Thu, Apr 25, 2024
Volume 28, Issue 3 (6-2018)
JHNM 2018, 28(3): 179-184 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Jafaryparvar Z, Adib M, Ghanbari Khanghah A, Kazem Nezhad Leyli E. Quality of Life and Associated Factors in Patients Suffering From Burns. JHNM 2018; 28 (3) :179-184
URL: http://hnmj.gums.ac.ir/article-1-531-en.html
URL: http://hnmj.gums.ac.ir/article-1-531-en.html



1- Razi Clinical Research Development Center, Nursing (MSc.), Guilan University of Medical Sciences, Rasht, Iran.
2- Social Determinants of Health Research Center (SDHRC), Instructor, Department of Nursing (Medical-Surgical), Guilan University of Medical Sciences, Rasht, Iran. , adibmasoomeh@yahoo.com
3- Social Determinants of Health Research Center (SDHRC), Department of Nursing (Medical-Surgical), Associate Professor, Guilan University of Medical Sciences, Rasht, Iran.
4- Social Determinants of Health Research Center (SDHRC), Bio-Statistics, Associate Professor, Guilan University of Medical Sciences, Rasht, Iran.
2- Social Determinants of Health Research Center (SDHRC), Instructor, Department of Nursing (Medical-Surgical), Guilan University of Medical Sciences, Rasht, Iran. , adibmasoomeh@yahoo.com
3- Social Determinants of Health Research Center (SDHRC), Department of Nursing (Medical-Surgical), Associate Professor, Guilan University of Medical Sciences, Rasht, Iran.
4- Social Determinants of Health Research Center (SDHRC), Bio-Statistics, Associate Professor, Guilan University of Medical Sciences, Rasht, Iran.
Full-Text [PDF 433 kb]
(1331 Downloads)
| Abstract (HTML) (4896 Views)


Full-Text: (1401 Views)
Introduction
Burn is an accident that could occur across all age groups and socioeconomic classes [1]. The national center for controlling and preventing damages and diseases introduced burn injuries as the fifth common cause of death resulting from unintentional injuries in the USA and the third cause of death in household accidents [2]. Burn has unfavorable effects on the economy of developed and developing countries. In developed countries, severe disabilities resulting from burns lead to considerable financial burden, while in developing countries, the rate of burn-related mortality is high [3]. In the USA, around 45000 individuals undergo burn treatment annually [1]. In Iran, 250000 people experience burn annually; of these, approximately 2000-3000 individuals succumb to death due to the deterioration caused by burns. Nevertheless, this figure has been declining over the past few years in Iran; for instance, in 2003-2004, the number of burn-related deaths was 3000 and is currently 2000 [4]. In the Guilan province in 2013, 11435 patients with burns visited Velayat subspecialty burn and plastic surgery center; 1147 were hospitalized, and 10288 were treated as outpatients [5].
The research and advances in such cases include fluid replacement, immediate burn treatment, treating inhalation injuries, nutritional needs, early debridement, skin grafting, and use of skin replacement that have significantly reduced the mortality resulting from burn accidents [1]. On the other hand, if the burn victims survive, they would experience various psychological and social issues with varying degrees [6]. The most common psychological disorder in burn survivors is Post-Traumatic Stress Disorder (PTSD). Anxiety, depression, and sleep disorders are among the other psychological disorders in burn patients. Consequently, the problems associated with the quality of life are severe, as the patient and their family experience life with new physical problems and challenges in their relationships [1]. Thus, promotion of the quality of life, and in turn, the promotion of health is considered as inseparable parts of socioeconomic development [7].
According to the definition of the World Health Organization (WHO), the quality of life refers to individuals’ understanding about their situation in life in terms of culture, the value system in which they live, and their goals, expectations, standards, and priorities. Accordingly, it is absolutely an individual-oriented concept that is based on the individual’s understanding of different aspects of their lives [8]. The evaluation of the quality of life can assist the burn team in determining the needs of burned patients and identifying the domains of quality of life affected by burns [9]. Given that nurses have a maximum contact with patients and relate to patients from the very early moments after the burn up to years after that, undertake the emotional support provide to the patient and their family, and monitor the treatments [10], they should have an active role in assessing the post-burn quality of life. If required, they should evaluate the mental and psychological status of the burned patients in terms of mental disorder and body image. They should also determine the specific educational needs of the patient and their family for self-care and house care. In addition, they can aid the rehabilitation team in assisting the patient to accept their current situation, develop self-confidence and not depend on others, and eventually return to the family environment and the society [11]. Thus, the present study was carried out with the aim of determining the quality of life and the associated factors in patients suffering from burns hospitalized at Velayat subspecialty burn and plastic surgery center in Rasht, Iran.
Materials and Methods
This cross-sectional analytical study was conducted on patients with burns admitted to Velayat subspecialty burn and plastic surgery center in Rasht between 2008 and 2012. The sample population was determined as 134 based on the study by Pishnamazi et al. in which, the correlation of the quality of life with the duration after the burn was 0.306 [7] with 95% test power in a two-tailed test. With 5% attrition, the final sample population was determined as 139 individuals. The subjects were selected from patients hospitalized from 2008-2012 and based on the following inclusion criteria: age >18 years, passage of at least 6 months after the discharge following burn, no confirmed psychological diseases and mental retardation, no auditory and visual disorders (all based on the patients' file), and the burns were based on American Burn Association classification, which includes the following: partial burn of >25% in adults or >20% in the elderly, third-degree burn ≥10%, all second-degree and third-degree burns of the critical regions (face, eyes, ears, hands, legs, and perineum), burns resulting from harmful chemical substances (acid, base), electrocution with high voltage (above 1000 V), burn due inhalation of toxic substances, trauma, and high-risk patients (diabetes, weakened immune system, and have other underlying diseases) [12, 13].
First, after obtaining permission from the Vice President for research and technology at the Guilan University of Medical Sciences and approval of the Ethics Committee (approval number IR.GUMS.REC.1394.331), the investigator visited Velayat subspecialty burn and plastic surgery center of Guilan University of Medical Sciences in Rasht. Subsequently, a list of patients with burns hospitalized at the center was prepared based on the Health Information System (HIS).
According to the prepared list within the study period, 2365 burn patients had been admitted to the center. The present study is a part of a two-stage research proposal, and in the first stage, 626 individuals were selected from 2365 patients using systematic random sampling, and the mortality rate and hospitalization duration after burns were assessed. In the second stage, 139.626 patients were selected from the first stage using systematic random sampling in order to investigate the quality of life after burns as well as the subsequent complications and problems, such as itching, hypertrophic scar, colloid, hypopigmentation, and hyperpigmentation. Once the patients were informed about voluntary participation, and after they had visited the academic healthcare center, they were invited to visit the researcher on a date previously specified. The participants were informed about the study objectives, and written consent was obtained. They were also assured of the confidentiality of information and were requested to complete the Burn-Specific Health Scale-Brief (BSHS-B). All the questions were read to the patients by the researcher and the questionnaire completed using the patient responses. This questionnaire, designed by Kildal et al. is a standard instrument for the investigation of the specific level of performance and quality of life after burn [14]. It includes 40 questions across nine domains including simple abilities, hand function, effects, body image, interpersonal relationships, sexuality, heat sensitivity, treatment regimen, and work; the reliability and validity have been examined by Pishnamazi et al. [15] in Iran. Each item in this questionnaire had the options of severe (0), relatively high (1), moderate (2), low (3), and not at all (4), scoring from 0-4. Thus, each question in the questionnaire had a minimum score of 0 and a maximum score of 4. Overall, acquiring a high mean score indicated a superior quality of life, while a low mean value suggested a low quality of life.
After completion of the questionnaire, the clinical visit of the patients was conducted by a specialist in the burn clinic, and problems such as itching, hypertrophic scar, colloid, hypopigmentation, and hyperpigmentation were examined and recorded.
Given that this study is a part of a large design, 139 patients were enrolled in the study initially. Despite the 6-month follow-up period for sampling and asking the patient to be present at the mentioned center and be visited freely by a burn specialist, we could collect information on only 67 patients. In telephonic interviews, the presence or absence of post-burn complications and problems were explained to the patients in a simple language. Subsequently, the options were completed based on their responses. A total of 3 patients were unwilling to participate in the research, 2 were excluded due to death caused by stroke, internal hemorrhage, and a thyroid problem, 1 was withdrawn due to Alzheimer’s disease, and 1 was excluded due to migration abroad, and eventually the quality of life of 60 patients was examined. Several patients did not consent to visiting the center, and hence, the interview of 49 patients was conducted via telephone and that of only 11 patients in person. The data were analyzed by SPSS V. 16 based on descriptive statistics (frequency estimation, mean, and standard deviation) as well as inferential statistical tests (Friedman and linear regression tests). In addition, a multivariate regression model was utilized with inclusion and exclusion probability of variables at P=0.1 and P=0.05.
Results
The findings indicated that a majority of the samples (76.7%) consisted of males and 55% were villagers. The mean duration of burn (the time that has passed after the burn) was 3.78±1.14. The mean age of the individuals was 65.45±12.39 (range, 18-35) years, and the mean percentage of burn extent was 9.35±11.85. A total of 65% of patients showed burns in more than one region of the body, and 48.3% had hyperpigmentation at the burnt site (Table 1).
Burn is an accident that could occur across all age groups and socioeconomic classes [1]. The national center for controlling and preventing damages and diseases introduced burn injuries as the fifth common cause of death resulting from unintentional injuries in the USA and the third cause of death in household accidents [2]. Burn has unfavorable effects on the economy of developed and developing countries. In developed countries, severe disabilities resulting from burns lead to considerable financial burden, while in developing countries, the rate of burn-related mortality is high [3]. In the USA, around 45000 individuals undergo burn treatment annually [1]. In Iran, 250000 people experience burn annually; of these, approximately 2000-3000 individuals succumb to death due to the deterioration caused by burns. Nevertheless, this figure has been declining over the past few years in Iran; for instance, in 2003-2004, the number of burn-related deaths was 3000 and is currently 2000 [4]. In the Guilan province in 2013, 11435 patients with burns visited Velayat subspecialty burn and plastic surgery center; 1147 were hospitalized, and 10288 were treated as outpatients [5].
The research and advances in such cases include fluid replacement, immediate burn treatment, treating inhalation injuries, nutritional needs, early debridement, skin grafting, and use of skin replacement that have significantly reduced the mortality resulting from burn accidents [1]. On the other hand, if the burn victims survive, they would experience various psychological and social issues with varying degrees [6]. The most common psychological disorder in burn survivors is Post-Traumatic Stress Disorder (PTSD). Anxiety, depression, and sleep disorders are among the other psychological disorders in burn patients. Consequently, the problems associated with the quality of life are severe, as the patient and their family experience life with new physical problems and challenges in their relationships [1]. Thus, promotion of the quality of life, and in turn, the promotion of health is considered as inseparable parts of socioeconomic development [7].
According to the definition of the World Health Organization (WHO), the quality of life refers to individuals’ understanding about their situation in life in terms of culture, the value system in which they live, and their goals, expectations, standards, and priorities. Accordingly, it is absolutely an individual-oriented concept that is based on the individual’s understanding of different aspects of their lives [8]. The evaluation of the quality of life can assist the burn team in determining the needs of burned patients and identifying the domains of quality of life affected by burns [9]. Given that nurses have a maximum contact with patients and relate to patients from the very early moments after the burn up to years after that, undertake the emotional support provide to the patient and their family, and monitor the treatments [10], they should have an active role in assessing the post-burn quality of life. If required, they should evaluate the mental and psychological status of the burned patients in terms of mental disorder and body image. They should also determine the specific educational needs of the patient and their family for self-care and house care. In addition, they can aid the rehabilitation team in assisting the patient to accept their current situation, develop self-confidence and not depend on others, and eventually return to the family environment and the society [11]. Thus, the present study was carried out with the aim of determining the quality of life and the associated factors in patients suffering from burns hospitalized at Velayat subspecialty burn and plastic surgery center in Rasht, Iran.
Materials and Methods
This cross-sectional analytical study was conducted on patients with burns admitted to Velayat subspecialty burn and plastic surgery center in Rasht between 2008 and 2012. The sample population was determined as 134 based on the study by Pishnamazi et al. in which, the correlation of the quality of life with the duration after the burn was 0.306 [7] with 95% test power in a two-tailed test. With 5% attrition, the final sample population was determined as 139 individuals. The subjects were selected from patients hospitalized from 2008-2012 and based on the following inclusion criteria: age >18 years, passage of at least 6 months after the discharge following burn, no confirmed psychological diseases and mental retardation, no auditory and visual disorders (all based on the patients' file), and the burns were based on American Burn Association classification, which includes the following: partial burn of >25% in adults or >20% in the elderly, third-degree burn ≥10%, all second-degree and third-degree burns of the critical regions (face, eyes, ears, hands, legs, and perineum), burns resulting from harmful chemical substances (acid, base), electrocution with high voltage (above 1000 V), burn due inhalation of toxic substances, trauma, and high-risk patients (diabetes, weakened immune system, and have other underlying diseases) [12, 13].
First, after obtaining permission from the Vice President for research and technology at the Guilan University of Medical Sciences and approval of the Ethics Committee (approval number IR.GUMS.REC.1394.331), the investigator visited Velayat subspecialty burn and plastic surgery center of Guilan University of Medical Sciences in Rasht. Subsequently, a list of patients with burns hospitalized at the center was prepared based on the Health Information System (HIS).
According to the prepared list within the study period, 2365 burn patients had been admitted to the center. The present study is a part of a two-stage research proposal, and in the first stage, 626 individuals were selected from 2365 patients using systematic random sampling, and the mortality rate and hospitalization duration after burns were assessed. In the second stage, 139.626 patients were selected from the first stage using systematic random sampling in order to investigate the quality of life after burns as well as the subsequent complications and problems, such as itching, hypertrophic scar, colloid, hypopigmentation, and hyperpigmentation. Once the patients were informed about voluntary participation, and after they had visited the academic healthcare center, they were invited to visit the researcher on a date previously specified. The participants were informed about the study objectives, and written consent was obtained. They were also assured of the confidentiality of information and were requested to complete the Burn-Specific Health Scale-Brief (BSHS-B). All the questions were read to the patients by the researcher and the questionnaire completed using the patient responses. This questionnaire, designed by Kildal et al. is a standard instrument for the investigation of the specific level of performance and quality of life after burn [14]. It includes 40 questions across nine domains including simple abilities, hand function, effects, body image, interpersonal relationships, sexuality, heat sensitivity, treatment regimen, and work; the reliability and validity have been examined by Pishnamazi et al. [15] in Iran. Each item in this questionnaire had the options of severe (0), relatively high (1), moderate (2), low (3), and not at all (4), scoring from 0-4. Thus, each question in the questionnaire had a minimum score of 0 and a maximum score of 4. Overall, acquiring a high mean score indicated a superior quality of life, while a low mean value suggested a low quality of life.
After completion of the questionnaire, the clinical visit of the patients was conducted by a specialist in the burn clinic, and problems such as itching, hypertrophic scar, colloid, hypopigmentation, and hyperpigmentation were examined and recorded.
Given that this study is a part of a large design, 139 patients were enrolled in the study initially. Despite the 6-month follow-up period for sampling and asking the patient to be present at the mentioned center and be visited freely by a burn specialist, we could collect information on only 67 patients. In telephonic interviews, the presence or absence of post-burn complications and problems were explained to the patients in a simple language. Subsequently, the options were completed based on their responses. A total of 3 patients were unwilling to participate in the research, 2 were excluded due to death caused by stroke, internal hemorrhage, and a thyroid problem, 1 was withdrawn due to Alzheimer’s disease, and 1 was excluded due to migration abroad, and eventually the quality of life of 60 patients was examined. Several patients did not consent to visiting the center, and hence, the interview of 49 patients was conducted via telephone and that of only 11 patients in person. The data were analyzed by SPSS V. 16 based on descriptive statistics (frequency estimation, mean, and standard deviation) as well as inferential statistical tests (Friedman and linear regression tests). In addition, a multivariate regression model was utilized with inclusion and exclusion probability of variables at P=0.1 and P=0.05.
Results
The findings indicated that a majority of the samples (76.7%) consisted of males and 55% were villagers. The mean duration of burn (the time that has passed after the burn) was 3.78±1.14. The mean age of the individuals was 65.45±12.39 (range, 18-35) years, and the mean percentage of burn extent was 9.35±11.85. A total of 65% of patients showed burns in more than one region of the body, and 48.3% had hyperpigmentation at the burnt site (Table 1).
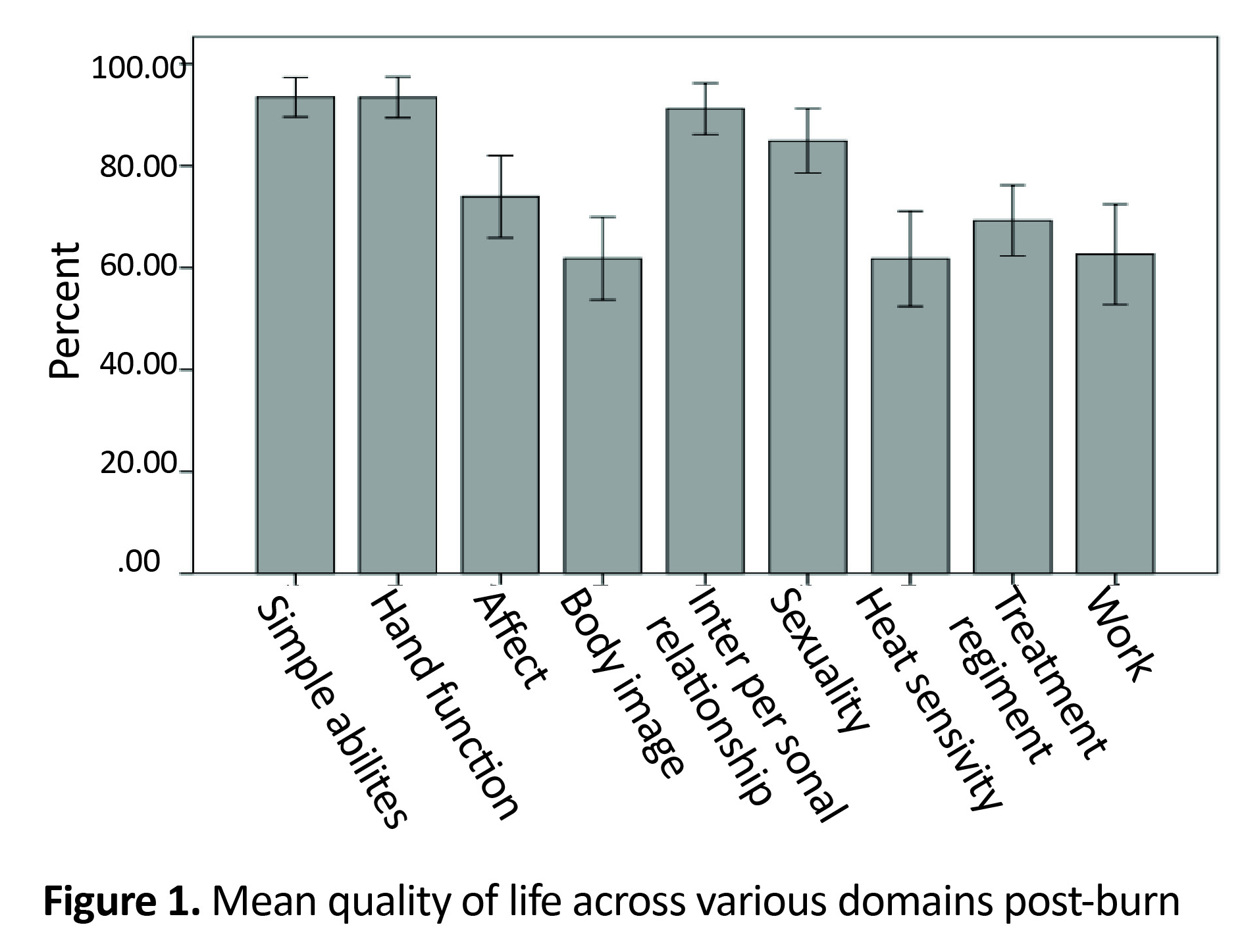
In investigating the post-burn quality of life, since the data did not follow a normal distribution, Friedman test was used, which revealed a significant difference in the post-burn quality of life among the different aspects of the quality of life (P=0.0001). The mean total score of the post-burn quality of life was 76.9±20.74 out of 100. Among the nine aspects of the quality of life, the percentage of the heat sensitivity domain of the burnt site was lower as compared to the other domains (61.75%). Furthermore, the percentage of the ability to perform simple activities was higher than the other domains (93.47%) (Figure 1).
While investigating the factors affecting the quality of life of patients after burn, the extent of the burn was found to be a predictive factor for the quality of life, and the extent of burn had an inverse relationship with the quality of life of patients (Table 2).
Discussion
The present results indicated that 1.3rd of the patients had hypertrophic scar, around 1.3rd had colloid, and half of them had hyperpigmentation and itching at the site of burn. The study by Holavanahalli et al. demonstrated that of the 98 patients with severe burn in the USA, 72% had itching, 66% had hypertrophic scar, and 53% suffered from hyperpigmentation in the grafted regions [16]. The difference between the results of the present study and those from the study by Holavanahalli et al. may be attributed to the different inclusion criteria. The previous study included patients with 30% burns and above after ≥3 years post-burn. Nonetheless, in the present study, all of the burn patients were included based on the American Burn Association classification. While investigating the post-burn quality of life, the mean domain of heat sensitivity of the burn site was lower than that of the other domains. In addition, the maximum required score was related to simple abilities. The domains of body image and work obtained the minimum scores after the heat sensitivity of the burn site. The study by Pishnamazi et al. on 200 patients revealed that the mean score of the psychological domain of the burn patients’ quality of life was lower than that of the other domains, where the maximum acquired score was related to the physical domain [7].
The study by Elsherbiny et al. on patients with severe burns in Egypt showed that the minimum scores were related to heat sensitivity, site of burn, work, affects, and body image. On the other hand, the maximum scores were related to interpersonal relationships and sexual function, simple abilities, and hand function [9]. However, in the present study, the low scores of the body image could be attributed to the presence of burn scars and complications resulting from the burn. Furthermore, Rahzani et al. demonstrated that the complications such as scar and deformity at the site of burn had caused patients to lose their self-confidence, hide their deformity, and confine themselves within specific frameworks [17]. The deformity and abnormalities resulting from different factors such as burn, accident, and surgery developed unfavorable psychological and behavioral changes in the affected individuals. Irrespective of the treatment and cost, these deformities might lead to personal and social behavioral abnormalities including avoidance, severing familial and social relations, as well as, depression [18].
In the present study, most of the subjects had returned to their previous job, while in the study by Pavoni et al. in Italy on patients with severe burns, none of the participants had returned to their previous job [19]. This difference might be attributed to the different inclusion criteria of patients with severe burns in the two studies. Herein, all the patients with severe burns, according to American Burn Association classification, were included, while those in the study by Pavoni et al. included only patients with severe burns (or 40%) admitted in the ICU ward requiring mechanical ventilator [19].
While investigating the factors associated with the quality of life, among the studied variables, only the extent of the burn was a predictor of the specific quality of life post-burn. On the other hand, Anzarut et al. studied patients with severe burns in Canada and proposed that the extent of the burn was not a predictor for the quality of life after burn [20]. These differences in the results could be attributed to the different inclusion criteria. However, the study included patients with ≥50% burn and a minimum age of 14 years [20]. Conversely, in the present study, the samples had been included based on severe burn criteria and a minimum age of 18 years.
Based on the current findings, it can be concluded that despite 2-6 years after the burn, the patients continued to face challenges of post-burn problems and complications. Even low-extent burns could adversely influence the quality of life of these individuals. In the present study, the burn patients exhibited major concerns in the domains of heat sensitivity of the burnt site, body image, and work. Thus, free annual visits of burn patients in burn clinic and re-constructive surgeries on the burnt regions are some of the recommended measures. In addition, providing psychological and mental support and rehabilitation for these individuals after discharge from the hospital should be emphasized, and measures should be taken to establish an association for supporting the burn patients in the Guilan province.
The limitations of the present study were as follows: low sample size, attrition of a large number of samples due to the incorrect address and telephone number of patients, and unavailability of patients to participate in the research. Since nurses constitute a major part of the burn treatment team, their knowledge on the quality of life after burn and the associated factors can set a suitable therapeutic and educational plan for the burn patients. Also, if required, they can refer the burn patients to clinical psychologists and consultants. The results of the present study can also be used as basic information for in order to investigate the post-burn quality of life and the associated factors. Nevertheless, additional studies on other variables associated with the quality of life of these patients are essential.
Ethical Considerations
Compliance with ethical guidelines
Once the patients were informed about voluntary participation, and after they had visited the academic healthcare center, they were invited to visit the researcher on a date previously specified date. The participants were informed about the study objectives, and written consent was obtained. They were also assured of the confidentiality of information and were requested to complete the Burn-Specific Health Scale-Brief (BSHS-B).
Funding
The vice president position for Research and Technology of Guilan University of Medical Sciences is highly appreciated for the financial support of this study.
Conflict of interest
No conflict of interest has been declared by the authors.
Acknowledgements
We would also like to appreciate the research center for executive factors affecting health, Dr Arman Parvizi, the head of Velayat subspecialty burn and plastic surgery Center, Dr Mohamadreza Mobayen, Fellowship of Burn, who provided free visits to burn clinic, and all individuals who cooperated in this study, especially patients with burn and the personnel of Velayat subspecialty burn and plastic surgery Center.
References
The present results indicated that 1.3rd of the patients had hypertrophic scar, around 1.3rd had colloid, and half of them had hyperpigmentation and itching at the site of burn. The study by Holavanahalli et al. demonstrated that of the 98 patients with severe burn in the USA, 72% had itching, 66% had hypertrophic scar, and 53% suffered from hyperpigmentation in the grafted regions [16]. The difference between the results of the present study and those from the study by Holavanahalli et al. may be attributed to the different inclusion criteria. The previous study included patients with 30% burns and above after ≥3 years post-burn. Nonetheless, in the present study, all of the burn patients were included based on the American Burn Association classification. While investigating the post-burn quality of life, the mean domain of heat sensitivity of the burn site was lower than that of the other domains. In addition, the maximum required score was related to simple abilities. The domains of body image and work obtained the minimum scores after the heat sensitivity of the burn site. The study by Pishnamazi et al. on 200 patients revealed that the mean score of the psychological domain of the burn patients’ quality of life was lower than that of the other domains, where the maximum acquired score was related to the physical domain [7].
The study by Elsherbiny et al. on patients with severe burns in Egypt showed that the minimum scores were related to heat sensitivity, site of burn, work, affects, and body image. On the other hand, the maximum scores were related to interpersonal relationships and sexual function, simple abilities, and hand function [9]. However, in the present study, the low scores of the body image could be attributed to the presence of burn scars and complications resulting from the burn. Furthermore, Rahzani et al. demonstrated that the complications such as scar and deformity at the site of burn had caused patients to lose their self-confidence, hide their deformity, and confine themselves within specific frameworks [17]. The deformity and abnormalities resulting from different factors such as burn, accident, and surgery developed unfavorable psychological and behavioral changes in the affected individuals. Irrespective of the treatment and cost, these deformities might lead to personal and social behavioral abnormalities including avoidance, severing familial and social relations, as well as, depression [18].
In the present study, most of the subjects had returned to their previous job, while in the study by Pavoni et al. in Italy on patients with severe burns, none of the participants had returned to their previous job [19]. This difference might be attributed to the different inclusion criteria of patients with severe burns in the two studies. Herein, all the patients with severe burns, according to American Burn Association classification, were included, while those in the study by Pavoni et al. included only patients with severe burns (or 40%) admitted in the ICU ward requiring mechanical ventilator [19].
While investigating the factors associated with the quality of life, among the studied variables, only the extent of the burn was a predictor of the specific quality of life post-burn. On the other hand, Anzarut et al. studied patients with severe burns in Canada and proposed that the extent of the burn was not a predictor for the quality of life after burn [20]. These differences in the results could be attributed to the different inclusion criteria. However, the study included patients with ≥50% burn and a minimum age of 14 years [20]. Conversely, in the present study, the samples had been included based on severe burn criteria and a minimum age of 18 years.
Based on the current findings, it can be concluded that despite 2-6 years after the burn, the patients continued to face challenges of post-burn problems and complications. Even low-extent burns could adversely influence the quality of life of these individuals. In the present study, the burn patients exhibited major concerns in the domains of heat sensitivity of the burnt site, body image, and work. Thus, free annual visits of burn patients in burn clinic and re-constructive surgeries on the burnt regions are some of the recommended measures. In addition, providing psychological and mental support and rehabilitation for these individuals after discharge from the hospital should be emphasized, and measures should be taken to establish an association for supporting the burn patients in the Guilan province.
The limitations of the present study were as follows: low sample size, attrition of a large number of samples due to the incorrect address and telephone number of patients, and unavailability of patients to participate in the research. Since nurses constitute a major part of the burn treatment team, their knowledge on the quality of life after burn and the associated factors can set a suitable therapeutic and educational plan for the burn patients. Also, if required, they can refer the burn patients to clinical psychologists and consultants. The results of the present study can also be used as basic information for in order to investigate the post-burn quality of life and the associated factors. Nevertheless, additional studies on other variables associated with the quality of life of these patients are essential.
Ethical Considerations
Compliance with ethical guidelines
Once the patients were informed about voluntary participation, and after they had visited the academic healthcare center, they were invited to visit the researcher on a date previously specified date. The participants were informed about the study objectives, and written consent was obtained. They were also assured of the confidentiality of information and were requested to complete the Burn-Specific Health Scale-Brief (BSHS-B).
Funding
The vice president position for Research and Technology of Guilan University of Medical Sciences is highly appreciated for the financial support of this study.
Conflict of interest
No conflict of interest has been declared by the authors.
Acknowledgements
We would also like to appreciate the research center for executive factors affecting health, Dr Arman Parvizi, the head of Velayat subspecialty burn and plastic surgery Center, Dr Mohamadreza Mobayen, Fellowship of Burn, who provided free visits to burn clinic, and all individuals who cooperated in this study, especially patients with burn and the personnel of Velayat subspecialty burn and plastic surgery Center.
References
- Hinkle JL, Cheever KH. Brunner & Suddarth Handbook of medical-surgical nursing [T Najafi, M Zeynali, Persian trans.]. 13rd ed. Tehran: Jame'e Negar; 2014.
- Smeltzer SC, Bare BG, Hinkle JL, Cheever KH. Textbook of medical-surgical nursing [T Najafi, M Zeynali, Persian trans.]. 12nd ed. Tehran: Jame'e Negar; 2010.
- Herndon DN. Total burn care. Amsterdam: Elsevier Health Sciences; 2007.
- The statistics of burn warning in Iran [Internet]. 2015 February 26. Available from: http://press.jamejamonline.ir/Newspreview/1846637177117442336
- Zahedsefat T. [Introducing Velayat Subspecialty Burn and Reconstructive Surgery Center (Persian)]. Eltiyam Educational Quarterly Newsletter. 2014; 4.
- Rashidinejad M, Karimi A, Jafarpoor M, Mohammadi M. [Psychosocial problems of clients suffering from burn deformities (Persian)]. Iran Journal of Nursing. 2001; 13(26):44-9.
- Pishnamazi Z, Kianiasiabar A, Heravi-Karimooi M, Zaeri F, Noorozzadeh R. [Quality of life in burn patients (Persian)]. Payesh. 2011; 11(1):103-10.
- Bonomi AE, Patrick DL, Bushnell DM, Martin M. Validation of the United States' version of the World Health Organization Quality of Life (WHOQOL) instrument. Journal of Clinical Epidemiology. 2000; 53(1):1-12. [DOI:10.1016/S0895-4356(99)00123-7]
- Elsherbiny OE, Salem MA, El-Sabbagh AH, Elhadidy MR, Eldeen SM. Quality of life of adult patients with severe burns. Burns. 2011; 37(5):776-89. [DOI:10.1016/j.burns.2010.12.017] [PMID]
- Rafii F. [Design theory, nursing care of burn patients (Persian)][PhD dissertation]. Tehran: Iran University of Medical Sciences; 2004. .
- Mirzabeygi Gh, Givry A. [Burn nurse`s specialized duties (Persian)]. Available from: file:///C:/Users/Raoufe%20Moshref/Downloads/%D9%BE%D8%B1%D8%B3%D8%AA%D8%A7%D8%B1%DB%8C%20%D8%AC%D8%AF%DB%8C%D8%AF.pdf
- Azar M, Abadi N, Aslani J, Afshar R, Emam M, Bidari A, et al. [Emergency Internal Medicine (Persian)]. Tehran: Noore Danesh; 2008.
- Noursalehi E, Gholipour A. [Practical Management: Children's burns (Persian)]. Tehran: Arjmand; 2011.
- Kildal M, Andersson G, Fugl Meyer AR, Lannerstam K, Gerdin B. Development of a brief version of the Burn Specific Health Scale (BSHS-B). Journal of Trauma-Injury, Infection, and Critical Care. 2001; 51(4):740-6. [DOI:10.1097/00005373-200110000-00020]
- Pishnamazi Z, Rejeh N, Heravi Karimooi M, Vaismoradi M. Validation of the Persian version of the Burn Specific Health Scale – Brief. Burns. 2013; 39(1):162–7. [DOI:10.1016/j.burns.2012.05.002]
- Holavanahalli RK, Helm PA, Kowalske KJ. Long-term outcomes in patients surviving large burns: the skin. Journal of Burn Care & Research. 2010; 31(4):631-9. [DOI:10.1097/BCR.0b013e3181e4ca62] [PMID]
- Rahzani K, Taleghani F, Nasrabadi AN, Malekirad A, Rezaei K. [Quality of life in burn disfigurement individuals as life in suffocation: A qualitative study (Persian)]. Nursing Research. 2012; 7(26):11-22.
- Malekmohammadi M, Tehrani HA, Aghdami N. [Skin structure and wound healing phases (Persian)]. Dermatology & Cosmetic. 2011; 2(4):229- 44.
- Pavoni V, Gianesello L, Paparella L, Buoninsegni L, Barboni E. Outcome predictors and quality of life of severe burn patients admitted to intensive care unit. Scandinavian Journal of Trauma, Resuscitation and Emergency Medicine. 2010; 18(1):24. [DOI:10.1186/1757-7241-18-24]
- Anzarut A, Chen M, Shankowsky H, Tredget EE. Quality-of-life and outcome predictors following massive burn injury. Plastic and Reconstructive Surgery. 2005; 116(3):791-7. [DOI:10.1097/01.prs.0000176257.22583.4b] [PMID]
Article Type : Applicable |
Subject:
Special
Received: 2015/09/29 | Accepted: 2015/11/10 | Published: 2018/06/15
Received: 2015/09/29 | Accepted: 2015/11/10 | Published: 2018/06/15
References
1. Hinkle JL, Cheever KH. Brunner & Suddarth Handbook of medical-surgical nursing [T Najafi, M Zeynali, Persian trans.]. 13rd ed. Tehran: Jame'e Negar; 2014.
2. Smeltzer SC, Bare BG, Hinkle JL, Cheever KH. Textbook of medical-surgical nursing [T Najafi, M Zeynali, Persian trans.]. 12nd ed. Tehran: Jame'e Negar; 2010.
3. Herndon DN. Total burn care. Amsterdam: Elsevier Health Sciences; 2007.
4. The statistics of burn warning in Iran [Internet]. 2015 February 26. Available from: http://press.jamejamonline.ir/Newspreview/1846637177117442336
5. Zahedsefat T. [Introducing Velayat Subspecialty Burn and Reconstructive Surgery Center (Persian)]. Eltiyam Educational Quarterly Newsletter. 2014; 4.
6. Rashidinejad M, Karimi A, Jafarpoor M, Mohammadi M. [Psychosocial problems of clients suffering from burn deformities (Persian)]. Iran Journal of Nursing. 2001; 13(26):44-9.
7. Pishnamazi Z, Kianiasiabar A, Heravi-Karimooi M, Zaeri F, Noorozzadeh R. [Quality of life in burn patients (Persian)]. Payesh. 2011; 11(1):103-10.
8. Bonomi AE, Patrick DL, Bushnell DM, Martin M. Validation of the United States' version of the World Health Organization Quality of Life (WHOQOL) instrument. Journal of Clinical Epidemiology. 2000; 53(1):1-12. [DOI:10.1016/S0895-4356(99)00123-7] [DOI:10.1016/S0895-4356(99)00123-7]
9. Elsherbiny OE, Salem MA, El-Sabbagh AH, Elhadidy MR, Eldeen SM. Quality of life of adult patients with severe burns. Burns. 2011; 37(5):776-89. [DOI:10.1016/j.burns.2010.12.017] [PMID] [DOI:10.1016/j.burns.2010.12.017]
10. Rafii F. [Design theory, nursing care of burn patients (Persian)][PhD dissertation]. Tehran: Iran University of Medical Sciences; 2004. .
11. Mirzabeygi Gh, Givry A. [Burn nurse`s specialized duties (Persian)]. Available from: file:///C:/Users/Raoufe%20Moshref/Downloads/%D9%BE%D8%B1%D8%B3%D8%AA%D8%A7%D8%B1%DB%8C%20%D8%AC%D8%AF%DB%8C%D8%AF.pdf
12. Azar M, Abadi N, Aslani J, Afshar R, Emam M, Bidari A, et al. [Emergency Internal Medicine (Persian)]. Tehran: Noore Danesh; 2008.
13. Noursalehi E, Gholipour A. [Practical Management: Children's burns (Persian)]. Tehran: Arjmand; 2011.
14. Kildal M, Andersson G, Fugl Meyer AR, Lannerstam K, Gerdin B. Development of a brief version of the Burn Specific Health Scale (BSHS-B). Journal of Trauma-Injury, Infection, and Critical Care. 2001; 51(4):740-6. [DOI:10.1097/00005373-200110000-00020] [DOI:10.1097/00005373-200110000-00020]
15. Pishnamazi Z, Rejeh N, Heravi Karimooi M, Vaismoradi M. Validation of the Persian version of the Burn Specific Health Scale – Brief. Burns. 2013; 39(1):162–7. [DOI:10.1016/j.burns.2012.05.002] [DOI:10.1016/j.burns.2012.05.002]
16. Holavanahalli RK, Helm PA, Kowalske KJ. Long-term outcomes in patients surviving large burns: the skin. Journal of Burn Care & Research. 2010; 31(4):631-9. [DOI:10.1097/BCR.0b013e3181e4ca62] [PMID] [DOI:10.1097/BCR.0b013e3181e4ca62]
17. Rahzani K, Taleghani F, Nasrabadi AN, Malekirad A, Rezaei K. [Quality of life in burn disfigurement individuals as life in suffocation: A qualitative study (Persian)]. Nursing Research. 2012; 7(26):11-22.
18. Malekmohammadi M, Tehrani HA, Aghdami N. [Skin structure and wound healing phases (Persian)]. Dermatology & Cosmetic. 2011; 2(4):229- 44.
19. Pavoni V, Gianesello L, Paparella L, Buoninsegni L, Barboni E. Outcome predictors and quality of life of severe burn patients admitted to intensive care unit. Scandinavian Journal of Trauma, Resuscitation and Emergency Medicine. 2010; 18(1):24. [DOI:10.1186/1757-7241-18-24] [DOI:10.1186/1757-7241-18-24]
20. Anzarut A, Chen M, Shankowsky H, Tredget EE. Quality-of-life and outcome predictors following massive burn injury. Plastic and Reconstructive Surgery. 2005; 116(3):791-7. [DOI:10.1097/01.prs.0000176257.22583.4b] [PMID] [DOI:10.1097/01.prs.0000176257.22583.4b]
Send email to the article author
| Rights and permissions | |
 | This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Articles Copyright © The Author(s).
Owned by Guilan University of Medical Sciences.
Co-published by Negah Institute for Scientific Communication.
Contact Information
JHNM Office, Guilan University of Medical Sciences P.O.Box 41635-1873, Rasht, Iran
Journal Tel: +9813 33553202
Publisher Tel: +9821 453 55 555; +9821 453 55 000
Email: holisticnmj@gmail.com, nursjournal@gums.ac.ir
