Sat, May 4, 2024
Volume 29, Issue 1 (1-2019)
JHNM 2019, 29(1): 8-14 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Asadi K, Niknami M, Jafari Asl M, Kazemnezhad Leyli E. Relationship Between the Dimensions of Quality of Work Life and General Health in Iranian Nurses. JHNM 2019; 29 (1) :8-14
URL: http://hnmj.gums.ac.ir/article-1-547-en.html
URL: http://hnmj.gums.ac.ir/article-1-547-en.html



1- Nursing (MSN), School of Nursing and Midwifery, Guilan University of Medical Sciences, Rasht, Iran.
2- Instructor, Department of Midwifery, School of Nursing and Midwifery, Guilan University of Medical Sciences, Rasht, Iran.
3- Instructor, Department of Nursing, School of Nursing and Midwifery, Guilan University of Medical Sciences, Rasht, Iran.
4- Associate Professor, Social Determinants of Health Research Center (SDHRC), Bio-Statistics, Guilan University of Medical Sciences, Rasht, Iran.
2- Instructor, Department of Midwifery, School of Nursing and Midwifery, Guilan University of Medical Sciences, Rasht, Iran.
3- Instructor, Department of Nursing, School of Nursing and Midwifery, Guilan University of Medical Sciences, Rasht, Iran.
4- Associate Professor, Social Determinants of Health Research Center (SDHRC), Bio-Statistics, Guilan University of Medical Sciences, Rasht, Iran.
Full-Text [PDF 523 kb]
(1028 Downloads)
| Abstract (HTML) (3843 Views)
Considering the vital role of nurses as the main member of the healthcare team responsible for maintaining health in the family and society, attention to the problems of this group and helping them to overcome their problems seems to be necessary. Therefore, according to the research results, it is recommended that hospital managers pay more attention to the different dimensions of nurses’ QWL, especially the dimension of work life/home life, and use appropriate strategies such as providing child care services (like kindergarten in or near the hospital), transportation service, reducing working hours, avoiding compulsory overtime, hiring new forces, and increasing salaries and benefits to improve their general health. In this way, the quality of nursing care will indirectly improve and ultimately result in the satisfaction of the patients, their families, and the community.
Psychological states of nurses while completing the questionnaires and their accuracy and honesty in their responses were some limitations of this study which can affect the study results. In this regard, the researcher, as far as possible, attempted to overcome these limitations by the presence in the service area of the nurses and giving sufficient explanations about the research objectives.
Ethical Considerations
Compliance with ethical guidelines
This paper was approved by the Ethics Committee of Guilan University of Medical Sciences (code: 93121912).
Funding
This paper was extracted from a master thesis of khadijeh Asadi in Department medical-surjycal, Guilan University of Medical Sciences. This study was supported by Guilan University of Medical Sciences (GUMS).
Authors contributions
The authors contributions is as follows: Design, definition of intellectual context, Literature search, clinical studies, and Manuscript review: Khadijeh Asadi, Maryam Niknami and Masoumeh Jafari Asl; Experimental studies: Khadijeh Asadi and Maryam Niknami; Data acquisition: Khadijeh Asadi and Ehsan Kazemnezhad Leyli; Data analysis and Statistical analysis: Khadijeh Asadi, Maryam Niknami and Ehsan Kazemnezhad Leyli; Manuscript preparation and Manuscript editing: Khadijeh Asadi and Maryam Niknami; and Guarantor: All Authors.
Conflict of interest
The authors declare no conflict of interest.
Acknowledgements
The authors would like to thank the Research deputy of Guilan University of Medical Sciences (GUMS) for the financial support.
Reference
Full-Text: (1099 Views)
Introduction
Health is everyone’s right, a social goal, and a necessary condition for doing individual and social roles [1]. As defined by the World Health Organization (WHO), health is a “State of complete physical, mental, and social well-being, and not merely infirmity or the absence of disease”. In recent years, the ability to have a productive life, both economically and socially, has been added to this definition [2-4]. According to WHO definition, health is a multi-dimensional concept and its dimensions affect each other [5, 6].
One of the social aspects affecting the people’s health is occupation [7]. Occupation is an important part of every person’s life, because at least one third of everyone’s life is spent at work [8]. Health and treatment sector is one of the most important areas for sustainable health development that shoulder the critical responsibility of maintaining and restoring the health of the human community [9]. Nurses are the largest group in this sector, and providing effective health services is highly dependent on their health [10]. In Iran, 80% of health care workers are nurses [11].
Some jobs compared to others more threaten the employees’ health by exposing them to multiple and different physical, bodily, mental, and social stressors. Nursing is one of the most stressful jobs [12]. A national report in Canada revealed that nurses are the sickest workers in Canada [13]. The results of a study in Tehran, Iran showed that 7.4% of nurses take leave of absence each week due to burnout or disability, which is 80% more than other jobs [14]. Also, based on a study in Rasht City, 70.3% of nurses complained of some health problems [15]. Therefore, in order to respect the body, spirit and dignity of the workers, especially nurses in the workplace, some measures such as providing welfare facilities, medical care, job security, career development, education, improvements, etc. are required; all of which are considered as the Quality of Work Life (QWL) [16]. The QWL is the ability of employees to meet their personal needs by using the experiences gained in the organization [17]. Based on the perspectives of employees, QWL is the desirability or undesirability of the work environment [18].
QWL of nurses has four dimentiors: 1. Work life/home life dimension which is the interface between nurse’s work and home life and as most nurses are women, this dimension reflects the conflict between nurse’s roles as mother, daughter, and wife with their work environment; 2. Work schedule that describes nurses specific tasks and duties; 3. Work condition refers to the effect of workplace on nurses and patients; and 4. Work environment denotes the social work backgrounds based on social attitudes toward occupational status, and social feedback of job position in the form of job satisfaction [19]. Problems in each area can lead to job dissatisfaction and, consequently, physical and mental burnout and inclination to leave the job [20].
The health of nurses as care providers influences the quality of the services provided to their patients. Therefore, in order to provide proper care by nurses, they should be healthy people [21, 22]. Nurses, on the other hand, spend most of their time at work and in close contact with patients. Therefore, attention to the QWL and its dimensions as an important cause of health disorders can affect family and professional tasks and the quality of the function and care of patients, which reveals the need for this research.
There are limited studies on the relationship between the QWL of nurses and their general health. In the studies the relationship between these two variables were assessed in various occupational groups (sports referees, employees, faculty members and school principals), and their results showed a relationship between QWL and the health of workers [8, 23, 24]. However, there is much controversy over which QWL dimension is more effective on the health of individuals; a topic which calls for further research. In this regard, this study aimed to examine the relationship of QWL dimensions with general health of nurses working in Rasht educational and treatment centers.
Materials and Methods
This is an analytical cross-sectional study. The study population consisted of all nurses working in Rasht educational and treatment centers with at least an associate degree and six months of clinical work experience [12, 25]. Those who were in long-term sick or paid leave (more than one week), and technical nursing managers (supervisors and metrons) as well as those who were unwilling to participate in the study, were excluded from the research.
The required sample size based on the reported correlation coefficient between two variables of QWL and general health (r=0.263) in a similar study [26], 95% confidence level, and 90% test power, was estimated as 418. Stratified random sampling technique was used for recruiting samples. To do so, each of the 8 Rasht educational and treatment centers was considered as a class. The researcher took the number of all working nurses (n=1460) from the Province Nurse Head Office. Then, it was determined the number of nurses in each center by visiting that center. Next, by dividing the total number of nurses in each educational center by the total study population, multiplied by the total number of samples, the number of samples needed from each educational center was determined.
Afterwards, by using the community proportion and dividing the number of nurses in each department by the whole nurses of that center multiplied by the number of samples needed from each center, the number of samples required from each department was determined. Next, in each department, by dividing the number of nurses in that department by the number of samples needed from that department, the sampling interval was obtained. Finally, in each department, using random number table, a number was selected; and according to the sampling interval, the selected samples of each department was determined.
For collecting data, a demographic-occupational form, Brooks’ Quality of Nursing Work Life (QNWL) questionnaire, and Goldberg and Hillier’s General Health Questionnaire (GHQ) were used. The demographic-occupational form had 27 items. QNWL had 42 items which assessed four dimensions of QWL (work Life/home life, work design, work context, work environment) and is based on 6-Point Likert-Type Scale. Items 4, 10, 12, 13, and 40 have reversed scoring. Score 42 refers to the lowest quality of work life from the participant’s perspective and score 252 is the highest score. Finally, the QWL of a person is reported by combining the mean scores of three options of “completely disagree” to “disagree” as undesirable and combining three options of “agree” to “completely agree” as desirable. A mean value of less than 147 indicates undesirable QWL and the value more than 147 indicates desirable QWL [27, 28].
GHQ is a standard tool for screening individuals’ health state and signs such as abnormal thoughts, feelings, and aspects of the person’s behavior in the last month. Its reliability and validity have been examined by Nazifi et al. and they reported its reliability coefficient as 92% [29]. It has 28 four-choice questions with four subscales: somatic symptoms, anxiety/insomnia, social dysfunction, and severe depression. Its scoring is based on 4-point Likert scale (0= not at all, 1= no more than usual, 2= rather more than usual, 3= much more than usual). Items 15, and 17-20 have reversed scoring. The total score ranges between 0 and 84. The score 23 or less indicates good general health and scores higher than 23 shows poor general health.
To determine the validity of Brooks’ QNWL, its translated version with the original English questionnaire was sent to 10 faculty members of Nursing and Midwifery School. They were retranslated and revised the questionnaire. Then, the Content Validity Index (CVI) and Content Validity Ratio (CVR) of each question was measured in three areas of clarity, relevance and simplicity and scored from 0.8 to 1, indicating the high validity of questionnaire. To determine its reliability, the questionnaire was answered by 20 nurses working in educational and treatment centers of Rasht in two-week interval. The Cronbach alpha coefficient was used to determine the internal consistency of items, which was obtained as 85%. Test-retest execution also confirmed the reliability of the answers in more than 98% of items.
The nurses with at least associate degree and 6 months clinical experience were enrolled in the study. Data were collected gradually by referring to the educational centers in different working shifts (morning, evening and night) during the three months of April, May, and June of 2015. Finally, of 418 distributed questionnaires, 404 were returned from study centers. After collecting data, they were presented using descriptive statistics (mean, standard deviation, percentage). Non-parametric test of Spearman correlation coefficient as well as Chi-Squared Test and multiple logistic regression analysis were used to analyze the obtained data. The significant level was set at 0.05 (P<0.05).
Results
Based on the results, most nurses were female (96.3%) and married (74.3%). About 58.2% of them were under 35 years old with a Mean±SD age of 34.72±8 years. Monthly salary of the most nurses (61.6%) was less than $500, and majority of them (51.2%) had overtime work less than 50 hours per month. Most of them (72.8%) had rotational shift and a working background of less than 10 years (54.5%).
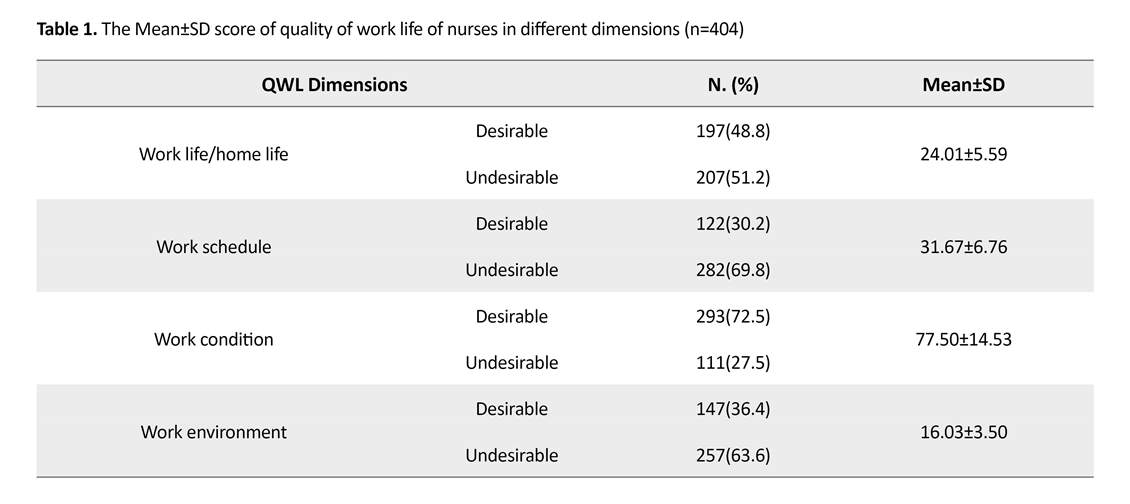
Their Mean±SD total score of QNWL was 149.21±23.92. The highest Mean score belonged to the dimension of work condition (77.50±14.53) and the lowest Mean was related to work environment (16.03±3.50). The general QWL for the majority of nurses (55.4%) was desirable, but undesirable for the remaining (44.4%). Among these, the most favorable state was related to the dimension of work condition (72.5%) and the lowest favorable was related to the work schedule (69.8%) (Table 1).
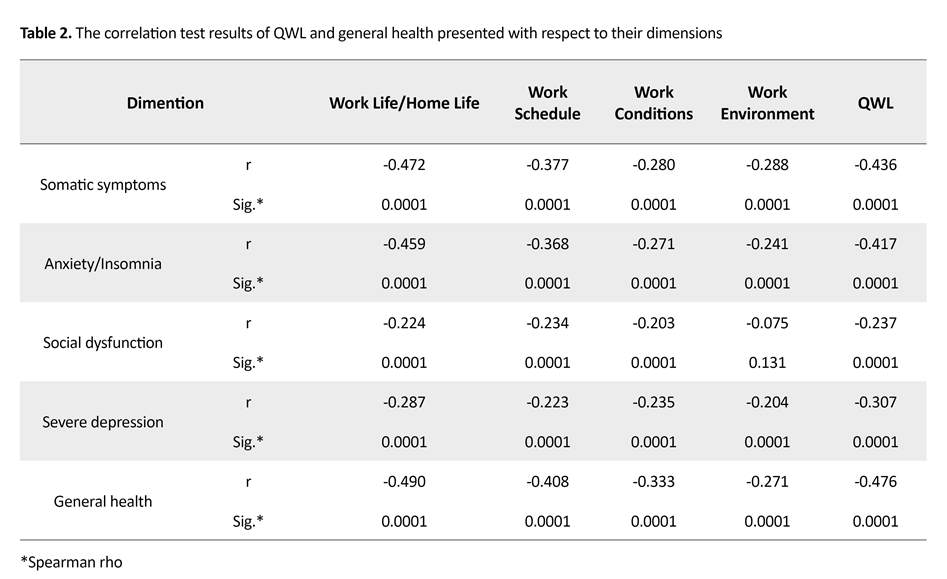
Their Mean±SD total score of GHQ was 28.03±11.53. Regarding the general health status, 157 (38.9%) nurses were healthy and 247 (61.1%) were suspected of having health disorders. The Spearman test results indicated a significant and negative relationship between QWL dimensions and the total score of QWL with each dimension of general health as well as total score of general health (P<0.001). Accordingly, the highest correlation was found between the dimensions of “work life/home life” (P=0.0001, r=-0.490) and then “work schedule” (P=0.0001, r=-0.408) with general health total score (Table 2).
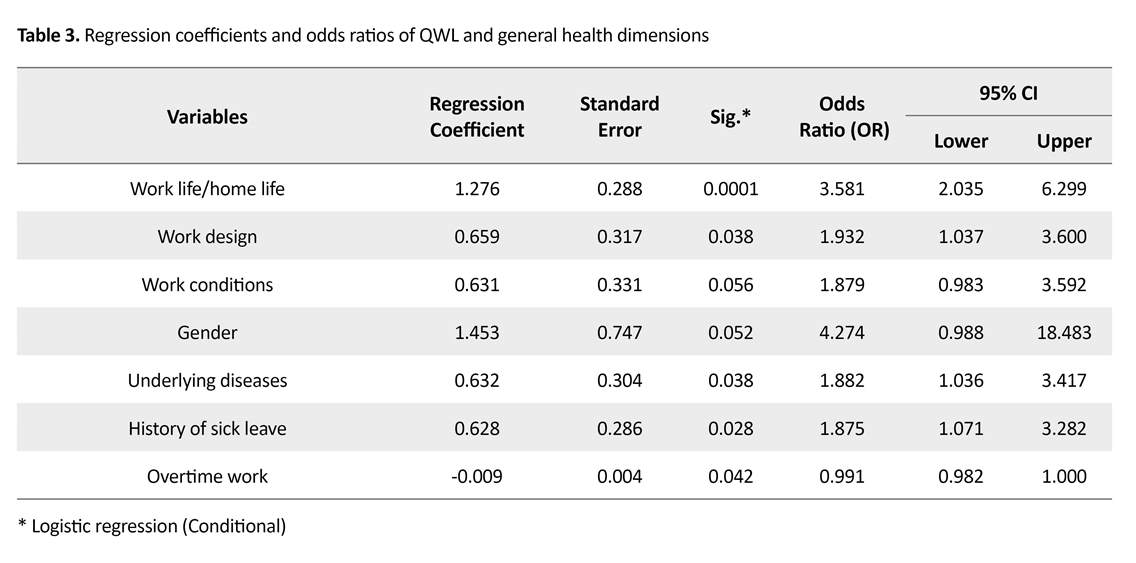
Multiple logistic regression analysis results showed that, after controlling the effects of seismographic variables and underlying diseases, dimensions of work life/home life (OR=3.581, P<001), work schedule (OR=1.932, P=0.038), and work conditions (OR=1.879, P=0.05) were, in the descending order, the predictors of general health in nurses. Nurses who have a desirable QWL based on these three dimensions are more likely to have general good health. Results also indicated that gender (OR=4.274, P=0.05), underlying diseases (OR=1.882, P=0.038), history of sick leave (OR=1.875, P=0.028), and overtime work hours (OR=0.991, P=0.042) were other predictors of nurses’ general health (Table 3).
Discussion
Based on the study results, the mean total score of QWL of nurses is higher than that what were reported in similar studies [28, 30, 31]. Differences in the results can be due to differences in by individuals’ expectations and perceptions of QWL, because the QWL is related to the individual’s mental and emotional perceptions of workplace [23]. In this study, the highest mean score of QWL dimensions was related to the work conditions and the lowest mean score related to the work environment that is in agreement with some studies [28, 30].
Overall QWL in the majority of nurses was reported as desirable, while in the study of Navidian [31], half of the nurses had moderate QWL, and in Opollo [32] study, the majority of them reported poor QWL. In the study of Khani [33], the most undesirable situation was related to the work conditions, while in Almalki study [28], the most undesirable state was work life/home life. These differences in the findings may be due to the differences in the time and settings of the studies as well as cultural, economic and social differences of the respondents; because studies have shown that temporal, social and cultural conditions affect the motivation, performance and satisfaction of employees, and cultural preferences in a particular culture have a major impact on the attitude of organization members towards the QWL.
The study results indicated that the mean general health of nurses was lower than that reported in Maghsoudi study [15], and higher than what reported in Hojjati study [11]. The majority of nurses in our study were suspected of having a health disorder whose rate was greater than that of reported by Noorian et al. [34]. It seems that differences in the time and place of study, lifestyle, and economic, social and cultural status of the study samples can be reasons of this inconsistency in results. The nurses’ health, for many reasons, is at a higher risk than other people in the community.
Health is everyone’s right, a social goal, and a necessary condition for doing individual and social roles [1]. As defined by the World Health Organization (WHO), health is a “State of complete physical, mental, and social well-being, and not merely infirmity or the absence of disease”. In recent years, the ability to have a productive life, both economically and socially, has been added to this definition [2-4]. According to WHO definition, health is a multi-dimensional concept and its dimensions affect each other [5, 6].
One of the social aspects affecting the people’s health is occupation [7]. Occupation is an important part of every person’s life, because at least one third of everyone’s life is spent at work [8]. Health and treatment sector is one of the most important areas for sustainable health development that shoulder the critical responsibility of maintaining and restoring the health of the human community [9]. Nurses are the largest group in this sector, and providing effective health services is highly dependent on their health [10]. In Iran, 80% of health care workers are nurses [11].
Some jobs compared to others more threaten the employees’ health by exposing them to multiple and different physical, bodily, mental, and social stressors. Nursing is one of the most stressful jobs [12]. A national report in Canada revealed that nurses are the sickest workers in Canada [13]. The results of a study in Tehran, Iran showed that 7.4% of nurses take leave of absence each week due to burnout or disability, which is 80% more than other jobs [14]. Also, based on a study in Rasht City, 70.3% of nurses complained of some health problems [15]. Therefore, in order to respect the body, spirit and dignity of the workers, especially nurses in the workplace, some measures such as providing welfare facilities, medical care, job security, career development, education, improvements, etc. are required; all of which are considered as the Quality of Work Life (QWL) [16]. The QWL is the ability of employees to meet their personal needs by using the experiences gained in the organization [17]. Based on the perspectives of employees, QWL is the desirability or undesirability of the work environment [18].
QWL of nurses has four dimentiors: 1. Work life/home life dimension which is the interface between nurse’s work and home life and as most nurses are women, this dimension reflects the conflict between nurse’s roles as mother, daughter, and wife with their work environment; 2. Work schedule that describes nurses specific tasks and duties; 3. Work condition refers to the effect of workplace on nurses and patients; and 4. Work environment denotes the social work backgrounds based on social attitudes toward occupational status, and social feedback of job position in the form of job satisfaction [19]. Problems in each area can lead to job dissatisfaction and, consequently, physical and mental burnout and inclination to leave the job [20].
The health of nurses as care providers influences the quality of the services provided to their patients. Therefore, in order to provide proper care by nurses, they should be healthy people [21, 22]. Nurses, on the other hand, spend most of their time at work and in close contact with patients. Therefore, attention to the QWL and its dimensions as an important cause of health disorders can affect family and professional tasks and the quality of the function and care of patients, which reveals the need for this research.
There are limited studies on the relationship between the QWL of nurses and their general health. In the studies the relationship between these two variables were assessed in various occupational groups (sports referees, employees, faculty members and school principals), and their results showed a relationship between QWL and the health of workers [8, 23, 24]. However, there is much controversy over which QWL dimension is more effective on the health of individuals; a topic which calls for further research. In this regard, this study aimed to examine the relationship of QWL dimensions with general health of nurses working in Rasht educational and treatment centers.
Materials and Methods
This is an analytical cross-sectional study. The study population consisted of all nurses working in Rasht educational and treatment centers with at least an associate degree and six months of clinical work experience [12, 25]. Those who were in long-term sick or paid leave (more than one week), and technical nursing managers (supervisors and metrons) as well as those who were unwilling to participate in the study, were excluded from the research.
The required sample size based on the reported correlation coefficient between two variables of QWL and general health (r=0.263) in a similar study [26], 95% confidence level, and 90% test power, was estimated as 418. Stratified random sampling technique was used for recruiting samples. To do so, each of the 8 Rasht educational and treatment centers was considered as a class. The researcher took the number of all working nurses (n=1460) from the Province Nurse Head Office. Then, it was determined the number of nurses in each center by visiting that center. Next, by dividing the total number of nurses in each educational center by the total study population, multiplied by the total number of samples, the number of samples needed from each educational center was determined.
Afterwards, by using the community proportion and dividing the number of nurses in each department by the whole nurses of that center multiplied by the number of samples needed from each center, the number of samples required from each department was determined. Next, in each department, by dividing the number of nurses in that department by the number of samples needed from that department, the sampling interval was obtained. Finally, in each department, using random number table, a number was selected; and according to the sampling interval, the selected samples of each department was determined.
For collecting data, a demographic-occupational form, Brooks’ Quality of Nursing Work Life (QNWL) questionnaire, and Goldberg and Hillier’s General Health Questionnaire (GHQ) were used. The demographic-occupational form had 27 items. QNWL had 42 items which assessed four dimensions of QWL (work Life/home life, work design, work context, work environment) and is based on 6-Point Likert-Type Scale. Items 4, 10, 12, 13, and 40 have reversed scoring. Score 42 refers to the lowest quality of work life from the participant’s perspective and score 252 is the highest score. Finally, the QWL of a person is reported by combining the mean scores of three options of “completely disagree” to “disagree” as undesirable and combining three options of “agree” to “completely agree” as desirable. A mean value of less than 147 indicates undesirable QWL and the value more than 147 indicates desirable QWL [27, 28].
GHQ is a standard tool for screening individuals’ health state and signs such as abnormal thoughts, feelings, and aspects of the person’s behavior in the last month. Its reliability and validity have been examined by Nazifi et al. and they reported its reliability coefficient as 92% [29]. It has 28 four-choice questions with four subscales: somatic symptoms, anxiety/insomnia, social dysfunction, and severe depression. Its scoring is based on 4-point Likert scale (0= not at all, 1= no more than usual, 2= rather more than usual, 3= much more than usual). Items 15, and 17-20 have reversed scoring. The total score ranges between 0 and 84. The score 23 or less indicates good general health and scores higher than 23 shows poor general health.
To determine the validity of Brooks’ QNWL, its translated version with the original English questionnaire was sent to 10 faculty members of Nursing and Midwifery School. They were retranslated and revised the questionnaire. Then, the Content Validity Index (CVI) and Content Validity Ratio (CVR) of each question was measured in three areas of clarity, relevance and simplicity and scored from 0.8 to 1, indicating the high validity of questionnaire. To determine its reliability, the questionnaire was answered by 20 nurses working in educational and treatment centers of Rasht in two-week interval. The Cronbach alpha coefficient was used to determine the internal consistency of items, which was obtained as 85%. Test-retest execution also confirmed the reliability of the answers in more than 98% of items.
The nurses with at least associate degree and 6 months clinical experience were enrolled in the study. Data were collected gradually by referring to the educational centers in different working shifts (morning, evening and night) during the three months of April, May, and June of 2015. Finally, of 418 distributed questionnaires, 404 were returned from study centers. After collecting data, they were presented using descriptive statistics (mean, standard deviation, percentage). Non-parametric test of Spearman correlation coefficient as well as Chi-Squared Test and multiple logistic regression analysis were used to analyze the obtained data. The significant level was set at 0.05 (P<0.05).
Results
Based on the results, most nurses were female (96.3%) and married (74.3%). About 58.2% of them were under 35 years old with a Mean±SD age of 34.72±8 years. Monthly salary of the most nurses (61.6%) was less than $500, and majority of them (51.2%) had overtime work less than 50 hours per month. Most of them (72.8%) had rotational shift and a working background of less than 10 years (54.5%).
Their Mean±SD total score of QNWL was 149.21±23.92. The highest Mean score belonged to the dimension of work condition (77.50±14.53) and the lowest Mean was related to work environment (16.03±3.50). The general QWL for the majority of nurses (55.4%) was desirable, but undesirable for the remaining (44.4%). Among these, the most favorable state was related to the dimension of work condition (72.5%) and the lowest favorable was related to the work schedule (69.8%) (Table 1).
Their Mean±SD total score of GHQ was 28.03±11.53. Regarding the general health status, 157 (38.9%) nurses were healthy and 247 (61.1%) were suspected of having health disorders. The Spearman test results indicated a significant and negative relationship between QWL dimensions and the total score of QWL with each dimension of general health as well as total score of general health (P<0.001). Accordingly, the highest correlation was found between the dimensions of “work life/home life” (P=0.0001, r=-0.490) and then “work schedule” (P=0.0001, r=-0.408) with general health total score (Table 2).
Multiple logistic regression analysis results showed that, after controlling the effects of seismographic variables and underlying diseases, dimensions of work life/home life (OR=3.581, P<001), work schedule (OR=1.932, P=0.038), and work conditions (OR=1.879, P=0.05) were, in the descending order, the predictors of general health in nurses. Nurses who have a desirable QWL based on these three dimensions are more likely to have general good health. Results also indicated that gender (OR=4.274, P=0.05), underlying diseases (OR=1.882, P=0.038), history of sick leave (OR=1.875, P=0.028), and overtime work hours (OR=0.991, P=0.042) were other predictors of nurses’ general health (Table 3).
Discussion
Based on the study results, the mean total score of QWL of nurses is higher than that what were reported in similar studies [28, 30, 31]. Differences in the results can be due to differences in by individuals’ expectations and perceptions of QWL, because the QWL is related to the individual’s mental and emotional perceptions of workplace [23]. In this study, the highest mean score of QWL dimensions was related to the work conditions and the lowest mean score related to the work environment that is in agreement with some studies [28, 30].
Overall QWL in the majority of nurses was reported as desirable, while in the study of Navidian [31], half of the nurses had moderate QWL, and in Opollo [32] study, the majority of them reported poor QWL. In the study of Khani [33], the most undesirable situation was related to the work conditions, while in Almalki study [28], the most undesirable state was work life/home life. These differences in the findings may be due to the differences in the time and settings of the studies as well as cultural, economic and social differences of the respondents; because studies have shown that temporal, social and cultural conditions affect the motivation, performance and satisfaction of employees, and cultural preferences in a particular culture have a major impact on the attitude of organization members towards the QWL.
The study results indicated that the mean general health of nurses was lower than that reported in Maghsoudi study [15], and higher than what reported in Hojjati study [11]. The majority of nurses in our study were suspected of having a health disorder whose rate was greater than that of reported by Noorian et al. [34]. It seems that differences in the time and place of study, lifestyle, and economic, social and cultural status of the study samples can be reasons of this inconsistency in results. The nurses’ health, for many reasons, is at a higher risk than other people in the community.
The most important reasons for this condition may be the stressful nature of this profession, variable work shifts, poor flexibility in the work schedule, long working hours and the impossibility of changing the work time. On the other hand, the majority of staff in this profession are women who, besides their working duties, are responsible for parenting and household tasks. This can increase the level of anxiety and stress in this group and put their health at risk [12, 15, 35, 36].
The results of our study also indicate a significant and negative relationship between QWL dimensions and total score of QWL with each subscales of general health as well as total score of general health. This results are consistent with the findings of some studies [24, 25, 37], while disagree with some others [14, 23]. Based on the researcher’ opinion, whole is something more than its parts and parts are not always suggestive of the whole. The difference in the findings can be due to this reason.
In this study, dimensions of work life/home life, work schedule, and work conditions were found to be the predictors of general health in nurses. This finding reflects the fact that work and family can interact with each other, and strengthen the physical and emotional health of employees. The results of Mostafavi Rad indicate that balance between work life and home life, work commitment, job security, human relationships in the workplace, and financial and welfare issues are among the predictors of mental health [38]. The researcher believes that in different times and places, the impact of some factors on health may be more and act as predictors. Therefore, health predictors are not constant and may vary depending on the time and place and in different individuals.
The results of our study also indicate a significant and negative relationship between QWL dimensions and total score of QWL with each subscales of general health as well as total score of general health. This results are consistent with the findings of some studies [24, 25, 37], while disagree with some others [14, 23]. Based on the researcher’ opinion, whole is something more than its parts and parts are not always suggestive of the whole. The difference in the findings can be due to this reason.
In this study, dimensions of work life/home life, work schedule, and work conditions were found to be the predictors of general health in nurses. This finding reflects the fact that work and family can interact with each other, and strengthen the physical and emotional health of employees. The results of Mostafavi Rad indicate that balance between work life and home life, work commitment, job security, human relationships in the workplace, and financial and welfare issues are among the predictors of mental health [38]. The researcher believes that in different times and places, the impact of some factors on health may be more and act as predictors. Therefore, health predictors are not constant and may vary depending on the time and place and in different individuals.
Considering the vital role of nurses as the main member of the healthcare team responsible for maintaining health in the family and society, attention to the problems of this group and helping them to overcome their problems seems to be necessary. Therefore, according to the research results, it is recommended that hospital managers pay more attention to the different dimensions of nurses’ QWL, especially the dimension of work life/home life, and use appropriate strategies such as providing child care services (like kindergarten in or near the hospital), transportation service, reducing working hours, avoiding compulsory overtime, hiring new forces, and increasing salaries and benefits to improve their general health. In this way, the quality of nursing care will indirectly improve and ultimately result in the satisfaction of the patients, their families, and the community.
Psychological states of nurses while completing the questionnaires and their accuracy and honesty in their responses were some limitations of this study which can affect the study results. In this regard, the researcher, as far as possible, attempted to overcome these limitations by the presence in the service area of the nurses and giving sufficient explanations about the research objectives.
Ethical Considerations
Compliance with ethical guidelines
This paper was approved by the Ethics Committee of Guilan University of Medical Sciences (code: 93121912).
Funding
This paper was extracted from a master thesis of khadijeh Asadi in Department medical-surjycal, Guilan University of Medical Sciences. This study was supported by Guilan University of Medical Sciences (GUMS).
Authors contributions
The authors contributions is as follows: Design, definition of intellectual context, Literature search, clinical studies, and Manuscript review: Khadijeh Asadi, Maryam Niknami and Masoumeh Jafari Asl; Experimental studies: Khadijeh Asadi and Maryam Niknami; Data acquisition: Khadijeh Asadi and Ehsan Kazemnezhad Leyli; Data analysis and Statistical analysis: Khadijeh Asadi, Maryam Niknami and Ehsan Kazemnezhad Leyli; Manuscript preparation and Manuscript editing: Khadijeh Asadi and Maryam Niknami; and Guarantor: All Authors.
Conflict of interest
The authors declare no conflict of interest.
Acknowledgements
The authors would like to thank the Research deputy of Guilan University of Medical Sciences (GUMS) for the financial support.
Reference
- Hesabi M. [The relationship between general health and mutual work-family conflict in medical education hospital nurses in rasht (Persian)] [MSc. thesis]. Rasht: Guilan University of Medical Science; 2011.
- Allender J, Rector C, Rector C, Warner K. Community & public health nursing: Promoting the public's health. Philadelphia: Lippincott Williams & Wilkins; 2013.
- Sadeghi Hassan Abadi A. [Generalities of public health (Persian)]. Tehran: Gap Publications; 2010.
- Ayldrabady I. [Textbook of community health nursing 1, 2, 3 (Persian)]. Tehran: Jame'e Negar; 2012.
- Kamali Dehkordi F. [Assesment of job satisfactions dimentions and its relationship with general health of health employe in rashtcity. Guilan University of Medical Sciences and Health Service (Persian)] [Master thesis]. Rasht: Guilan University of Medical Sciences; 2013.
- Hosseini V, Jafary Varjoshani N. [Lancaster community health nursing (Persian)]. Tehran: Jame'e Negar; 2013.
- Haddadi M, Kaldi A, Sajadi H, Salehi M. [Relationship between job classification and mental health in employed women (Persian)]. Social Welfare Quarterly. 2011; 11(40):107-27.
- Nazari S, Tojari F, Esmaeili MR. The relationship between mental health with job stress, quality of work life, and self-efficacy among referees. International Journal of Sport Studies. 2014; 4(5):531-9.
- Heidari F, Mohammad-Khan Kermanshahi S. [Barriers to health-promoting behaviors in nurses (Persian)]. Journal of Health and Care. 2012; 4(14):9-18.
- Fronteira I, Ferrinho P. Do nurses have a different physical health profile? A systematic review of experimental and observational studies on nurses’ physical health. Journal of Clinical Nursing. 2011; 20(17-18):2404-24. [DOI:10.1111/j.1365-2702.2011.03721.x] [PMID]
- Hojjati H, Jalalmanesh Sh, Fesharaki M. [Sleeplessness effect on the general health of hospitals nightshift nurses in Gorgan, Iran (Persian)]. Journal of Gorgan University of Medical Sciences. 2009; 11(3):70-5.
- Darvishpoor Kakhki A, Ebrahimi H, Alavi Majd H. [Health status of nurses of hospitals dependent to Shahroud Medical University (Persian)]. Iran Journal of Nursing .2009; 22(60):19-27.
- Horrigan JM, Lightfoot NE, Larivière MA, Jacklin K. Evaluating and improving nurses' health and quality of work life: A cross-sectional study of Korean blue collar workers employed by small businesses. Workplace Health & Safety. 2013; 61(4):173-81. [DOI:10.1177/216507991306100405] [PMID]
- Mohamadi A, Sarhangi F, Ebadi A, Daneshmandi M, Reiisifar A, Amiri F, et al. [Relationship between psychological problems and quality of work life of intensive care units nurses (Persian)]. Iranian Journal of Critical Care Nursing. 2011; 3(4):135-40.
- Maghsoudi Sh, Hesabi M, EmamiSigaroudi A, Kazemnejad Leili E, Monfared A. [General health and related factors in employed nurses in Medical-Educational Centers in Rasht (Persian)]. Holistic Nursing and Midwifery. 2015; 75(25):63-72.
- Godarzvand Chegini M, Haghghi M. [Compare the quality of work life and personal characteristics among Gilan University and Islamic Azad University of Rasht Branch (Persian)]. Journal of Iranian Higher Education. 2010; 3(2):139-57.
- Koushki MS, Akbari Sari A, Arab M, Ahmadi Engali K. [Quality of working life and its relation with productivity of nurses' performance in Shahid Beheshti University of Medical Sciences hospitals (Persian)]. Journal of the School of Public Health and Institute of Public Health Research. 2013; 10(4):81-90.
- Naeimi G, Nazari AM, Sanai ZB. [A study of relationship between qulaity of work life and work-family conflict with job performance among married men employee (Persian)]. Quarterly Journal of Career & Organizational Counseling. 2012; 10(4):57-72.
- Azarrang Sh, Yaghmaei F, Shiri M. [Correlation dimensions of quality of work life of nurses and demographic characteristics (Persian)]. Nursing Research. 2012; 7(27):18-24.
- Dargahi H, Gharib M, Goudarzi M. [Quality of work life in nursing employees of Tehran University of Medical Sciences hospitals (Persian)]. Hayat. 2007; 13(2):13-21.
- Soleymani MA, Masoodi R, Sadeghi T, Bahrami N, Ghorbani M, Hassanpour Dehkordi A. [General health and its relationship with sleep quality of full-time and part-time nurses working in Educational Centers affiliated to Iran University of Medical Sciences (Persian)]. Journal of Shahrkord University of Medical Sciences. 2008; 10(3):70-5.
- Hamid N, Dehghanizadeh Z. [The relationship between spirituality, organizational commitment and general health with job performance of clinical nurses (Persian)]. Journal of Nursing Management. 2012; 1(2):20-8.
- Kamrani Z. [Relationship between quality of work Life and mental health in Esfahan Iron and Steel workers (Persian)]. Paper presented at: The 1st Congress of Pathology of organizational learning. 25-26 February 2012; Tehran, Iran.
- Farahbakhsh S, Sattar A. [The role of quality of work life in mental health of school principals (Persian)]. Journal of Fundamentals of Mental Health. 2012; 14(55):200-9. [DOI:10.22038/JFMH.2012.937]
- As'adi SN, Behdani F, Seyyed Nouzadi M, Farhadi M. [Effect of work place parameters on mental health of physicians and nurses of emergency and non-emergency wards (Persian)]. Journal of Fundamentals of Mental Health. 2010; 12(47):612-19.
- Mostahfezian M, Mozafari SAA, Amirtash AM. [Comparison study of general health, quality of work life of active and inactive faculty members at different Azad Universities in area 4 (Persian)]. Research on Sport Sciences. 2009; 6(4):113-46.
- Brooks BA, Anderson MA. Defining quality of nursing work life. Nursing Economics. 2005; 23(6):319-26. [PMID]
- Almalki MJ, FitzGerald G, Clark M. Quality of work life among primary health care nurses in the Jazan region, Saudi Arabia: A cross-sectional study. Human Resources for Health. 2012; 10(1):30. [DOI:10.1186/1478-4491-10-30] [PMID] [PMCID]
- Nazifi M, Mokarami H, Akbaritabar A, Faraji Kujerdi M, Tabrizi R, Rahi A. [Reliability, validity and factor structure of the Persian translation of General Health Questionnire (GHQ) in hospitals of Kerman University of Medical Sciences (Persian)]. Journal of Fasa University of Medical Sciences. 2014; 3(4):336-42.
- Saber S, Borhani F, Navidian A, Ramezani T, Rezvani Amin M, Kianian T. [Related quality of work life and productivity of hospitals in Kerman University of Medical Sciences (Persian)]. Bioethics Journal. 2013; 3(9):143-166.
- Navidian A, Saber S, RezvaniAmin M, Kianian T. Correlation of quality of work life and job satisfaction in nurses of Kerman University of Medical Sciences (Persian)]. Health Promotion Management. 2014; 2(3):7-15.
- Opollo J, Gray J, Spies L. Work‐related quality of life of Ugandan healthcare workers. International Nursing Review. 2014; 61(1):116-23. [DOI:10.1111/inr.12077] [PMID]
- Khani A, Jaafarpour M, Dyrekvandmogadam A. Quality of nursing work life. Journal of Clinical and Diagnostic Research. 2008; 2(6):1169-74.
- Noorian C, Parvin N , Mehrabi T. [Evaluation of the relationship between occupational stress and general health condition in nurses working in Isfahan university hospitals 2005 (Persian)]. Journal of Community Health. 2005; 5(1):45-52.
- Parvizi S, Naseri F, Seyed Fatemi N, Ghasem Zadeh kakroudi F. [Social factors contributing in women health in Tehran city: A qualitative study (Persian)]. Iranian Journal of Nursing Research. 2010; 4(15):6-15.
- Musarezaie A, Bagherian-Sararoudi R, Fanian N, Tabatabaie SM. [Predictors of nurses’ mental health in medical and surgical wards based on demographic variables (Persian)]. Journal of Research in Behavioural Sciences. 2014; 12(3):369-79.
- Rasti S, Niazmand H, Heydari HR. [Survey the relationship between quality of work life and mental health in Bushehr prison staff; Case study: Dashtestan Prison Staff (Persian)]. Correction and Upbringing. 2011; 142:48-52.
- Mostafavi Rad F, Tabe Bordbar F, Zahedi S. [Prediction of mental health through considering organizational justice and quality of work life (Persian)]. Journal of Analytical-Cognitive Psychology. 2011; 2(6):75-87.
Article Type : Research |
Subject:
Special
Received: 2018/05/22 | Accepted: 2018/10/8 | Published: 2019/01/1
Received: 2018/05/22 | Accepted: 2018/10/8 | Published: 2019/01/1
References
1. Hesabi M. [The relationship between general health and mutual work-family conflict in medical education hospital nurses in rasht (Persian)] [MSc. thesis]. Rasht: Guilan University of Medical Science; 2011.
2. Allender J, Rector C, Rector C, Warner K. Community & public health nursing: Promoting the public's health. Philadelphia: Lippincott Williams & Wilkins; 2013.
3. Sadeghi Hassan Abadi A. [Generalities of public health (Persian)]. Tehran: Gap Publications; 2010.
4. Ayldrabady I. [Textbook of community health nursing 1, 2, 3 (Persian)]. Tehran: Jame'e Negar; 2012.
5. Kamali Dehkordi F. [Assesment of job satisfactions dimentions and its relationship with general health of health employe in rashtcity. Guilan University of Medical Sciences and Health Service (Persian)] [Master thesis]. Rasht: Guilan University of Medical Sciences; 2013.
6. Hosseini V, Jafary Varjoshani N. [Lancaster community health nursing (Persian)]. Tehran: Jame'e Negar; 2013.
7. Haddadi M, Kaldi A, Sajadi H, Salehi M. [Relationship between job classification and mental health in employed women (Persian)]. Social Welfare Quarterly. 2011; 11(40):107-27.
8. Nazari S, Tojari F, Esmaeili MR. The relationship between mental health with job stress, quality of work life, and self-efficacy among referees. International Journal of Sport Studies. 2014; 4(5):531-9.
9. Heidari F, Mohammad-Khan Kermanshahi S. [Barriers to health-promoting behaviors in nurses (Persian)]. Journal of Health and Care. 2012; 4(14):9-18.
10. Fronteira I, Ferrinho P. Do nurses have a different physical health profile? A systematic review of experimental and observational studies on nurses' physical health. Journal of Clinical Nursing. 2011; 20(17-18):2404-24. [DOI:10.1111/j.1365-2702.2011.03721.x] [PMID] [DOI:10.1111/j.1365-2702.2011.03721.x]
11. Hojjati H, Jalalmanesh Sh, Fesharaki M. [Sleeplessness effect on the general health of hospitals nightshift nurses in Gorgan, Iran (Persian)]. Journal of Gorgan University of Medical Sciences. 2009; 11(3):70-5.
12. Darvishpoor Kakhki A, Ebrahimi H, Alavi Majd H. [Health status of nurses of hospitals dependent to Shahroud Medical University (Persian)]. Iran Journal of Nursing .2009; 22(60):19-27.
13. Horrigan JM, Lightfoot NE, Larivière MA, Jacklin K. Evaluating and improving nurses' health and quality of work life: A cross-sectional study of Korean blue collar workers employed by small businesses. Workplace Health & Safety. 2013; 61(4):173-81. [DOI:10.1177/216507991306100405] [PMID] [DOI:10.1177/216507991306100405]
14. Mohamadi A, Sarhangi F, Ebadi A, Daneshmandi M, Reiisifar A, Amiri F, et al. [Relationship between psychological problems and quality of work life of intensive care units nurses (Persian)]. Iranian Journal of Critical Care Nursing. 2011; 3(4):135-40.
15. Maghsoudi Sh, Hesabi M, EmamiSigaroudi A, Kazemnejad Leili E, Monfared A. [General health and related factors in employed nurses in Medical-Educational Centers in Rasht (Persian)]. Holistic Nursing and Midwifery. 2015; 75(25):63-72.
16. Godarzvand Chegini M, Haghghi M. [Compare the quality of work life and personal characteristics among Gilan University and Islamic Azad University of Rasht Branch (Persian)]. Journal of Iranian Higher Education. 2010; 3(2):139-57.
17. Koushki MS, Akbari Sari A, Arab M, Ahmadi Engali K. [Quality of working life and its relation with productivity of nurses' performance in Shahid Beheshti University of Medical Sciences hospitals (Persian)]. Journal of the School of Public Health and Institute of Public Health Research. 2013; 10(4):81-90.
18. Naeimi G, Nazari AM, Sanai ZB. [A study of relationship between qulaity of work life and work-family conflict with job performance among married men employee (Persian)]. Quarterly Journal of Career & Organizational Counseling. 2012; 10(4):57-72.
19. Azarrang Sh, Yaghmaei F, Shiri M. [Correlation dimensions of quality of work life of nurses and demographic characteristics (Persian)]. Nursing Research. 2012; 7(27):18-24.
20. Dargahi H, Gharib M, Goudarzi M. [Quality of work life in nursing employees of Tehran University of Medical Sciences hospitals (Persian)]. Hayat. 2007; 13(2):13-21.
21. Soleymani MA, Masoodi R, Sadeghi T, Bahrami N, Ghorbani M, Hassanpour Dehkordi A. [General health and its relationship with sleep quality of full-time and part-time nurses working in Educational Centers affiliated to Iran University of Medical Sciences (Persian)]. Journal of Shahrkord University of Medical Sciences. 2008; 10(3):70-5.
22. Hamid N, Dehghanizadeh Z. [The relationship between spirituality, organizational commitment and general health with job performance of clinical nurses (Persian)]. Journal of Nursing Management. 2012; 1(2):20-8.
23. Kamrani Z. [Relationship between quality of work Life and mental health in Esfahan Iron and Steel workers (Persian)]. Paper presented at: The 1st Congress of Pathology of organizational learning. 25-26 February 2012; Tehran, Iran.
24. Farahbakhsh S, Sattar A. [The role of quality of work life in mental health of school principals (Persian)]. Journal of Fundamentals of Mental Health. 2012; 14(55):200-9. [DOI:10.22038/JFMH.2012.937]
25. As'adi SN, Behdani F, Seyyed Nouzadi M, Farhadi M. [Effect of work place parameters on mental health of physicians and nurses of emergency and non-emergency wards (Persian)]. Journal of Fundamentals of Mental Health. 2010; 12(47):612-19.
26. Mostahfezian M, Mozafari SAA, Amirtash AM. [Comparison study of general health, quality of work life of active and inactive faculty members at different Azad Universities in area 4 (Persian)]. Research on Sport Sciences. 2009; 6(4):113-46.
27. Brooks BA, Anderson MA. Defining quality of nursing work life. Nursing Economics. 2005; 23(6):319-26. [PMID] [PMID]
28. Almalki MJ, FitzGerald G, Clark M. Quality of work life among primary health care nurses in the Jazan region, Saudi Arabia: A cross-sectional study. Human Resources for Health. 2012; 10(1):30. [DOI:10.1186/1478-4491-10-30] [PMID] [PMCID] [DOI:10.1186/1478-4491-10-30]
29. Nazifi M, Mokarami H, Akbaritabar A, Faraji Kujerdi M, Tabrizi R, Rahi A. [Reliability, validity and factor structure of the Persian translation of General Health Questionnire (GHQ) in hospitals of Kerman University of Medical Sciences (Persian)]. Journal of Fasa University of Medical Sciences. 2014; 3(4):336-42.
30. Saber S, Borhani F, Navidian A, Ramezani T, Rezvani Amin M, Kianian T. [Related quality of work life and productivity of hospitals in Kerman University of Medical Sciences (Persian)]. Bioethics Journal. 2013; 3(9):143-166.
31. Navidian A, Saber S, RezvaniAmin M, Kianian T. Correlation of quality of work life and job satisfaction in nurses of Kerman University of Medical Sciences (Persian)]. Health Promotion Management. 2014; 2(3):7-15.
32. Opollo J, Gray J, Spies L. Work‐related quality of life of Ugandan healthcare workers. International Nursing Review. 2014; 61(1):116-23. [DOI:10.1111/inr.12077] [PMID] [DOI:10.1111/inr.12077]
33. Khani A, Jaafarpour M, Dyrekvandmogadam A. Quality of nursing work life. Journal of Clinical and Diagnostic Research. 2008; 2(6):1169-74.
34. Noorian C, Parvin N, Mehrabi T. [Evaluation of the relationship between occupational stress and general health condition in nurses working in Isfahan university hospitals 2005 (Persian)]. Journal of Community Health. 2005; 5(1):45-52.
35. Parvizi S, Naseri F, Seyed Fatemi N, Ghasem Zadeh kakroudi F. [Social factors contributing in women health in Tehran city: A qualitative study (Persian)]. Iranian Journal of Nursing Research. 2010; 4(15):6-15.
36. Musarezaie A, Bagherian-Sararoudi R, Fanian N, Tabatabaie SM. [Predictors of nurses' mental health in medical and surgical wards based on demographic variables (Persian)]. Journal of Research in Behavioural Sciences. 2014; 12(3):369-79.
37. Rasti S, Niazmand H, Heydari HR. [Survey the relationship between quality of work life and mental health in Bushehr prison staff; Case study: Dashtestan Prison Staff (Persian)]. Correction and Upbringing. 2011; 142:48-52.
38. Mostafavi Rad F, Tabe Bordbar F, Zahedi S. [Prediction of mental health through considering organizational justice and quality of work life (Persian)]. Journal of Analytical-Cognitive Psychology. 2011; 2(6):75-87.
| Rights and permissions | |
 | This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Articles Copyright © The Author(s).
Owned by Guilan University of Medical Sciences.
Co-published by Negah Institute for Scientific Communication.
Contact Information
JHNM Office, Guilan University of Medical Sciences P.O.Box 41635-1873, Rasht, Iran
Journal Tel: +9813 33553202
Publisher Tel: +9821 453 55 555; +9821 453 55 000
Email: holisticnmj@gmail.com, nursjournal@gums.ac.ir
