.2017.1369583] [PMID]
Ozkan A, Ozdevecioglu M, Kaga Y, Ozsahin Koc F. Effect of mental workloads on depression-anger symptoms and interpersonal sensitivities of accounting professionals. Revista de Contabilidad- Spanish Accounting Review. 2015; 18(2):194-99. [DOI:10.1016/j.rcsar.2014.06.005]
Safari S, Akbari J, Kazemi M, AminMououdi M, Mahaki B. Personnel’s health surveillance at work: Effect of age, Body Mass Index, and shift work on mental workload and work ability index. Hindawi Publishing Corporation Journal of Environmental and Public Health. 2013; 2013:289498. [DOI:10.1155/2013/289498] [PMID] [PMCID]
Safari Sh, Mohammadi Bolban Abadi H, Kazemi M. [Evaluation mental work load in nursing critical care unit with National Aeronautics and Space Administration Task Load Index (NASATLX) (Persian)]. Health System Research Journal. 2013; 9(6):613-9.
Sarsangi V, Saberi H, Hannani M, Honarjoo F, Salim Abadi M, Goroohi M, et al. [Mental workload and its affected factors among nurses in Kashan Province during 2014 (Persian)]. Journal of Rafsanjan University of Medical Sciences. 2015; 14(1):25-36.
Young G, Zavelina L, Hooper V. Assessment of workload using NASA task load index in Perianesthesia nursing. Journal of PeriAnesthesia Nursing. 2008; 23(2):102-10. [DOI:10.1016/j.jopan.2008.01.008] [PMID]
Mohammadi M, Mazlomi A, Nasl Seraji J, Zeraati h. [Designing questionnaire of assessing mental workload and determine its validity and reliability among ICUs nurses in one of the TUMS’s hospitals (Persian)]. Scientific Journal of School of Public Health and Institute of Public Health Research. 2012; 11(2):87-96.
Kamfiruzi A. National aeronautics and space administration task load index [Internet]. 2019 [Updated 2019 March 6]. Available from: http://humansystems.arc.nasa.gov/groups/tlx/computer.php .http://earmin.com/nasa-tlx-fa/
Khandan M, Roshan Zamir S, Maghsoudipour M. [Survey of workload and job satisfaction relationship in a heavy mental manufacturing company (Persian)]. Iran Occupational Health. 2012; 9(1):30-6.
Tubbs-Cooley HL, Mara CA, Carle AC, Gurses AP. The NASA Task Load Index as a measure of overall workload among neonatal, paediatric and adult intensive care nurses. Intensive and Critical Care Nursing. 2018; 46:64-9. [DOI:10.1016/j.iccn.2018.01.004] [PMID]
Malekpour F, Mohammadian Y, Malekpour A, Mohammadpour Y, Sheikh Ahmadi A, Shakarami A. [Assessment of mental workload in nursing by using NASA-TLX (Persian)]. Journal of Urmia Nursing and Midwifery Faculty. 2014; 11(11):892-9.
Gholam Nejad H, Nikpeyma N. [Occupational stressors in nursing (Persian)]. Iran Occupational Health. 2009; 6(1):22-7.
Bahrami A, Akbari H, Mousavi G, Hannani M, Ramezani Y. [Job stress among the nursing staff of Kashan hospital (Persian)]. Feyz. 2011; 15(4):366-73.
Article Type : Research |
Subject:
Special
Received: 2018/12/20 | Accepted: 2019/02/5 | Published: 2019/04/1
Received: 2018/12/20 | Accepted: 2019/02/5 | Published: 2019/04/1
Send email to the article author
| Rights and permissions | |
 | This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Articles Copyright © The Author(s).
Owned by Guilan University of Medical Sciences.
Co-published by Negah Institute for Scientific Communication.
Contact Information
JHNM Office, Guilan University of Medical Sciences P.O.Box 41635-1873, Rasht, Iran
Journal Tel: +9813 33553202
Publisher Tel: +9821 453 55 555; +9821 453 55 000
Email: holisticnmj@gmail.com, nursjournal@gums.ac.ir
