Mon, May 6, 2024
Volume 29, Issue 1 (1-2019)
JHNM 2019, 29(1): 15-21 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Atadokht A, Ebrahimzadeh S, Mikaeeli N. The Effectiveness of Humor Skills Training on Positive and Negative Symptoms of Chronic Schizophrenia Spectrum. JHNM 2019; 29 (1) :15-21
URL: http://hnmj.gums.ac.ir/article-1-658-en.html
URL: http://hnmj.gums.ac.ir/article-1-658-en.html



1- Associate Professor, Department of Psychology, School of Education and Psychology, University of Mohaghegh Ardabili, Ardabil, Iran. , ak_atadokht@yahoo.com
2- Psychology (MA.), School of Education and Psychology, University of Mohaghegh Ardabili, Ardabil, Iran.
3- Associate Professor, Department of Psychology, School of Education and Psychology, University of Mohaghegh Ardabili, Ardabil, Iran.
2- Psychology (MA.), School of Education and Psychology, University of Mohaghegh Ardabili, Ardabil, Iran.
3- Associate Professor, Department of Psychology, School of Education and Psychology, University of Mohaghegh Ardabili, Ardabil, Iran.
Full-Text [PDF 500 kb]
(1683 Downloads)
| Abstract (HTML) (4128 Views)

Full-Text: (1490 Views)
Introduction
Schizophrenia is a serious mental disorder in which the patient experiences distorted perception of reality and disturbances in thinking, behavior, emotions and motivation [1]. The prevalence of schizophrenia is about 0.3% to 0.7% [2]. The incidence rate is quite similar in men and women, but the disorder onset in men is earlier and they are more likely to be admitted to rehabilitation centers. About 5% to 25% of these patients are treated annually [3]. Symptoms of schizophrenia are expressed in patients’ physical, mental, behavioral and emotional aspects and affect patients’ thoughts, feelings, senses, and behavior. These include both positive and negative symptoms.
Positive symptoms are those that were not present in the patient, but appeared after the disorder [4]. Contrary to what the name implies, these symptoms are not good or useful. They are called “positive” because they expand the truth and enhance it. Such expansion or exaggeration is undesirable [5]. The symptoms are more functional and the most important of which are hallucinations, delusions, strange behavior, and impaired thinking [6]. Negative symptoms indicate some kinds of activities and tasks that should be existed [5] but expressing behavioral disorders. They include superficial emotion, speech poverty (alogia), passivity, lack of motivation, lack of pleasure, attention and cognitive deficits [6].
Schizophrenia causes conflicts in job performance and education along with economic, social and personal problems and would instigate numerous medical and non-medical costs such as loss of work (due to illness or caring for relatives) on the patient, the family and society [7]. Long-term treatment goals consist of improving negative symptoms and empowering patients’ functioning and optimizing positive symptoms control [8-10].
Various therapeutic interventions have been recommended for the patients among which are cognitive behavioral therapy to reduce positive symptoms [11]; music therapy to control psychotic symptoms [12], depression (as positive symptoms) [13], and increased quality of life [14]; agricultural activity to improve physical, social, emotional and cognitive functioning [15], and quality of life [16]; and humorous films to reduce negative symptoms of anxiety and depression in patients with schizophrenia [17]. Although the conventional treatment of schizophrenia include both medical and psychiatric practices, integrating psychological treatment with medical therapy may significantly improve the general health of the patients with schizophrenia [18].
In this regard, one of the psychological interventions to control symptoms and complications of mental disorders is strengthening the sense of humor i.e. the ability to understand and experience a humorous and ridiculous situation. This ability is not inherited but acquired through learning and practice. Through emotional, cognitive, social and physiological impact, humor can be used as a new procedure to deal with various mental disorders and rehabilitate them [17]. Its first function would be serving as a distracting technique, i.e. preventing patients from thinking about their problems [19] and help people have more desire to do social activities as well as forming social interaction and strengthening it over time [20].
The results of most studies on the impact of physical and psychological health foster a sense of humor [21], because telling jokes and humor serve as an effective way to deal with problems, or cope with the problems which are uncontrollable [22]. In humorous patients, the process of perception and judgment of the current condition is better [23]. The implementation of humor skill training in a mental health service may improve rehabilitative outcomes [24] and reduce frustration in depressed patients with spinal cord injury [25, 26].
Schizophrenia is a chronic disease, so huge expenditures including the cost of medication, frequent hospitalization and outpatient centers, therapeutic and rehabilitation services are obviously imposed on the health system and the patients’ families. Therefore, exploring new ways to improve the patients’ symptoms seems to be necessary. With appropriate skills and techniques to reduce this problem, steps can be taken to improve patients’ mental and physical problems. In this regard, this study aimed to determine the effectiveness of humor skills training in reducing positive and negative symptoms of male patients with chronic schizophrenia.
Materials and Methods
The research adopted a quasi-experimental approach with pretest-posttest design and control group. In this study, the skills of humor were the independent variables and positive and negative symptoms were the dependent variables. The study population consisted of male patients with chronic schizophrenia hospitalized in medical and rehabilitation centers in Ardabil, Iran (five centers with approximately 250 patients) in 2016. Among these centers, one rehabilitation center was randomly selected and then 30 subjects were selected from this center through simple random sampling and were randomly categorized into two groups, experimental (n=15) and control (n=15), according to the minimum sample law in experimental studies.
The study inclusion criteria comprised confirmed diagnosis of schizophrenia by psychiatrists through clinical interview based on DSM-5 diagnostic criteria, ability to read and write, and patient and family’s written consent to participate in the study. In the process of implementing the study, one of the patients died and four others were excluded from the research process because of taking time off from the study and finally the data of 13 patients in the experimental group and 12 patients in the control group were analyzed.
To collect the data, Positive and Negative Syndrome Scale (PANSS) was used that developed in 1987 by Kay to measure the severity of symptoms in patients with schizophrenia [27]. It assesses five subscales of negative symptoms, positive symptoms, disintegration, agitation, anxiety, and depression. The scale is scored based on a 5-point Likert-type scale. High scores indicate more severe symptoms. Total scores were obtained from summing up scores of 30 questions. The Cronbach alpha coefficient for this scale was estimated as 0.83. In a study conducted by Abolghasemi [28] and in this study, the Cronbach alpha coefficient was estimated as 0.80.
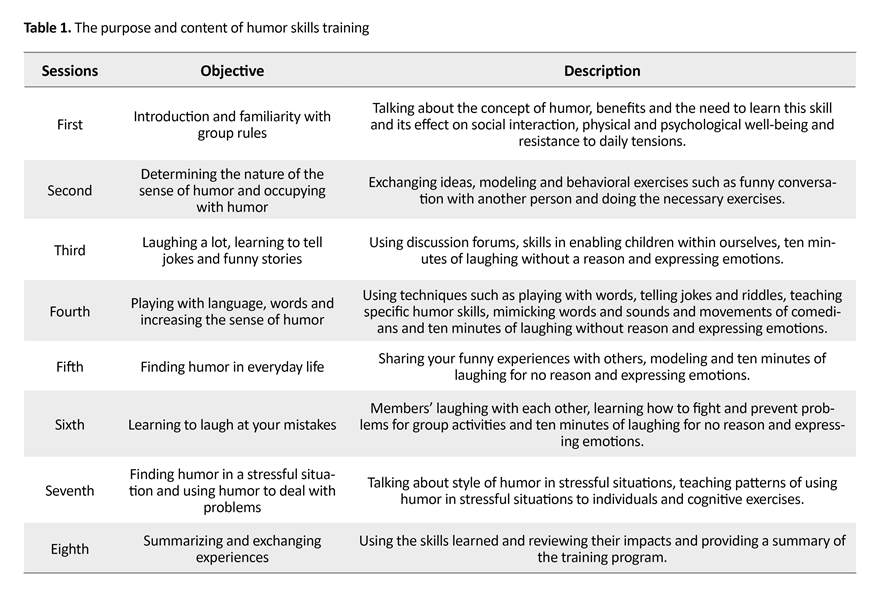
The study procedure was as follows: after randomly assigning the participants (the names are arranged alphabetically and divided into even and odd numbers), they were divided into control and experimental groups. First, members of both groups were tested (as pretest). Then, humor skills training program [25] was administered to the experimental group using the 8-step McGee’s humor skills training program for 4 weeks, two 60-minute sessions per week. The session contents are listed in Table 1. It should be noted that both the assessment and the intervention were carried out by one person (researcher) and patients in both groups received their routine treatment during the intervention.
To analyze the data, the Chi-square test was used to compare the frequency distribution of patients in the two groups in terms of demographic characteristics and their homogeneity. In addition, covariance analysis was used to evaluate the effectiveness of intervention and compare the controlling effect of pretest and posttest scores. All analyses were done in SPSS V. 18.
Results
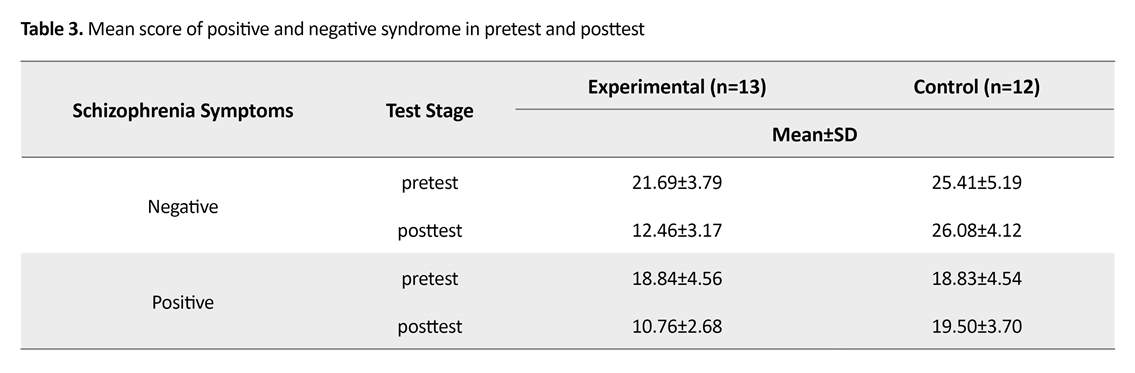
All patients were male and some personal characteristics of the participants are reported and compared in Table 2. According to the findings, there is no significant difference between groups in terms of educational status, marital status, age distribution and admission in the center (P>0.05). Table 3 presents the mean score of schizophrenia symptoms in the experimental and control group. The experimental group scores in the posttest decreased. To evaluate the effectiveness of teaching humor skills on the positive and negative symptoms, the covariance analysis was used.
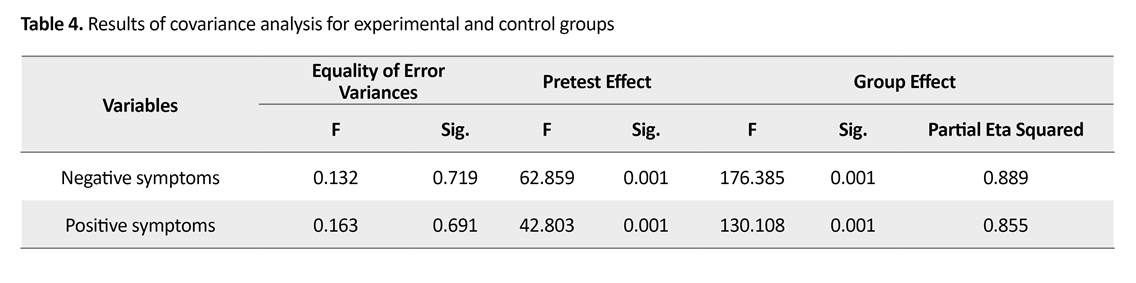
The results in Table 4 indicate that after controlling the pretest effect, there is a significant difference in positive and negative symptoms in posttest scores between the two groups (P<0.05); and the ETA coefficient or the effect size estimate suggests that subjects’ membership to a group (with or without treatment) explained 85% to 89% of the variance in positive and negative symptoms. The results of the homogeneity of variances analysis indicate that the assumption has been observed in all the studied variables.
Schizophrenia is a serious mental disorder in which the patient experiences distorted perception of reality and disturbances in thinking, behavior, emotions and motivation [1]. The prevalence of schizophrenia is about 0.3% to 0.7% [2]. The incidence rate is quite similar in men and women, but the disorder onset in men is earlier and they are more likely to be admitted to rehabilitation centers. About 5% to 25% of these patients are treated annually [3]. Symptoms of schizophrenia are expressed in patients’ physical, mental, behavioral and emotional aspects and affect patients’ thoughts, feelings, senses, and behavior. These include both positive and negative symptoms.
Positive symptoms are those that were not present in the patient, but appeared after the disorder [4]. Contrary to what the name implies, these symptoms are not good or useful. They are called “positive” because they expand the truth and enhance it. Such expansion or exaggeration is undesirable [5]. The symptoms are more functional and the most important of which are hallucinations, delusions, strange behavior, and impaired thinking [6]. Negative symptoms indicate some kinds of activities and tasks that should be existed [5] but expressing behavioral disorders. They include superficial emotion, speech poverty (alogia), passivity, lack of motivation, lack of pleasure, attention and cognitive deficits [6].
Schizophrenia causes conflicts in job performance and education along with economic, social and personal problems and would instigate numerous medical and non-medical costs such as loss of work (due to illness or caring for relatives) on the patient, the family and society [7]. Long-term treatment goals consist of improving negative symptoms and empowering patients’ functioning and optimizing positive symptoms control [8-10].
Various therapeutic interventions have been recommended for the patients among which are cognitive behavioral therapy to reduce positive symptoms [11]; music therapy to control psychotic symptoms [12], depression (as positive symptoms) [13], and increased quality of life [14]; agricultural activity to improve physical, social, emotional and cognitive functioning [15], and quality of life [16]; and humorous films to reduce negative symptoms of anxiety and depression in patients with schizophrenia [17]. Although the conventional treatment of schizophrenia include both medical and psychiatric practices, integrating psychological treatment with medical therapy may significantly improve the general health of the patients with schizophrenia [18].
In this regard, one of the psychological interventions to control symptoms and complications of mental disorders is strengthening the sense of humor i.e. the ability to understand and experience a humorous and ridiculous situation. This ability is not inherited but acquired through learning and practice. Through emotional, cognitive, social and physiological impact, humor can be used as a new procedure to deal with various mental disorders and rehabilitate them [17]. Its first function would be serving as a distracting technique, i.e. preventing patients from thinking about their problems [19] and help people have more desire to do social activities as well as forming social interaction and strengthening it over time [20].
The results of most studies on the impact of physical and psychological health foster a sense of humor [21], because telling jokes and humor serve as an effective way to deal with problems, or cope with the problems which are uncontrollable [22]. In humorous patients, the process of perception and judgment of the current condition is better [23]. The implementation of humor skill training in a mental health service may improve rehabilitative outcomes [24] and reduce frustration in depressed patients with spinal cord injury [25, 26].
Schizophrenia is a chronic disease, so huge expenditures including the cost of medication, frequent hospitalization and outpatient centers, therapeutic and rehabilitation services are obviously imposed on the health system and the patients’ families. Therefore, exploring new ways to improve the patients’ symptoms seems to be necessary. With appropriate skills and techniques to reduce this problem, steps can be taken to improve patients’ mental and physical problems. In this regard, this study aimed to determine the effectiveness of humor skills training in reducing positive and negative symptoms of male patients with chronic schizophrenia.
Materials and Methods
The research adopted a quasi-experimental approach with pretest-posttest design and control group. In this study, the skills of humor were the independent variables and positive and negative symptoms were the dependent variables. The study population consisted of male patients with chronic schizophrenia hospitalized in medical and rehabilitation centers in Ardabil, Iran (five centers with approximately 250 patients) in 2016. Among these centers, one rehabilitation center was randomly selected and then 30 subjects were selected from this center through simple random sampling and were randomly categorized into two groups, experimental (n=15) and control (n=15), according to the minimum sample law in experimental studies.
The study inclusion criteria comprised confirmed diagnosis of schizophrenia by psychiatrists through clinical interview based on DSM-5 diagnostic criteria, ability to read and write, and patient and family’s written consent to participate in the study. In the process of implementing the study, one of the patients died and four others were excluded from the research process because of taking time off from the study and finally the data of 13 patients in the experimental group and 12 patients in the control group were analyzed.
To collect the data, Positive and Negative Syndrome Scale (PANSS) was used that developed in 1987 by Kay to measure the severity of symptoms in patients with schizophrenia [27]. It assesses five subscales of negative symptoms, positive symptoms, disintegration, agitation, anxiety, and depression. The scale is scored based on a 5-point Likert-type scale. High scores indicate more severe symptoms. Total scores were obtained from summing up scores of 30 questions. The Cronbach alpha coefficient for this scale was estimated as 0.83. In a study conducted by Abolghasemi [28] and in this study, the Cronbach alpha coefficient was estimated as 0.80.
The study procedure was as follows: after randomly assigning the participants (the names are arranged alphabetically and divided into even and odd numbers), they were divided into control and experimental groups. First, members of both groups were tested (as pretest). Then, humor skills training program [25] was administered to the experimental group using the 8-step McGee’s humor skills training program for 4 weeks, two 60-minute sessions per week. The session contents are listed in Table 1. It should be noted that both the assessment and the intervention were carried out by one person (researcher) and patients in both groups received their routine treatment during the intervention.
To analyze the data, the Chi-square test was used to compare the frequency distribution of patients in the two groups in terms of demographic characteristics and their homogeneity. In addition, covariance analysis was used to evaluate the effectiveness of intervention and compare the controlling effect of pretest and posttest scores. All analyses were done in SPSS V. 18.
Results
All patients were male and some personal characteristics of the participants are reported and compared in Table 2. According to the findings, there is no significant difference between groups in terms of educational status, marital status, age distribution and admission in the center (P>0.05). Table 3 presents the mean score of schizophrenia symptoms in the experimental and control group. The experimental group scores in the posttest decreased. To evaluate the effectiveness of teaching humor skills on the positive and negative symptoms, the covariance analysis was used.
The results in Table 4 indicate that after controlling the pretest effect, there is a significant difference in positive and negative symptoms in posttest scores between the two groups (P<0.05); and the ETA coefficient or the effect size estimate suggests that subjects’ membership to a group (with or without treatment) explained 85% to 89% of the variance in positive and negative symptoms. The results of the homogeneity of variances analysis indicate that the assumption has been observed in all the studied variables.
Discussion
The study results indicate that the experimental group had a significant reduction in negative symptoms, expressed in their posttest scores. Thus, teaching humor skills significantly reduced the negative symptoms of schizophrenia disorder. The findings of this study are in line with the results of the studies by Chunfeng et al. [24] and Gelkopf [17] on the effect of humor on patients with schizophrenia and with the Shams study on depressed people’s frustration and compatibility [26]. The results of the current study are also consistent with the study by Falkenberg on improving the depressed patients’ mood [29].
These results can be justified because in schizophrenic patients with negative symptoms due to behavioral impairments such as passivity, inexpressiveness, lack of enjoyment, loss of emotional and social apathy, almost no stimulus can trigger emotional responses [30]. Thus, jokes and humor in these patients would trigger a sense of enjoyment, and serve as an acceptable therapeutic method to endure many unpleasant things. They gradually gain the capacity to cope with stress and anxiety caused by serious diseases and eventually stop and even improve their condition [31].
When hilarious and witty people encounter negative events, they try to maintain their positive feeling, while people with weak sense of humor have lower levels of positive emotions. In addition to the beneficial nature of positive emotions and coping with negative mood, humor serves as a coping mechanism against stressful events of life and a valuable social skill useful to establish, maintain and improve interpersonal relationships [32]. People who learn, practice and apply the humor skills, can partly forget their illnesses. Such people are also able to establish sound relationships with family members and others and achieve a high level of social harmony [25]. The results also showed that humor skills training reduces positive symptoms in patients with schizophrenia. Such finding is consistent with the results of the studies by Falkenberg [29] and Shams [26] but disagree with the results of Chunfeng [24] and Gelkopf et al. Studies [17].
To explain such discrepancy between the results, it should be mentioned that the patients with schizophrenia use schemes related to hallucinations and delusions to organize their information. This leads to their inability to correctly process and recognize emotions resulting in facing trouble in their social interaction and exposure to different life situations [33]. These patients express their excitement in almost unusual ways and such strange behavior makes people stay away from these patients [34].
The significant relationship can be attributed to humor skills training sessions which help them experience the right way to show their emotions and appropriate facial expressions. In addition, positive emotions lead to social cohesion and expression of negative emotions and they serve as one of the most common and most effective methods of inducing mood. Jokes and humor release tension from the conflicts, attitudes and ideas and can be useful to help the mentally-ill patients to the extent that they have lower stress, better social interactions. They also cope better with the problems and are more compatible people [35].
Humor widely and positively impact the patients’ health, perceptions, attitudes, judgments and feelings [23]. Humor helps people see the positive side of the events and consider them as funny conditions which would, therefore, decrease the stress [36]. As a result, humor would bring about the enjoyment and better social relations. It teaches patients the proper way to experience the excitement. The negative symptoms would decrease patients’ ability to enjoy positive stimuli and social interactions and positive symptoms cause problems for the patients to express their emotions, but humor prepares the ground for better social relationships.
Based on our results, the changes in the experimental group, who received the humor skills training, reflect the impact of learning these skills in eight sessions. Therefore, the skills taught in this study can be used as part of treatment of schizophrenic patients. In future studies, it is suggested to assess the patients’ condition at 3-month or 6-month follow-up or more to test the effects of long-term intervention. In addition, to increase the generalizability of the findings, further studies should include female schizophrenic patients to compare the differences in the study variables and to examine the effect of humor skills training on other issues in these patients.
Ethical Considerations
Compliance with ethical guidelines
This research has been approved by the Ethics Committee of the Islamic Azad University of Ardabil (code No. IR.IAU.ARDABIL.REC.1395.6) and registered (IRCT2016053028174N1).
Funding
This article was extracted from a Master thesis of Sorayya Ebrahimzadeh in School of Education and Psychology, University of Mohaghegh Ardabili, Ardabil, Iran.
Authors contributions
The authors contributions is as follows: Conceptualization, methodology, investigation and writing-original draft: Akbar Atadokht and Sorayya Ebrahimzadeh; Writing-review & editing: Akbar Atadokht and Niloofar Mikaeeli; Funding acquisition and resources: Sorayya Ebrahimzadeh; and Supervision: Akbar Atadokht and Niloofar Mikaeeli.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgements
Researchers would like to appreciate the personnel of Ardabil Rehabilitation Centers.
References
The study results indicate that the experimental group had a significant reduction in negative symptoms, expressed in their posttest scores. Thus, teaching humor skills significantly reduced the negative symptoms of schizophrenia disorder. The findings of this study are in line with the results of the studies by Chunfeng et al. [24] and Gelkopf [17] on the effect of humor on patients with schizophrenia and with the Shams study on depressed people’s frustration and compatibility [26]. The results of the current study are also consistent with the study by Falkenberg on improving the depressed patients’ mood [29].
These results can be justified because in schizophrenic patients with negative symptoms due to behavioral impairments such as passivity, inexpressiveness, lack of enjoyment, loss of emotional and social apathy, almost no stimulus can trigger emotional responses [30]. Thus, jokes and humor in these patients would trigger a sense of enjoyment, and serve as an acceptable therapeutic method to endure many unpleasant things. They gradually gain the capacity to cope with stress and anxiety caused by serious diseases and eventually stop and even improve their condition [31].
When hilarious and witty people encounter negative events, they try to maintain their positive feeling, while people with weak sense of humor have lower levels of positive emotions. In addition to the beneficial nature of positive emotions and coping with negative mood, humor serves as a coping mechanism against stressful events of life and a valuable social skill useful to establish, maintain and improve interpersonal relationships [32]. People who learn, practice and apply the humor skills, can partly forget their illnesses. Such people are also able to establish sound relationships with family members and others and achieve a high level of social harmony [25]. The results also showed that humor skills training reduces positive symptoms in patients with schizophrenia. Such finding is consistent with the results of the studies by Falkenberg [29] and Shams [26] but disagree with the results of Chunfeng [24] and Gelkopf et al. Studies [17].
To explain such discrepancy between the results, it should be mentioned that the patients with schizophrenia use schemes related to hallucinations and delusions to organize their information. This leads to their inability to correctly process and recognize emotions resulting in facing trouble in their social interaction and exposure to different life situations [33]. These patients express their excitement in almost unusual ways and such strange behavior makes people stay away from these patients [34].
The significant relationship can be attributed to humor skills training sessions which help them experience the right way to show their emotions and appropriate facial expressions. In addition, positive emotions lead to social cohesion and expression of negative emotions and they serve as one of the most common and most effective methods of inducing mood. Jokes and humor release tension from the conflicts, attitudes and ideas and can be useful to help the mentally-ill patients to the extent that they have lower stress, better social interactions. They also cope better with the problems and are more compatible people [35].
Humor widely and positively impact the patients’ health, perceptions, attitudes, judgments and feelings [23]. Humor helps people see the positive side of the events and consider them as funny conditions which would, therefore, decrease the stress [36]. As a result, humor would bring about the enjoyment and better social relations. It teaches patients the proper way to experience the excitement. The negative symptoms would decrease patients’ ability to enjoy positive stimuli and social interactions and positive symptoms cause problems for the patients to express their emotions, but humor prepares the ground for better social relationships.
Based on our results, the changes in the experimental group, who received the humor skills training, reflect the impact of learning these skills in eight sessions. Therefore, the skills taught in this study can be used as part of treatment of schizophrenic patients. In future studies, it is suggested to assess the patients’ condition at 3-month or 6-month follow-up or more to test the effects of long-term intervention. In addition, to increase the generalizability of the findings, further studies should include female schizophrenic patients to compare the differences in the study variables and to examine the effect of humor skills training on other issues in these patients.
Ethical Considerations
Compliance with ethical guidelines
This research has been approved by the Ethics Committee of the Islamic Azad University of Ardabil (code No. IR.IAU.ARDABIL.REC.1395.6) and registered (IRCT2016053028174N1).
Funding
This article was extracted from a Master thesis of Sorayya Ebrahimzadeh in School of Education and Psychology, University of Mohaghegh Ardabili, Ardabil, Iran.
Authors contributions
The authors contributions is as follows: Conceptualization, methodology, investigation and writing-original draft: Akbar Atadokht and Sorayya Ebrahimzadeh; Writing-review & editing: Akbar Atadokht and Niloofar Mikaeeli; Funding acquisition and resources: Sorayya Ebrahimzadeh; and Supervision: Akbar Atadokht and Niloofar Mikaeeli.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgements
Researchers would like to appreciate the personnel of Ardabil Rehabilitation Centers.
References
- Halgin R. Abnormal Psychology: Clinical Perspectives on Psychological Disorders [Y Seyed Mohammadi, Persian Trans.]. Tehran: Ravan Publisher; 2014.
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. [Y Seyed Mohammadi, Persian Trans.]. Tehran: Ravan Publisher; 2013.
- Jianhuai CH, Zhijian YA, Jiaolong QI, Rui YA, Lingling HU, Qing LU. Abnormal inter-and intra-hemispheric integration in male paranoid schizophrenia: A graph-theoretical analysis. Shanghai Archives of Psychiatry. 2015; 27(3):158-66.[PMID] [PMCID]
- Ghaemmagham Farahani Z, Khodabakhshei Kollai A, Barati Sedah F. [Treatment and rehabilitation schizophrenia (Persian)]. Tehran: Roshd Publisher; 2009.
- Peyvaste Negar M. [Diagnosis of schizophrenia and clinical applications of psychological tests (Persian)]. Tehran: Avaye Noor Publisher; 2012.
- Ellenbroek BA. Psychopharmacological treatment of schizophrenia: What do we have, and what could we get. Neuropharmacology. 2012; 62(3):1371-80. [DOI:10.1016/j.neuropharm.2011.03.013] [PMID]
- Ettinger U, Meyhofer I, Steffens M, Wagner M, Koutsouleris N. Genetics, cognition, and neurobiology of schizotypal personality: A review of the overlap with schizophrenia. Frontiers in Psychiatry. 2014; 5(18):1-16. [DOI:10.3389/fpsyt.2014.00018]
- Bobes J, Arango C, Garcia-Garcia M, Rejas J. Prevalence of negative symptoms in outpatients with schizophrenia spectrum disorders treated with antipsychotics in routine clinical practice: Findings from the CLAMORS study. Journal of Clinical Psychiatry. 2010; 71(3):280-6. [DOI:10.4088/JCP.08m04250yel] [PMID]
- Kane J. Commentary: Consensus statement on negative symptoms. Schizophrenia Bulletin. 2006; 32(2):223-4. [DOI:10.1093/schbul/sbj010] [PMID] [PMCID]
- Kirkpatrick B, Fenton WS, CarpenterJr WT, Marder SR. The NIMH MATRICS consensus statement on negative symptoms. Schizophrenia Bulletin. 2006; 32(2):214-9. [DOI:10.1093/schbul/sbj053] [PMID] [PMCID]
- Mohammadi J, Narimani M, Bagyan, M. [Effects of cognitive-behavioral therapy on positive symptoms of schizophrenia (Persian)]. Urmia Medical Journal. 2014; 25(3):182-90.
- Peng SM, Koo M, Kuo JC. Effect of group music activity as an adjunctive therapy on psychotic symptoms in patients with acute schizophrenia. Archives of Psychiatric Nursing. 2010; 24(6):347-429. [DOI:10.1016/j.apnu.2010.04.001] [PMID]
- Mapar M, Golshokoh F. [The effect of music therapy on positive symptoms of schizophrenia Shafa Center in Dezful (Persian)]. New Findings in Psychology. 2009; 2(7):8-22.
- Shiou-Fang L, Chi-Hui K, Huei-Chuan S, Tsung-Cheng H, Shun-Chieh Y, Shu-Chuan Ch. Effects of group music intervention on psychiatric symptoms and depression in patient with schizophrenia. Complementary Therapies in Medicine. 2013; 21(6):682-8. [DOI:10.1016/j.ctim.2013.09.002] [PMID]
- Wichrowski M, Whiteson J, Haas F, Mola A, Rey MJ. Effects of horticultural therapy on mood and heart rate in patients participating in an inpatient cardiopulmonary rehabilitation program. Journal of Cardiopulmonary Rehabilitation. 2005; 25(5):270-4. [DOI:10.1097/00008483-200509000-00008] [PMID]
- Parvin N, Rafiee Vardanjani L, Nikfarjam M, Mohammadi A, Mahmoudi A, Deris F. [The effect of agriculture activity on quality of life in chronic schizophrenic patients (Persian)]. Iranian Journal of Psychiatric Nursing. 2014; 2(3):70-6.
- Gelkopf M, Gonen B, Kurs R, Melamed Y, Bleich A. The effect of humorous movies on in patients with chronic schizophrenia. Journal of Nervous and Mental Disease. 2006; 194(11):880-3. [DOI:10.1097/01.nmd.0000243811.29997.f7] [PMID]
- Lysaker PH, Glynn SM, Wilkniss SM, Silverstein SM. Psychotherapy and recovery from schizophrenia: A review of potential applications and need for future study. Psychological Services. 2010; 7(2):75-91. [DOI:10.1037/a0019115] [PMID] [PMCID]
- Joshua AM, Cotroneo A, Clarke S. Humor and oncology. Journal of Clinical Oncology. 2005; 23(3):645-8. [DOI:10.1200/JCO.2005.09.064] [PMID]
- Levenson RW, Miller BM. Loss of cells loss of self Frontotemporal lobar degeneration and human emotion. Current Directions Psychological Science. 2007; 15(1):289-94. [DOI:10.1111/j.1467-8721.2007.00523.x]
- Khoshoi M. [Relation beetween sense of humor and mental disorder in students in pre-university period in Isfahan city (Persian)]. Journal of Psychology of Tabriz University. 2008; 3(9):45-64.
- Bahadori-Khosroshahi J, Khanjani Z. [Relationship of humor and negative life events with depression among students (Persian)]. Zahedan Journal of Research in Medical Sciences. 2012; 14(2):96-100.
- Gelkopf M. The use of humor in serious mental illness: A review. Evidence-Based Complementary and Alternative Medicine. 2011; 2011:342837. [DOI:10.1093/ecam/nep106] [PMID] [PMCID]
- Cai C, Yu L, Rong L, Zhong H. Effectiveness of humor intervention for patients with schizophrenia: A randomized controlled trial. Journal of Psychiatric Research. 2014; 59:174-8.
- Beh-Pajooh A, Jahangiri M, Zahrakar K. [Homor skills training and reducing depression in patients with spinal cord injury (Persian)]. Developmental Psychology. 2010; 6(23):227-36.
- Shams S, Hashemyan K, Shafiabadi A. [Effectiveness of teaching methods sense of humor on despair and social adjustment depressed students in Tehran (Persian)]. Journal of Modern Thoughts in Education. 2007; 3(1):82-99.
- Narimani M, Maleki Pirbazari M, Keykhosrovani M, Barkordari F. [Applied mental tests (Persian)]. Ardabil: Mohaghegh Ardabili; 2014.
- Abolghasemi A. [The relationship metacognitive belives with positive and negative symptoms in patients with schizophrenia (Persian)]. Daneshvar-e Raftar Journal. 2007; 16(2):85-98.
- Falkenberg I, Buchkremer G, Bartels M, Wild B. Implementation of a manual-based training of humor abilities in patients with depression: A pilot study. Psychiatry Research. 2011; 186(2-3):454-7. [DOI:10.1016/j.psychres.2010.10.009]
- Amminger GP, Schäfer MR, Papageorgiou K, Klier CM, Schlögelhofer M, Mossaheb N, et al. Emotion recognition in individuals at clinical high-risk for schizophrenia. Schizophrenia Bulletin. 2011; 38(5):1030-9. [DOI:10.1093/schbul/sbr015]
- Poladie Reyshahri A, Golestane M. [Psychology humor, creativity and mental health (Persian)]. Tehran: Nasl-e Noandish Publisher; 2008.
- McGhee P. Understanding and promoting the development of children’s humor. New York: Kendall/Hunt Publishing Company; 2002.
- Abolghasemi A. [The relationship between non-verbal behaviors, emotional processing and recognition with positive and negative symptoms in pietients with schizophrenia patient (Persian)]. Journal of Rafsanjan University of Medical Sciences. 2013; 12(2):89-102.
- Rosenhan DL, Seligman MEP. Abnormal psychology: Revised in line with the new DSM-IV manual, this edition of Abnormal. New York: Norton; 2008.
- Argyle M. The psychology of happiness [F Bahrami, H Palahang, H Taher Neshat doost, M Gohari, Persian trans.]. Isfahan: Jahad Daneshghahi Isfahan Publisher; 2007.
- Erickson SJ, Feldstein SW. Adolescent humor and its relationship tocoping, defense strategies, psychological distress and well-being. Child Psychiatry & Human Development. 2006; 37(3):255-71. [DOI:10.1007/s10578-006-0034-5] [PMID]
- Lovorn MG. Humor in the home and in the classroom: The benefits of laughing while we learn. Journal of Education and Human Development. 2008; 20(1):123-33.
Article Type : Research |
Subject:
Special
Received: 2018/03/15 | Accepted: 2018/08/27 | Published: 2019/01/1
Received: 2018/03/15 | Accepted: 2018/08/27 | Published: 2019/01/1
References
1. Halgin R. Abnormal Psychology: Clinical Perspectives on Psychological Disorders [Y Seyed Mohammadi, Persian Trans.]. Tehran: Ravan Publisher; 2014.
2. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. [Y Seyed Mohammadi, Persian Trans.]. Tehran: Ravan Publisher; 2013.
3. Jianhuai CH, Zhijian YA, Jiaolong QI, Rui YA, Lingling HU, Qing LU. Abnormal inter-and intra-hemispheric integration in male paranoid schizophrenia: A graph-theoretical analysis. Shanghai Archives of Psychiatry. 2015; 27(3):158-66.[PMID] [PMCID]
4. Ghaemmagham Farahani Z, Khodabakhshei Kollai A, Barati Sedah F. [Treatment and rehabilitation schizophrenia (Persian)]. Tehran: Roshd Publisher; 2009.
5. Peyvaste Negar M. [Diagnosis of schizophrenia and clinical applications of psychological tests (Persian)]. Tehran: Avaye Noor Publisher; 2012.
6. Ellenbroek BA. Psychopharmacological treatment of schizophrenia: What do we have, and what could we get. Neuropharmacology. 2012; 62(3):1371-80. [DOI:10.1016/j.neuropharm.2011.03.013] [PMID] [DOI:10.1016/j.neuropharm.2011.03.013]
7. Ettinger U, Meyhofer I, Steffens M, Wagner M, Koutsouleris N. Genetics, cognition, and neurobiology of schizotypal personality: A review of the overlap with schizophrenia. Frontiers in Psychiatry. 2014; 5(18):1-16. [DOI:10.3389/fpsyt.2014.00018] [DOI:10.3389/fpsyt.2014.00018]
8. Bobes J, Arango C, Garcia-Garcia M, Rejas J. Prevalence of negative symptoms in outpatients with schizophrenia spectrum disorders treated with antipsychotics in routine clinical practice: Findings from the CLAMORS study. Journal of Clinical Psychiatry. 2010; 71(3):280-6. [DOI:10.4088/JCP.08m04250yel] [PMID] [DOI:10.4088/JCP.08m04250yel]
9. Kane J. Commentary: Consensus statement on negative symptoms. Schizophrenia Bulletin. 2006; 32(2):223-4. [DOI:10.1093/schbul/sbj010] [PMID] [PMCID] [DOI:10.1093/schbul/sbj010]
10. Kirkpatrick B, Fenton WS, CarpenterJr WT, Marder SR. The NIMH MATRICS consensus statement on negative symptoms. Schizophrenia Bulletin. 2006; 32(2):214-9. [DOI:10.1093/schbul/sbj053] [PMID] [PMCID] [DOI:10.1093/schbul/sbj053]
11. Mohammadi J, Narimani M, Bagyan, M. [Effects of cognitive-behavioral therapy on positive symptoms of schizophrenia (Persian)]. Urmia Medical Journal. 2014; 25(3):182-90.
12. Peng SM, Koo M, Kuo JC. Effect of group music activity as an adjunctive therapy on psychotic symptoms in patients with acute schizophrenia. Archives of Psychiatric Nursing. 2010; 24(6):347-429. [DOI:10.1016/j.apnu.2010.04.001] [PMID] [DOI:10.1016/j.apnu.2010.04.001]
13. Mapar M, Golshokoh F. [The effect of music therapy on positive symptoms of schizophrenia Shafa Center in Dezful (Persian)]. New Findings in Psychology. 2009; 2(7):8-22.
14. Shiou-Fang L, Chi-Hui K, Huei-Chuan S, Tsung-Cheng H, Shun-Chieh Y, Shu-Chuan Ch. Effects of group music intervention on psychiatric symptoms and depression in patient with schizophrenia. Complementary Therapies in Medicine. 2013; 21(6):682-8. [DOI:10.1016/j.ctim.2013.09.002] [PMID] [DOI:10.1016/j.ctim.2013.09.002]
15. Wichrowski M, Whiteson J, Haas F, Mola A, Rey MJ. Effects of horticultural therapy on mood and heart rate in patients participating in an inpatient cardiopulmonary rehabilitation program. Journal of Cardiopulmonary Rehabilitation. 2005; 25(5):270-4. [DOI:10.1097/00008483-200509000-00008] [PMID] [DOI:10.1097/00008483-200509000-00008]
16. Parvin N, Rafiee Vardanjani L, Nikfarjam M, Mohammadi A, Mahmoudi A, Deris F. [The effect of agriculture activity on quality of life in chronic schizophrenic patients (Persian)]. Iranian Journal of Psychiatric Nursing. 2014; 2(3):70-6.
17. Gelkopf M, Gonen B, Kurs R, Melamed Y, Bleich A. The effect of humorous movies on in patients with chronic schizophrenia. Journal of Nervous and Mental Disease. 2006; 194(11):880-3. [DOI:10.1097/01.nmd.0000243811.29997.f7] [PMID] [DOI:10.1097/01.nmd.0000243811.29997.f7]
18. Lysaker PH, Glynn SM, Wilkniss SM, Silverstein SM. Psychotherapy and recovery from schizophrenia: A review of potential applications and need for future study. Psychological Services. 2010; 7(2):75-91. [DOI:10.1037/a0019115] [PMID] [PMCID] [DOI:10.1037/a0019115]
19. Joshua AM, Cotroneo A, Clarke S. Humor and oncology. Journal of Clinical Oncology. 2005; 23(3):645-8. [DOI:10.1200/JCO.2005.09.064] [PMID] [DOI:10.1200/JCO.2005.09.064]
20. Levenson RW, Miller BM. Loss of cells loss of self Frontotemporal lobar degeneration and human emotion. Current Directions Psychological Science. 2007; 15(1):289-94. [DOI:10.1111/j.1467-8721.2007.00523.x] [DOI:10.1111/j.1467-8721.2007.00523.x]
21. Khoshoi M. [Relation beetween sense of humor and mental disorder in students in pre-university period in Isfahan city (Persian)]. Journal of Psychology of Tabriz University. 2008; 3(9):45-64.
22. Bahadori-Khosroshahi J, Khanjani Z. [Relationship of humor and negative life events with depression among students (Persian)]. Zahedan Journal of Research in Medical Sciences. 2012; 14(2):96-100.
23. Gelkopf M. The use of humor in serious mental illness: A review. Evidence-Based Complementary and Alternative Medicine. 2011; 2011:342837. [DOI:10.1093/ecam/nep106] [PMID] [PMCID] [DOI:10.1093/ecam/nep106]
24. Cai C, Yu L, Rong L, Zhong H. Effectiveness of humor intervention for patients with schizophrenia: A randomized controlled trial. Journal of Psychiatric Research. 2014; 59:174-8. [DOI:10.1016/j.jpsychires.2014.09.010] [PMID]
25. Beh-Pajooh A, Jahangiri M, Zahrakar K. [Homor skills training and reducing depression in patients with spinal cord injury (Persian)]. Developmental Psychology. 2010; 6(23):227-36.
26. Shams S, Hashemyan K, Shafiabadi A. [Effectiveness of teaching methods sense of humor on despair and social adjustment depressed students in Tehran (Persian)]. Journal of Modern Thoughts in Education. 2007; 3(1):82-99.
27. Narimani M, Maleki Pirbazari M, Keykhosrovani M, Barkordari F. [Applied mental tests (Persian)]. Ardabil: Mohaghegh Ardabili; 2014.
28. Abolghasemi A. [The relationship metacognitive belives with positive and negative symptoms in patients with schizophrenia (Persian)]. Daneshvar-e Raftar Journal. 2007; 16(2):85-98.
29. Falkenberg I, Buchkremer G, Bartels M, Wild B. Implementation of a manual-based training of humor abilities in patients with depression: A pilot study. Psychiatry Research. 2011; 186(2-3):454-7. [DOI:10.1016/j.psychres.2010.10.009] [DOI:10.1016/j.psychres.2010.10.009]
30. Amminger GP, Schäfer MR, Papageorgiou K, Klier CM, Schlögelhofer M, Mossaheb N, et al. Emotion recognition in individuals at clinical high-risk for schizophrenia. Schizophrenia Bulletin. 2011; 38(5):1030-9. [DOI:10.1093/schbul/sbr015] [DOI:10.1093/schbul/sbr015]
31. Poladie Reyshahri A, Golestane M. [Psychology humor, creativity and mental health (Persian)]. Tehran: Nasl-e Noandish Publisher; 2008.
32. McGhee P. Understanding and promoting the development of children's humor. New York: Kendall/Hunt Publishing Company; 2002.
33. Abolghasemi A. [The relationship between non-verbal behaviors, emotional processing and recognition with positive and negative symptoms in pietients with schizophrenia patient (Persian)]. Journal of Rafsanjan University of Medical Sciences. 2013; 12(2):89-102.
34. Rosenhan DL, Seligman MEP. Abnormal psychology: Revised in line with the new DSM-IV manual, this edition of Abnormal. New York: Norton; 2008.
35. Argyle M. The psychology of happiness [F Bahrami, H Palahang, H Taher Neshat doost, M Gohari, Persian trans.]. Isfahan: Jahad Daneshghahi Isfahan Publisher; 2007.
36. Erickson SJ, Feldstein SW. Adolescent humor and its relationship tocoping, defense strategies, psychological distress and well-being. Child Psychiatry & Human Development. 2006; 37(3):255-71. [DOI:10.1007/s10578-006-0034-5] [PMID] [DOI:10.1007/s10578-006-0034-5]
37. Lovorn MG. Humor in the home and in the classroom: The benefits of laughing while we learn. Journal of Education and Human Development. 2008; 20(1):123-33.
Send email to the article author
| Rights and permissions | |
 | This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Articles Copyright © The Author(s).
Owned by Guilan University of Medical Sciences.
Co-published by Negah Institute for Scientific Communication.
Contact Information
JHNM Office, Guilan University of Medical Sciences P.O.Box 41635-1873, Rasht, Iran
Journal Tel: +9813 33553202
Publisher Tel: +9821 453 55 555; +9821 453 55 000
Email: holisticnmj@gmail.com, nursjournal@gums.ac.ir
