Sat, May 4, 2024
Volume 28, Issue 3 (6-2018)
JHNM 2018, 28(3): 198-204 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Varvani Farahani P, Hekmat Pou D, Alhani F, Ashori M, Azadnia M. Investigating the Effect of Family-Centered Empowerment Model on the Lifestyle of Children Suffering From Leukemia. JHNM 2018; 28 (3) :198-204
URL: http://hnmj.gums.ac.ir/article-1-606-en.html
URL: http://hnmj.gums.ac.ir/article-1-606-en.html
Pouran Varvani Farahani1 

 , Davoud Hekmat Pou * 2, Fatemeh Alhani3 , Morteza Ashori4 , Mayam Azadnia5
, Davoud Hekmat Pou * 2, Fatemeh Alhani3 , Morteza Ashori4 , Mayam Azadnia5
, Davoud Hekmat Pou * 2, Fatemeh Alhani3 , Morteza Ashori4 , Mayam Azadnia5
1- Nursing (MSN), School of Nursing and Midwifery, Arak University of Medical Sciences, Arak, Iran.
2- Department of Nursing, Associate Professor, Arak University of Medical Sciences, Arak, Iran. , dr_hekmat@arakmu.ac.ir
3- Department of Nursing, Associate Professor, Tarbiat Modarres University, Tehran, Iran.
4- Nursing (BS), Arak University of Medical Sciences, Arak, Iran.
5- Nursing (BS), Amir Kabir Hospital, Arak University of Medical Sciences, Arak, Iran.
2- Department of Nursing, Associate Professor, Arak University of Medical Sciences, Arak, Iran. , dr_hekmat@arakmu.ac.ir
3- Department of Nursing, Associate Professor, Tarbiat Modarres University, Tehran, Iran.
4- Nursing (BS), Arak University of Medical Sciences, Arak, Iran.
5- Nursing (BS), Amir Kabir Hospital, Arak University of Medical Sciences, Arak, Iran.
Full-Text [PDF 417 kb]
(1176 Downloads)
| Abstract (HTML) (4304 Views)
Full-Text: (1366 Views)
Introduction
Leukemia is the most common type of cancer in children, and 80% of leukemia cases involve acute lymphoblastic leukemia while 20% cases involve acute myeloid leukemia [1]. A research conducted in Iran during 2006 to 2013 in children below 15 years of age in the city of Sari, the rate of incidence of acute lymphoblastic leukemia was reported as 86.6% and acute myeloblastic leukemia 13.6% [2].
During the recent decades, a significant improvement has been observed in the treatment of children suffering from cancer. However, children suffer from a relapse comprise a major part of the children suffering from cancer. Unfortunately, relapse is considered the most effective factor in the survival rate of patients suffering from leukemia [3]. Cancer and its treatments in children are related to physical limitations, depression, losing the experiences of childhood, stresses and harms sustained by parents and other children of the family [4]. Therefore, it is necessary that the patients should be empowered to better control the illness and enjoy a better lifestyle. Empowerment is a dynamic, positive [5, 6], interactional, and social process [7]. A process that takes shape in relation to others and leads to improvements in the quality of life, assuming responsibility, better interaction with health workers, satisfaction [8], response to treatment [9], prevention of complications, reduction of treatment costs, and positive attitude to the illness [10]. For these reasons, it is referred to as the nursing profession’s necessity [11].
Family-centered empowerment model emphasizes the individual’s role and the role of other family members in the motivational, psychological (self-belief, self-control and self-efficacy) dimension. Empowerment is the advancement of conscious efforts by the individuals to care for themselves, the families and the communities, in order to assume responsibility for promoting and maintaining their own health and the health of others [12].
The purpose of this study is to implement the empowerment model based on four stages: 1. Perceived threat (perceived severity and sensitivity - Advancement of the level of knowledge and awareness regarding the quality and the probability of developing complications; 2. Self-efficacy - Problem solving which leads to enhancement of self-esteem and self-control; 3. Self-esteem (self-belief) - Educational participation using educational cards through the children to the active family members; and 4. Process evaluation [12].
So far this model has been implemented for improving quality of life of patients suffering from chronic illness (thalassemia, epilepsy). The complicated treatment of leukemia and the chronic nature of the illness creates difficulties for the foundation of the family and affects the lifestyle of the children, family and the community as the lifestyle provides for security, preservation, and promotes health and welfare of the individual [13]. The widespread incidence of leukemia in children necessitates the empowerment of the family system. This study was conducted to determine the effect of family-centered empowerment model on improving the lifestyle of children suffering from leukemia.
Materials and Methods
This double-blind clinical trial was conducted in school-age children (8 to 12 years) suffering from leukemia and their active family members. All patients referred to the oncology ward of one of the hospitals in the city of Arak who satisfied the inclusion criteria: children aged between 8 to 12 years (school age) suffering from different types of leukemia, the child and the family’s willingness to participate in the study and cooperate, absence of any particular psychological illness as stated by the parents, the ability to take part in the empowerment program, feeling of responsibility and the ability for decision making by the active family member, were selected using the census method.
The participants were randomized into the two groups - test and control. The sampling framework for 60 people was defined, and the cards with numbers 1- 60 written were dropped into a goblet. Then the numbers were randomly pulled out and assigned to the control and test groups, respectively. Based on the number referring to the patient, their groups were specified. The Chi-square test was obtained to control the sorting out of the groups in terms of different variables. Total number of the participants based on the pilot study was 60 (30 of them children and 30 parents active family members). Fifteen children were placed in the test group and control group each. Similarly, 15 active family members (the children’s parents who participated in the study with ability, willingness and sufficient knowledge regarding the illness process) were placed in the test group and control group each.
The tools used included A) The child’s demographic information questionnaire (3 questions), and the active family member demographic information questionnaire (20 questions); B) Questionnaire evaluating the children’s lifestyle included the five dimensions of nutrition (10 questions), sleep (17 questions), physical activity (3 questions), physical health (3 questions), and stress (5 questions). Answers to the questions were fixed responses as always, often, sometimes, never, that corresponded to scores 0 to 3. The five dimensions had a total score of 114 which was categorized into three levels as unfavorable (38-63 score), average (64-88 score), and favorable (89-114 score). The lifestyle questionnaire was designed by the researchers based on related books and articles; C) Child empowerment dimensions evaluation questionnaire included seven dimensions: Control axis (1 question), perceived severity (10 questions), perceived sensitivity (10 questions), feeling of self-efficacy (10 questions), self-efficacy in the form of self-report (10 questions), the researcher observation of the child’s self-efficacy (10 questions) and self-control (4 questions). Answers to the questions were fixed responses as strongly agree, agree, don’t know, disagree, and strongly disagree each corresponded to scores 0 to 4. The questionnaire had a total score of 220 which was perceived into three levels as unfavorable (55-110), average (111-165), and favorable (166-220). The seven dimensions of the family-centered empowerment model questionnaire were designed by the researchers. D) The questionnaire on evaluation of empowerment dimensions of the active family member included eight dimensions: control axis (3 questions), perceived severity (14 questions), perceived sensitivity (20 questions), feeling of self-efficacy (11 questions), self-efficacy in the form of self-reporting (12 questions), researcher’s observation of the child’s self-efficacy (6 questions), self-esteem (34 questions), and self-control (3 questions). Answers to the questions were fixed responses as strongly agree, agree, don’t know, disagree, and strongly disagree each corresponded to scores 0 to 4. The questionnaire had a total score of 412 which was perceived into three levels as unfavorable (103-206), average (207 – 309), and favorable (310 – 412). The questionnaire was designed by the researchers based on related sources.
To determine the validity of the tools (lifestyle, family-centered empowerment, and the active family member family-centered empowerment), the Content Validity method was used. In this method, the questionnaire was prepared by considering credible sources and books and other validated questionnaires in the field. It was later reviewed by a number of professors of Arak University of Medical Sciences and Tarbiat Modarres University and needed corrections were made based on their opinions. The tools reliability was determined by conducting Test-re-test. Children and mothers (10 each) apart from participating in the study filled out the questionnaire, and after a week, the questionnaire was given back to the same persons; and each turn was verified with 95% certainty and the problems observed were resolved. The Cronbach’s alpha reliability test result for lifestyle questionnaire was 0.75, for child empowerment questionnaire 0.79 and for empowering the child’s caregiver questionnaire 0.76.
Guidance was provided to the participants in case they face any difficulty while filling out the questionnaires. The questionnaire on the patients’ demographic information and the questionnaire on the lifestyle of the patient prior to the intervention were filled out by the participants in both groups. Also, the questionnaire on the demographic information of the active family member was completed by the children’s caregivers prior to intervention in both the groups. The data collected were statistically analyzed, and empowerment program was reviewed for implementation. Prior to intervention data identified sources, limitations, needs, and points of strength and weakness in various fields; changes were implemented in the empowerment program to be suitable with the needs and aims of the research. After the pre-test, the intervention was employed in the test group. The control group did not receive any intervention.
In the test group, the family-centered empowerment model was implemented through group discussion 3 – 5 sessions for the children (30 minutes) and parents (one hour) in the ward by the researcher’s colleague who is a nursing expert and has years of experience at the oncology ward.
The family-centered empowerment program was implemented in following steps: 1. Perceiving threat: The group discussion sessions with participant children and their active family members were conducted with the objective of increasing the perceived severity through increasing the knowledge and awareness about the illness, its complications and its treatment process. The perceived sensitivity was improved through upgrading their recognition of their conditions.
2. Self-efficacy: Problem solving through the scientific display of required skills to the children (for example: performing the relaxation technique and temperature control) to increase participation in solving problems was carried out in groups to increase self-efficacy, self-esteem, and self-control. At this stage, the children and parents become aware of the illness process and its complications, participated with self-confidence and the feeling that: I can have a role in improving my condition.
3. Educational participation: The children were encouraged to convey what they have learned to the active family member through educational cards. These cards were given to them at the conclusion of each previous session. The ability to carry out this responsibility and their belief in their knowledge of the illness and conveying this knowledge to others is believed to enhance their self-esteem.
4. Evaluation: This step included evaluation of the process of each session in order to ensure the participation in the care program and the necessary follow-ups. Two or three questions were asked verbally to the participants on the issues discussed in the previous session.
5. The final evaluation: The participants performed the acquired skills, and after one month of implementing the family-centered empowerment model, its effectiveness was evaluated. The participant children filled out the questionnaire on the child’s lifestyle in both groups.
This research was approved by Arak Medical Sciences University Research Council (approval number 748), and Medical Researches Department (ethics code number: IR.ARAKMU.REC.1391.130). The data was analyzed using SPSS version 20 and the descriptive statistics, chi-square test, paired t-test and independent t-test at the significance level (P<0.05).
Results
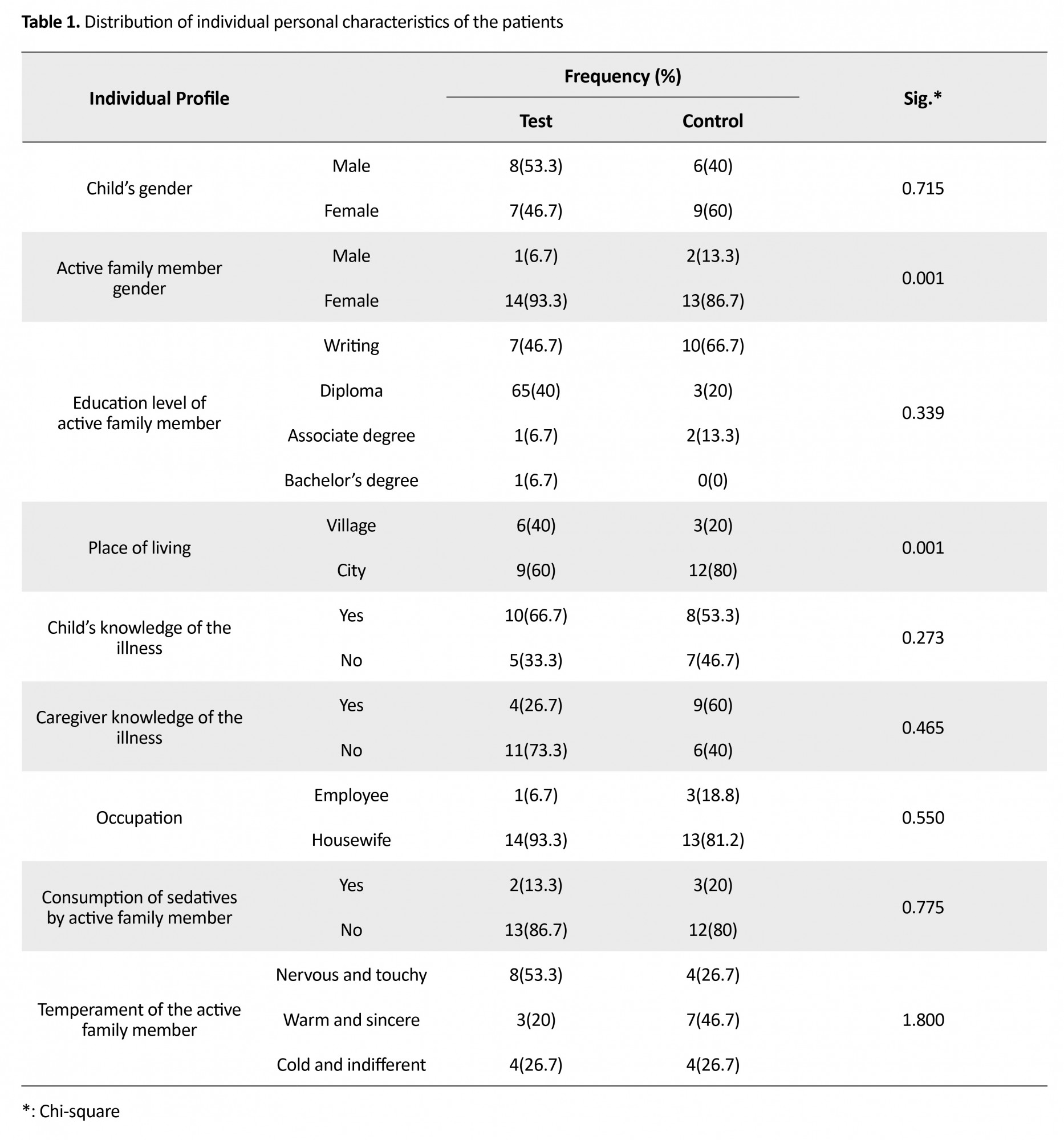
In this study, 30 children suffering from leukemia and 30 parents of these children participated. There was no significant difference between the test and control group in the gender of the children (P=0.715) and age. Most of the active family members in the control group (86.7%) and in the test group (93.3%) were females. In the test group, the mean±SD age of children was 10.3±0.49 and of the active family member was 42.5±5.13. In the control group, the mean±SD of children was 9.6±1.39 and of the active family member was 39.6±4.51. Most active family members had an education level of reading and writing ability, married, had local residence in the city, housewife, and were not using tranquilizers and sedatives and anti-stress drugs. There were no significant differences between the two groups in terms of educational level, employment status, and temperament. Also, statistical test prior to intervention did not show a significant difference between the two groups in knowledge levels of the children and the active family member about the illness (P>0.05). Table 1 shows the demographic specifications of the children suffering from leukemia and their parents in both groups, i.e., test and control, using descriptive statistics of frequencies and its percentage.
Leukemia is the most common type of cancer in children, and 80% of leukemia cases involve acute lymphoblastic leukemia while 20% cases involve acute myeloid leukemia [1]. A research conducted in Iran during 2006 to 2013 in children below 15 years of age in the city of Sari, the rate of incidence of acute lymphoblastic leukemia was reported as 86.6% and acute myeloblastic leukemia 13.6% [2].
During the recent decades, a significant improvement has been observed in the treatment of children suffering from cancer. However, children suffer from a relapse comprise a major part of the children suffering from cancer. Unfortunately, relapse is considered the most effective factor in the survival rate of patients suffering from leukemia [3]. Cancer and its treatments in children are related to physical limitations, depression, losing the experiences of childhood, stresses and harms sustained by parents and other children of the family [4]. Therefore, it is necessary that the patients should be empowered to better control the illness and enjoy a better lifestyle. Empowerment is a dynamic, positive [5, 6], interactional, and social process [7]. A process that takes shape in relation to others and leads to improvements in the quality of life, assuming responsibility, better interaction with health workers, satisfaction [8], response to treatment [9], prevention of complications, reduction of treatment costs, and positive attitude to the illness [10]. For these reasons, it is referred to as the nursing profession’s necessity [11].
Family-centered empowerment model emphasizes the individual’s role and the role of other family members in the motivational, psychological (self-belief, self-control and self-efficacy) dimension. Empowerment is the advancement of conscious efforts by the individuals to care for themselves, the families and the communities, in order to assume responsibility for promoting and maintaining their own health and the health of others [12].
The purpose of this study is to implement the empowerment model based on four stages: 1. Perceived threat (perceived severity and sensitivity - Advancement of the level of knowledge and awareness regarding the quality and the probability of developing complications; 2. Self-efficacy - Problem solving which leads to enhancement of self-esteem and self-control; 3. Self-esteem (self-belief) - Educational participation using educational cards through the children to the active family members; and 4. Process evaluation [12].
So far this model has been implemented for improving quality of life of patients suffering from chronic illness (thalassemia, epilepsy). The complicated treatment of leukemia and the chronic nature of the illness creates difficulties for the foundation of the family and affects the lifestyle of the children, family and the community as the lifestyle provides for security, preservation, and promotes health and welfare of the individual [13]. The widespread incidence of leukemia in children necessitates the empowerment of the family system. This study was conducted to determine the effect of family-centered empowerment model on improving the lifestyle of children suffering from leukemia.
Materials and Methods
This double-blind clinical trial was conducted in school-age children (8 to 12 years) suffering from leukemia and their active family members. All patients referred to the oncology ward of one of the hospitals in the city of Arak who satisfied the inclusion criteria: children aged between 8 to 12 years (school age) suffering from different types of leukemia, the child and the family’s willingness to participate in the study and cooperate, absence of any particular psychological illness as stated by the parents, the ability to take part in the empowerment program, feeling of responsibility and the ability for decision making by the active family member, were selected using the census method.
The participants were randomized into the two groups - test and control. The sampling framework for 60 people was defined, and the cards with numbers 1- 60 written were dropped into a goblet. Then the numbers were randomly pulled out and assigned to the control and test groups, respectively. Based on the number referring to the patient, their groups were specified. The Chi-square test was obtained to control the sorting out of the groups in terms of different variables. Total number of the participants based on the pilot study was 60 (30 of them children and 30 parents active family members). Fifteen children were placed in the test group and control group each. Similarly, 15 active family members (the children’s parents who participated in the study with ability, willingness and sufficient knowledge regarding the illness process) were placed in the test group and control group each.
The tools used included A) The child’s demographic information questionnaire (3 questions), and the active family member demographic information questionnaire (20 questions); B) Questionnaire evaluating the children’s lifestyle included the five dimensions of nutrition (10 questions), sleep (17 questions), physical activity (3 questions), physical health (3 questions), and stress (5 questions). Answers to the questions were fixed responses as always, often, sometimes, never, that corresponded to scores 0 to 3. The five dimensions had a total score of 114 which was categorized into three levels as unfavorable (38-63 score), average (64-88 score), and favorable (89-114 score). The lifestyle questionnaire was designed by the researchers based on related books and articles; C) Child empowerment dimensions evaluation questionnaire included seven dimensions: Control axis (1 question), perceived severity (10 questions), perceived sensitivity (10 questions), feeling of self-efficacy (10 questions), self-efficacy in the form of self-report (10 questions), the researcher observation of the child’s self-efficacy (10 questions) and self-control (4 questions). Answers to the questions were fixed responses as strongly agree, agree, don’t know, disagree, and strongly disagree each corresponded to scores 0 to 4. The questionnaire had a total score of 220 which was perceived into three levels as unfavorable (55-110), average (111-165), and favorable (166-220). The seven dimensions of the family-centered empowerment model questionnaire were designed by the researchers. D) The questionnaire on evaluation of empowerment dimensions of the active family member included eight dimensions: control axis (3 questions), perceived severity (14 questions), perceived sensitivity (20 questions), feeling of self-efficacy (11 questions), self-efficacy in the form of self-reporting (12 questions), researcher’s observation of the child’s self-efficacy (6 questions), self-esteem (34 questions), and self-control (3 questions). Answers to the questions were fixed responses as strongly agree, agree, don’t know, disagree, and strongly disagree each corresponded to scores 0 to 4. The questionnaire had a total score of 412 which was perceived into three levels as unfavorable (103-206), average (207 – 309), and favorable (310 – 412). The questionnaire was designed by the researchers based on related sources.
To determine the validity of the tools (lifestyle, family-centered empowerment, and the active family member family-centered empowerment), the Content Validity method was used. In this method, the questionnaire was prepared by considering credible sources and books and other validated questionnaires in the field. It was later reviewed by a number of professors of Arak University of Medical Sciences and Tarbiat Modarres University and needed corrections were made based on their opinions. The tools reliability was determined by conducting Test-re-test. Children and mothers (10 each) apart from participating in the study filled out the questionnaire, and after a week, the questionnaire was given back to the same persons; and each turn was verified with 95% certainty and the problems observed were resolved. The Cronbach’s alpha reliability test result for lifestyle questionnaire was 0.75, for child empowerment questionnaire 0.79 and for empowering the child’s caregiver questionnaire 0.76.
Guidance was provided to the participants in case they face any difficulty while filling out the questionnaires. The questionnaire on the patients’ demographic information and the questionnaire on the lifestyle of the patient prior to the intervention were filled out by the participants in both groups. Also, the questionnaire on the demographic information of the active family member was completed by the children’s caregivers prior to intervention in both the groups. The data collected were statistically analyzed, and empowerment program was reviewed for implementation. Prior to intervention data identified sources, limitations, needs, and points of strength and weakness in various fields; changes were implemented in the empowerment program to be suitable with the needs and aims of the research. After the pre-test, the intervention was employed in the test group. The control group did not receive any intervention.
In the test group, the family-centered empowerment model was implemented through group discussion 3 – 5 sessions for the children (30 minutes) and parents (one hour) in the ward by the researcher’s colleague who is a nursing expert and has years of experience at the oncology ward.
The family-centered empowerment program was implemented in following steps: 1. Perceiving threat: The group discussion sessions with participant children and their active family members were conducted with the objective of increasing the perceived severity through increasing the knowledge and awareness about the illness, its complications and its treatment process. The perceived sensitivity was improved through upgrading their recognition of their conditions.
2. Self-efficacy: Problem solving through the scientific display of required skills to the children (for example: performing the relaxation technique and temperature control) to increase participation in solving problems was carried out in groups to increase self-efficacy, self-esteem, and self-control. At this stage, the children and parents become aware of the illness process and its complications, participated with self-confidence and the feeling that: I can have a role in improving my condition.
3. Educational participation: The children were encouraged to convey what they have learned to the active family member through educational cards. These cards were given to them at the conclusion of each previous session. The ability to carry out this responsibility and their belief in their knowledge of the illness and conveying this knowledge to others is believed to enhance their self-esteem.
4. Evaluation: This step included evaluation of the process of each session in order to ensure the participation in the care program and the necessary follow-ups. Two or three questions were asked verbally to the participants on the issues discussed in the previous session.
5. The final evaluation: The participants performed the acquired skills, and after one month of implementing the family-centered empowerment model, its effectiveness was evaluated. The participant children filled out the questionnaire on the child’s lifestyle in both groups.
This research was approved by Arak Medical Sciences University Research Council (approval number 748), and Medical Researches Department (ethics code number: IR.ARAKMU.REC.1391.130). The data was analyzed using SPSS version 20 and the descriptive statistics, chi-square test, paired t-test and independent t-test at the significance level (P<0.05).
Results
In this study, 30 children suffering from leukemia and 30 parents of these children participated. There was no significant difference between the test and control group in the gender of the children (P=0.715) and age. Most of the active family members in the control group (86.7%) and in the test group (93.3%) were females. In the test group, the mean±SD age of children was 10.3±0.49 and of the active family member was 42.5±5.13. In the control group, the mean±SD of children was 9.6±1.39 and of the active family member was 39.6±4.51. Most active family members had an education level of reading and writing ability, married, had local residence in the city, housewife, and were not using tranquilizers and sedatives and anti-stress drugs. There were no significant differences between the two groups in terms of educational level, employment status, and temperament. Also, statistical test prior to intervention did not show a significant difference between the two groups in knowledge levels of the children and the active family member about the illness (P>0.05). Table 1 shows the demographic specifications of the children suffering from leukemia and their parents in both groups, i.e., test and control, using descriptive statistics of frequencies and its percentage.
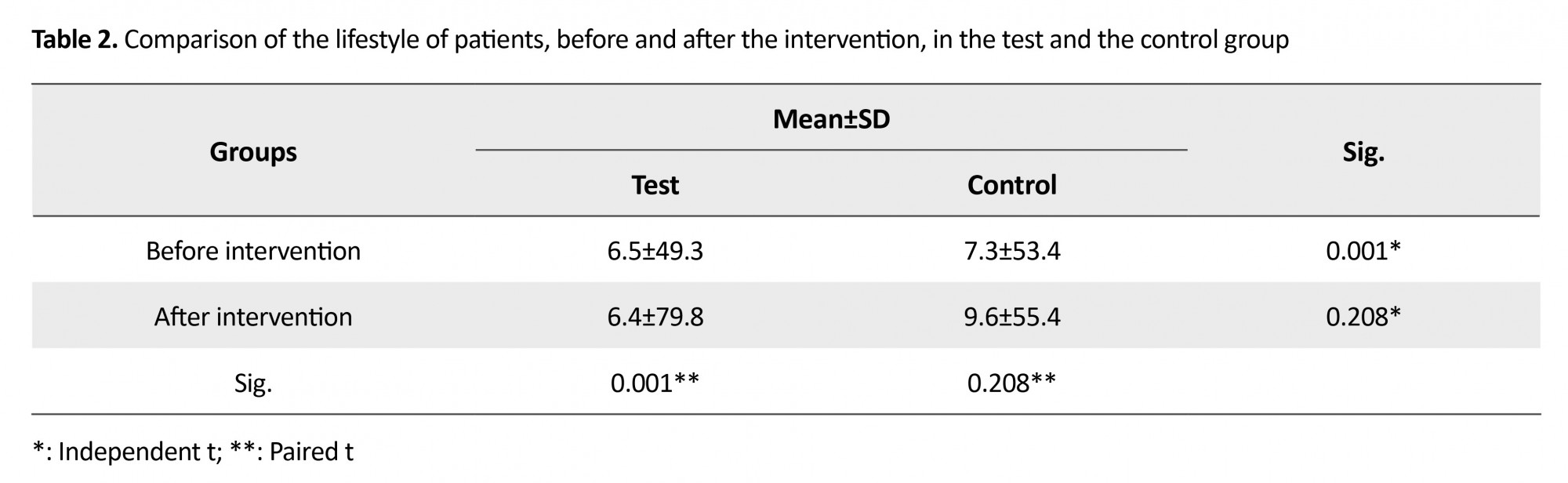
The mean±SD lifestyle before and after the intervention in the test group changed from 49.3±6.5 to 79.8±6.4 and that in the control group changed from 53.4±7.3 to 55.4±9.6. Result of paired- t-test showed a significant difference between the mean lifestyle in the test group before and after intervention (P˂0.001). However, there was no significant difference between the mean lifestyle of the control group before and after intervention (P=0.208). Also, the results of the independent t-test showed a significant difference between the two groups in terms of the mean score of lifestyle after intervention (P˂0.001) when there was no significant difference between the two groups before intervention (P=0.119) (Table 2).
Discussion
In this study, the effect of family-centered empowerment model on the lifestyle of children suffering from leukemia was examined in comparison with the control group. The results showed that there was no significant difference in the control group in terms of mean lifestyle before and after the intervention. However, there was a significant difference between the mean lifestyle of the test group before and after the intervention. These findings indicate the effectiveness of family-centered empowerment model on improving the lifestyle of children suffering from leukemia. Vahedian et. al., in a study on 70 patients suffering from cardiac infarction, found similar results [14]. Several other studies [15-22] showed results similar to other chronic illnesses. Chen and Li et. al. considered empowerment interventions useful in improving the quality of life in patients suffering from chronic illnesses [23]. Karimi Monaghi et. al. demonstrated positive the effect of family-centered empowerment model on quality of life of patients suffering from multiple sclerosis, and writes: “This model in terms of the need for shorter time for implementation and lesser cost and involvement of the family in implementation, is superior to other plans” [24].
Assuming responsibility by the individual for the sake of his or her health is a requisite part of any plan for change. In fact, it is the key point of the family-centered empowerment model. In this model, the cornerstone of empowering the patients is the patients themselves, and not the researcher. The researcher accompanies the patient in all of the stages; however, the tasks and the needed care to achieve favorably and desired conditions are performed by the patients themselves. The results of the study by Graves and Shelton showed that empowerment has led to positive change in the functions of the child and significant improvement in the children’s behavioral problems [25]. In the family-centered cares, there are also references to the importance of participation by parents in medical cares. For example, Holm in his findings refers to the importance of the need to use family-centered aspects in the treatment of children suffering from cancer, with support and strengthening the active involvement by parents in treatment and management of treatment of the children [26].
In this investigation, the total mean score of the lifestyle of patients showed an unfavorable lifestyle before intervention in both the groups. The change in this score after intervention showed that lifestyle improved to the medium level. The results of Khanjari's study emphasized on unfavorable condition of children who suffer from leukemia [27]. The results obtained by Wahnefried et. al. also showed that by intervention to change the behavior of patients suffering from cancer, regarding weight control, food diet, exercise and withdrawing from smoking, led to improvement in the health of these patients [28]. These results demonstrate that one of the main objectives in the treatment of patients suffering from leukemia is to improve their lifestyle.
The family-centered empowerment model helps the patients and their families to identify their imperfections and shortcomings and have sufficient power to change their current condition. This feeling of ability is achieved through information, support, and skills that improve the patient’s condition. As results showed, implementation of the family-centered empowerment model was effective in elevating the lifestyle of school-age children suffering from leukemia; it is also recommended other patients suffering from leukemia.
Generally, it can be said that empowerment of the family is an important method for improving care services, continuity of cares by the patients themselves and for participation by members of their family. Therefore, it is recommended that this model should be used for other illnesses as well. The limitations of this study were the small number of participants.
Ethical Considerations
Compliance with ethical guidelines
This research proposal was approved by the Research Council elsewhere in terms of ethical considerations. The subjects (parents) were informed about the purpose and method of the study. They were assured that they could withdraw from the study at any time without being penalized. Lastly, written informed consent was obtained from the nurses who willingly declared their participation in the study.
Funding
We express our thanks to the Office of Assistant Dean for Research and the Student Research Committee of Arak Medical Sciences University for their ample assistance and also for providing the budget for conducting this study.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
Authors of this study hereby express their gratitude toward the personnel of the oncology department of Amirkabir Hospital and also toward all the children and parents participating in this study who cooperated in completing the questionnaires. We also sincerely express our thanks to Tarbiat Modarres University Research Office for their participation in this project.
References
In this study, the effect of family-centered empowerment model on the lifestyle of children suffering from leukemia was examined in comparison with the control group. The results showed that there was no significant difference in the control group in terms of mean lifestyle before and after the intervention. However, there was a significant difference between the mean lifestyle of the test group before and after the intervention. These findings indicate the effectiveness of family-centered empowerment model on improving the lifestyle of children suffering from leukemia. Vahedian et. al., in a study on 70 patients suffering from cardiac infarction, found similar results [14]. Several other studies [15-22] showed results similar to other chronic illnesses. Chen and Li et. al. considered empowerment interventions useful in improving the quality of life in patients suffering from chronic illnesses [23]. Karimi Monaghi et. al. demonstrated positive the effect of family-centered empowerment model on quality of life of patients suffering from multiple sclerosis, and writes: “This model in terms of the need for shorter time for implementation and lesser cost and involvement of the family in implementation, is superior to other plans” [24].
Assuming responsibility by the individual for the sake of his or her health is a requisite part of any plan for change. In fact, it is the key point of the family-centered empowerment model. In this model, the cornerstone of empowering the patients is the patients themselves, and not the researcher. The researcher accompanies the patient in all of the stages; however, the tasks and the needed care to achieve favorably and desired conditions are performed by the patients themselves. The results of the study by Graves and Shelton showed that empowerment has led to positive change in the functions of the child and significant improvement in the children’s behavioral problems [25]. In the family-centered cares, there are also references to the importance of participation by parents in medical cares. For example, Holm in his findings refers to the importance of the need to use family-centered aspects in the treatment of children suffering from cancer, with support and strengthening the active involvement by parents in treatment and management of treatment of the children [26].
In this investigation, the total mean score of the lifestyle of patients showed an unfavorable lifestyle before intervention in both the groups. The change in this score after intervention showed that lifestyle improved to the medium level. The results of Khanjari's study emphasized on unfavorable condition of children who suffer from leukemia [27]. The results obtained by Wahnefried et. al. also showed that by intervention to change the behavior of patients suffering from cancer, regarding weight control, food diet, exercise and withdrawing from smoking, led to improvement in the health of these patients [28]. These results demonstrate that one of the main objectives in the treatment of patients suffering from leukemia is to improve their lifestyle.
The family-centered empowerment model helps the patients and their families to identify their imperfections and shortcomings and have sufficient power to change their current condition. This feeling of ability is achieved through information, support, and skills that improve the patient’s condition. As results showed, implementation of the family-centered empowerment model was effective in elevating the lifestyle of school-age children suffering from leukemia; it is also recommended other patients suffering from leukemia.
Generally, it can be said that empowerment of the family is an important method for improving care services, continuity of cares by the patients themselves and for participation by members of their family. Therefore, it is recommended that this model should be used for other illnesses as well. The limitations of this study were the small number of participants.
Ethical Considerations
Compliance with ethical guidelines
This research proposal was approved by the Research Council elsewhere in terms of ethical considerations. The subjects (parents) were informed about the purpose and method of the study. They were assured that they could withdraw from the study at any time without being penalized. Lastly, written informed consent was obtained from the nurses who willingly declared their participation in the study.
Funding
We express our thanks to the Office of Assistant Dean for Research and the Student Research Committee of Arak Medical Sciences University for their ample assistance and also for providing the budget for conducting this study.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
Authors of this study hereby express their gratitude toward the personnel of the oncology department of Amirkabir Hospital and also toward all the children and parents participating in this study who cooperated in completing the questionnaires. We also sincerely express our thanks to Tarbiat Modarres University Research Office for their participation in this project.
References
- William CM, William A. The leukemias: In: Behrman RE, Kingdom RM, Jenson HB, editors. Nelson of pediatrics. Philadelphia, Pennsylvania: Walter Burns Saunders; 2011.
- Mousavinasab SN, Yazdani Cherati J, Karami H, Khaksar Sh. [Risk factors influencing the survival of pediatric acute leukemia using competing risk model (Persian)]. Journal of Mazandaran University of Medical Sciences. 2015; 24(121):31-8.
- Almasi-Hashiani A, Zareifar S, Hashemi-Teir A. [Survival rate among children with acute lymphoblastic leukemia based on their relapse status in Shiraz Shahid Faghihi hospital during 2004-9 (Persian)]. Feyz Journal of Kashan University of Medical Sciences. 2012; 16(3):248-53.
- Bhatia S. Disparities in cancer outcomes: Lessons learned from children with cancer. Pediatric Blood & Cancer. 2011; 56(6):994–1002. [DOI:10.1002/pbc.23078] [PMID] [PMCID]
- Changizi A, Zeighami R, Mirzaei E, Alipour M. Family-oriented empowerment model influencing quality of life CABG patients. Journal of Nursing and Midwifery Sciences. 2014; 1(2):14-23. [DOI:10.18869/acadpub.jnms.1.2.14]
- Wahlin I, Idvall E. Patient empowerment in intensive care: An interview study. Intensive and Critical Care Nursing. 2006; 22(6):370-7. [DOI:10.1016/j.iccn.2006.05.003] [PMID]
- Harn P. The empowerment model of parent consultation with the positive psychology perspective. The European Journal of Social & Behavioural Sciences. 2013; 5(2):914–9. [DOI:10.15405/ejsbs.65]
- Small N, Bower P, Chew-Graham CA, Whalley D , Protheroe J. Patient empowerment in long-term conditions: Development and preliminary testing of a new measure. Health Services Research 2013; 13:263. [DOI:10.1186/1472-6963-13-263] [PMID] [PMCID]
- Samuel PS, Rillotta F, Brown I. The development of family quality of life concepts and measure. Journal of Intellectual Disability Research. 2012; 56(1):1-16. [DOI:10.1111/j.1365-2788.2011.01486.x] [PMID]
- Anderson RM, Funnell MM. Patient empowerment reflections on the challenge of fostering: The adopting of a new paradigm. Patient Education and Counseling. 2005; 5(2):153-7. [DOI:10.1016/j.pec.2004.05.008] [PMID]
- McCorkle R, Ercolano E, Lazenby M, Schulman-Green D, Schilling LS, Lorig K, et al. Self-Management: Enabling and Empowering Patients Living With Cancer as a Chronic Illness. CA: A Cancer Journal for Clinicians. 2011; 61(1):50-62. [DOI:10.3322/caac.20093] [PMID] [PMCID]
- Alhani F, Niknami Sh, Kimiagar M, Kazemnezhad A, Heidarnia A. [Designing of family based empowering model and evaluation of its effect on prevention of iron deficiency anemia in teenager girls (Persian)]. Pejouhandeh Journal. 2003; 8(4):283-9.
- Eshaghi Q, Farajzadegan Z, Babak A. [Healthy lifestyle assessment questionnaire in elderly: Translation, reliability and validity (Persian)]. Payesh Journal. 2009; 9(1):91-9.
- Vahedian Azimi A, Alhani F, Ahmadi F, Kazemnejad A. Effect of family-oriented empowerment model on the life style of myocardial infarction patients. Iranian Journal of Critical Care Nursing. 2010; 2(4):127-32.
- Allahyari A, Alhani F, Kazemnejad A, Izadyar M. [The effect of family centered empowerment model on the quality of life of school-age B-thalassemic children (Persian)]. Iranian Journal of Pediatrics. 2006; 16(4):455-61.
- Seyed Nematollah Roshan F, Navipor H, Alhani F. [Effect of Family-Centered Empowerment Model (FCEM) on quality of life of mothers having teenagers with iron deficiency anemia (Persian)]. Journal of Nursing Education. 2014; 3(2):27-40.
- Teymouri F, Alhani F, Kazemnejad A. [The effect of family-centered empowerment model on the Quality of life of school-age asthma children (Persian)]. Iranian Journal of Nursing Research. 2011; 6(20):52-63.
- Rajabi R, Sabzevari S, Borhani F, Haghdoost AA, Bazargan N. [The effect of family-centered Empowerment Model on quality of life of school age children with asthma (Persian)]. Journal of Health Promotion Management. 2013; 2(4):7-15.
- Stang I, Mittelmark MB. Learning as an empowerment process in breast cancer self-help groups. Journal of Clinical Nursing. 2008; 18(14):2049–57. [DOI:10.1111/j.1365-2702.2008.02320.x] [PMID]
- Masoodi R, Alhani F, Moghaddasi J, Ghorbani M. [The effect of family-centered empowerment model on skill, attitude, and knowledge of multiple sclerosis caregivers (Persian)]. Journal of Birjand University of Medical Sciences. 2010; 17(2):87-97.
- Heidari M, Alhani F, Kazem Nejad A, Moezzi F. [Effect of empowerment model on quality of life in adolescents with diabetes (Persian)]. Iranian Journal of Pediatrics. 2007; 17(1):87-94.
- Masoudi R, Soleimani MA, Hasheminia AM, Qorbani M, Dehkordi Pour AH, Bahrami N. [The effect of family centered empowerment model on quality of life in elderly people (Persian)]. Journal of Qazvin University of Medical Science. 2010; 14(1):57-64.
- Chen YC, Li IC. Effectiveness of interventions using empowerment concept for Patients with chronic disease: A systematic review. JBI Library of Systematic Reviews. 2009; 7(27):1177–1232. [PMID]
- Karimi Monaghi H, Haresabadi M, Foroghipor M, Zarifnejad GH, Mazloum SR, Alhani F. [The effect of family-centered empowerment model on the quality of life of patient with multiple sclerosis (Persian)]. Journal of Mashhad School of Nursing & Midwifery. 2009; 9(3):8-14.
- Graves KN, Shelton TL. Family empowerment as a mediator between family-centered systems of care and changes in child functioning: Identifying an important mechanism of change. Journal of Child and Family Studies. 2007; 16(4):556-66. [DOI:10.1007/s10826-006-9106-1]
- Holm KE, Patterson JM, Gurney JG. Parental involvement and family-centered care in the diagnostic and treatment phases of childhood cancer: results from a qualitative study. Journal of Pediatric oncology Nursing. 2003; 20(6):301-13. [DOI:10.1177/1043454203254984] [PMID]
- Khanjari S, Seyedfatemi N, Borji S, Haghani H. [Effect of coping skills training on quality of life among parents of children with leukemia (Persian)]. Hayat. 2013; 19(4):15-25.
- Wahnefried WD, Jones LW. Promoting a healthy lifestyle among cancer survivors. Hematology/Oncology Clinics of North America. 2008; 22(2):319-42. [DOI:10.1016/j.hoc.2008.01.012] [PMID] [PMCID]
Article Type : Research |
Subject:
Special
Received: 2016/01/9 | Accepted: 2016/05/9 | Published: 2018/06/15
Received: 2016/01/9 | Accepted: 2016/05/9 | Published: 2018/06/15
References
1. William CM, William A. The leukemias: In: Behrman RE, Kingdom RM, Jenson HB, editors. Nelson of pediatrics. Philadelphia, Pennsylvania: Walter Burns Saunders; 2011.
2. Mousavinasab SN, Yazdani Cherati J, Karami H, Khaksar Sh. [Risk factors influencing the survival of pediatric acute leukemia using competing risk model (Persian)]. Journal of Mazandaran University of Medical Sciences. 2015; 24(121):31-8.
3. Almasi-Hashiani A, Zareifar S, Hashemi-Teir A. [Survival rate among children with acute lymphoblastic leukemia based on their relapse status in Shiraz Shahid Faghihi hospital during 2004-9 (Persian)]. Feyz Journal of Kashan University of Medical Sciences. 2012; 16(3):248-53.
4. Bhatia S. Disparities in cancer outcomes: Lessons learned from children with cancer. Pediatric Blood & Cancer. 2011; 56(6):994–1002. [DOI:10.1002/pbc.23078] [PMID] [PMCID] [DOI:10.1002/pbc.23078]
5. Changizi A, Zeighami R, Mirzaei E, Alipour M. Family-oriented empowerment model influencing quality of life CABG patients. Journal of Nursing and Midwifery Sciences. 2014; 1(2):14-23. [DOI:10.18869/acadpub.jnms.1.2.14] [DOI:10.18869/acadpub.jnms.1.2.14]
6. Wahlin I, Idvall E. Patient empowerment in intensive care: An interview study. Intensive and Critical Care Nursing. 2006; 22(6):370-7. [DOI:10.1016/j.iccn.2006.05.003] [PMID] [DOI:10.1016/j.iccn.2006.05.003]
7. Harn P. The empowerment model of parent consultation with the positive psychology perspective. The European Journal of Social & Behavioural Sciences. 2013; 5(2):914–9. [DOI:10.15405/ejsbs.65] [DOI:10.15405/ejsbs.65]
8. Small N, Bower P, Chew-Graham CA, Whalley D , Protheroe J. Patient empowerment in long-term conditions: Development and preliminary testing of a new measure. Health Services Research 2013; 13:263. [DOI:10.1186/1472-6963-13-263] [PMID] [PMCID] [DOI:10.1186/1472-6963-13-263]
9. Samuel PS, Rillotta F, Brown I. The development of family quality of life concepts and measure. Journal of Intellectual Disability Research. 2012; 56(1):1-16. [DOI:10.1111/j.1365-2788.2011.01486.x] [PMID] [DOI:10.1111/j.1365-2788.2011.01486.x]
10. Anderson RM, Funnell MM. Patient empowerment reflections on the challenge of fostering: The adopting of a new paradigm. Patient Education and Counseling. 2005; 5(2):153-7. [DOI:10.1016/j.pec.2004.05.008] [PMID] [DOI:10.1016/j.pec.2004.05.008]
11. McCorkle R, Ercolano E, Lazenby M, Schulman-Green D, Schilling LS, Lorig K, et al. Self-Management: Enabling and Empowering Patients Living With Cancer as a Chronic Illness. CA: A Cancer Journal for Clinicians. 2011; 61(1):50-62. [DOI:10.3322/caac.20093] [PMID] [PMCID] [DOI:10.3322/caac.20093]
12. Alhani F, Niknami Sh, Kimiagar M, Kazemnezhad A, Heidarnia A. [Designing of family based empowering model and evaluation of its effect on prevention of iron deficiency anemia in teenager girls (Persian)]. Pejouhandeh Journal. 2003; 8(4):283-9.
13. Eshaghi Q, Farajzadegan Z, Babak A. [Healthy lifestyle assessment questionnaire in elderly: Translation, reliability and validity (Persian)]. Payesh Journal. 2009; 9(1):91-9.
14. Vahedian Azimi A, Alhani F, Ahmadi F, Kazemnejad A. Effect of family-oriented empowerment model on the life style of myocardial infarction patients. Iranian Journal of Critical Care Nursing. 2010; 2(4):127-32.
15. Allahyari A, Alhani F, Kazemnejad A, Izadyar M. [The effect of family centered empowerment model on the quality of life of school-age B-thalassemic children (Persian)]. Iranian Journal of Pediatrics. 2006; 16(4):455-61.
16. Seyed Nematollah Roshan F, Navipor H, Alhani F. [Effect of Family-Centered Empowerment Model (FCEM) on quality of life of mothers having teenagers with iron deficiency anemia (Persian)]. Journal of Nursing Education. 2014; 3(2):27-40.
17. Teymouri F, Alhani F, Kazemnejad A. [The effect of family-centered empowerment model on the Quality of life of school-age asthma children (Persian)]. Iranian Journal of Nursing Research. 2011; 6(20):52-63.
18. Rajabi R, Sabzevari S, Borhani F, Haghdoost AA, Bazargan N. [The effect of family-centered Empowerment Model on quality of life of school age children with asthma (Persian)]. Journal of Health Promotion Management. 2013; 2(4):7-15.
19. Stang I, Mittelmark MB. Learning as an empowerment process in breast cancer self-help groups. Journal of Clinical Nursing. 2008; 18(14):2049–57. [DOI:10.1111/j.1365-2702.2008.02320.x] [PMID] [DOI:10.1111/j.1365-2702.2008.02320.x]
20. Masoodi R, Alhani F, Moghaddasi J, Ghorbani M. [The effect of family-centered empowerment model on skill, attitude, and knowledge of multiple sclerosis caregivers (Persian)]. Journal of Birjand University of Medical Sciences. 2010; 17(2):87-97.
21. Heidari M, Alhani F, Kazem Nejad A, Moezzi F. [Effect of empowerment model on quality of life in adolescents with diabetes (Persian)]. Iranian Journal of Pediatrics. 2007; 17(1):87-94.
22. Masoudi R, Soleimani MA, Hasheminia AM, Qorbani M, Dehkordi Pour AH, Bahrami N. [The effect of family centered empowerment model on quality of life in elderly people (Persian)]. Journal of Qazvin University of Medical Science. 2010; 14(1):57-64.
23. Chen YC, Li IC. Effectiveness of interventions using empowerment concept for Patients with chronic disease: A systematic review. JBI Library of Systematic Reviews. 2009; 7(27):1177–1232. [PMID] [DOI:10.11124/01938924-200907270-00001]
24. Karimi Monaghi H, Haresabadi M, Foroghipor M, Zarifnejad GH, Mazloum SR, Alhani F. [The effect of family-centered empowerment model on the quality of life of patient with multiple sclerosis (Persian)]. Journal of Mashhad School of Nursing & Midwifery. 2009; 9(3):8-14.
25. Graves KN, Shelton TL. Family empowerment as a mediator between family-centered systems of care and changes in child functioning: Identifying an important mechanism of change. Journal of Child and Family Studies. 2007; 16(4):556-66. [DOI:10.1007/s10826-006-9106-1] [DOI:10.1007/s10826-006-9106-1]
26. Holm KE, Patterson JM, Gurney JG. Parental involvement and family-centered care in the diagnostic and treatment phases of childhood cancer: results from a qualitative study. Journal of Pediatric oncology Nursing. 2003; 20(6):301-13. [DOI:10.1177/1043454203254984] [PMID] [DOI:10.1177/1043454203254984]
27. Khanjari S, Seyedfatemi N, Borji S, Haghani H. [Effect of coping skills training on quality of life among parents of children with leukemia (Persian)]. Hayat. 2013; 19(4):15-25.
28. Wahnefried WD, Jones LW. Promoting a healthy lifestyle among cancer survivors. Hematology/Oncology Clinics of North America. 2008; 22(2):319-42. [DOI:10.1016/j.hoc.2008.01.012] [PMID] [PMCID] [DOI:10.1016/j.hoc.2008.01.012]
Send email to the article author
| Rights and permissions | |
 | This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Articles Copyright © The Author(s).
Owned by Guilan University of Medical Sciences.
Co-published by Negah Institute for Scientific Communication.
Contact Information
JHNM Office, Guilan University of Medical Sciences P.O.Box 41635-1873, Rasht, Iran
Journal Tel: +9813 33553202
Publisher Tel: +9821 453 55 555; +9821 453 55 000
Email: holisticnmj@gmail.com, nursjournal@gums.ac.ir
