Thu, Jan 1, 2026
Volume 35, Issue 3 (6-2025)
JHNM 2025, 35(3): 200-207 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Shabani M, Pourghane P, Mahdavi Roshan M, Atrkar Roushan Z. Investigating Food Insecurity and Its Socioeconomic Factors in Older People. JHNM 2025; 35 (3) :200-207
URL: http://hnmj.gums.ac.ir/article-1-2401-en.html
URL: http://hnmj.gums.ac.ir/article-1-2401-en.html


1- Master's Student in Geriatric Nursing, Zeynab School of Nursing and Midwifery, Guilan University of Medical Sciences, Rasht, Iran.
2- Associate Professor, Department of Nursing, Zeynab School of Nursing and Midwifery, Guilan University of Medical Sciences, Rasht, Iran. ,pourghanep@gmail.com
3- Associate Professor, Cardiovascular Diseases Research Center, School of Medicine, Guilan University of Medical Sciences, Rasht, Iran.
4- Associate Professor, Department of Community Medicine, School of Medicine, Guilan University of Medical Sciences, Rasht, Iran.
2- Associate Professor, Department of Nursing, Zeynab School of Nursing and Midwifery, Guilan University of Medical Sciences, Rasht, Iran. ,
3- Associate Professor, Cardiovascular Diseases Research Center, School of Medicine, Guilan University of Medical Sciences, Rasht, Iran.
4- Associate Professor, Department of Community Medicine, School of Medicine, Guilan University of Medical Sciences, Rasht, Iran.
Full-Text [PDF 495 kb]
(304 Downloads)
| Abstract (HTML) (483 Views)
Full-Text: (143 Views)
Introduction
The increase in the older population in countries is associated with greater vulnerability and disability. These negative health consequences have a direct impact on access to sufficient food and food insecurity. The older the head of household, the lower the likelihood of food security in the family [1, 2]. Experimental evidence shows that the prevalence of food insecurity among older people is very high due to physical limitations, poor heart conditions, social isolation, and lack of means of transport [3].
Food security is defined as a situation in which all people have access to adequate, safe, and nutritious food at all times to maintain a healthy and active life [4]. Food insecurity, on the other hand, exists when individuals lack full social, economic, and physical access to adequate and healthy food at all times, thereby failing to meet their nutritional needs for a healthy and active life [5]. Household food insecurity, which occurs when a person or family lacks access to food due to financial or other constraints, is a growing public health problem in most developed countries, especially in cases where there is inequality in food sharing [6].
Food insecurity affects more than 820 million people worldwide [7]. The results of recent research in Iran have shown that 73% of urban households experience food security, while 27% face food insecurity [8]. Food insecurity is a major risk factor for malnutrition and has negative consequences for the health of the population [9, 10].
Meanwhile, nutritional poverty in older adults who sometimes have poor dietary patterns is associated with a higher risk of malnutrition, weakness, worsening health conditions, disability, adverse effects on their quality of life and health, and functional impairments. Lack of home, isolation, gender, financial vulnerability, and poor health statistically have significant associations with food insecurity [11].
Population aging is a global challenge for the social and economic development of the world. With advances in the health system, the overall population and, consequently, the older population worldwide have increased, particularly in the 21st century, thereby increasing the need to address this issue [12, 13]. It is estimated that over the next 30 years, the older population will comprise approximately 20% of the world’s population, resulting in a total of two billion older individuals by 2050, meaning that for every five people in the world, one will be aged 65 or older [14].
Additionally, Iran, as a developing country, is also rapidly aging due to changes in various health policies over the past few decades [15]. According to the 2016 census of the Iranian Statistics Center, the total older population of the country is estimated to be 7,414,091 people, and the number of older people in Guilan (the oldest province in the country) is 335,313 (163,438 men and 171,875 women) [16].
Considering the older population of Guilan Province in Iran, this study aimed to investigate food insecurity and socioeconomic factors affecting it among older people visiting comprehensive health centers in the east of Guilan.
Materials and Methods
The study sample for this cross-sectional analytical study consisted of 245 older individuals attending comprehensive health centers in East Guilan. The study sample size was determined based on the results of a similar study [2], which found that 43% of its samples experienced food insecurity (p=0.43, d=0.06, α=0.05). The sampling method employed a multi-stage cluster design. Six clusters were selected from the comprehensive health centers in East Guilan, located in 6 cities (Langerud, Lahijan, Astana, Rudsar, Siahkal, and Amlash). Then one center was randomly selected from each city. Then, the seniors in question were chosen systematically at random at each center.
The inclusion criteria were as follows: 60 years and older, willingness to participate in the study, having health records in comprehensive urban health service centers ability to answer questionnaires through interviews, score above 7 in the Abbreviated Mental Test (AMT) cognitive status test, and completion of the questionnaire.
The research tools included the demographic profile questionnaire, the Household Food Insecurity Access Score (HFIAS), the food security questionnaire, and the Socioeconomic Status (SES) questionnaire. Qualified samples were first assessed with the AMT instrument and entered into the study if they had normal cognitive status. AMT is a cognitive test, originally presented by Hodkinson. This test consisted of 10 questions assessing distant memory, close memory, attention, and orientation. The correct answer to each question scores 1, and an overall score lower than 7 indicates cognitive impairment [17]. The reliability and validity of the questionnaire in Iran were determined by Bakhtiari et al. in older adults [18].
The HFIAS food insecurity questionnaire (in terms of access) consists of 9 questions about the occurrence of food insecurity, followed by recurrence, ranked by severity of food insecurity (in terms of access). For each question (phrase), 4 response options are considered about the number of times the situation has been experienced, including asking how many times (0=never, 1=rarely [once or twice], 2=sometimes [three to ten times], 3=often [more than ten times] during the one-month time frame (30 days ago). In assessing food insecurity (in terms of accessibility) in the community, the data from this questionnaire can be used both quantitatively and qualitatively to evaluate food insecurity in the studied community. The HFIAS score is a continuous measure of an older person’s food insecurity over the past month, derived from a total of occurrence codes answered by the older for 9 questions. The lowest score is 0, and the highest score is 27. The higher the elder’s score, the more food insecurity they experienced. The household food insecurity access prevalence qualitative measure is also used to report the frequency of food insecurity (in terms of access) among older and regional decision-makers. This criterion divides the older population into 4 groups based on insecurity: Food-safe (0-1 points), food-insecure, including mild (2-7 points), moderate (8-14 points), and severe (15-27 points). The higher the number of positive responses of the older to the questions or the more frequently they experienced insecure situations, the more likely they were to be classified as insecure [19].
The SES questionnaire of powerhouse, which comprises four components: Income level, economic class, education, and housing status, along with a total of six demographic questions and five main questions. The measurement comparison of the questions in this questionnaire has five options, and the scoring method is in order from very low (1) to very high (5). Eslami et al. confirmed the validity and internal consistency of this questionnaire [20]. A researcher-made questionnaire, based on similar studies, was used to determine economic and social status [20, 21].
Data collection in this study began with the use of the AMT test in the first step to assess cognitive status. If there was no cognitive impairment, the subjects were included in the study. Following this, demographic characteristics (such as age, gender, marital status, education, occupation, and income), the HFIAS food security questionnaire, and the SES questionnaire were completed.
For statistical analysis, descriptive statistics were employed, and descriptive indicators such as Mean±SD, and univariate chi-square tests were utilized. The simultaneous effect of independent variables on severe food insecurity was shown through multiple logistic regression. Data analysis was performed using SPSS software, version 16.
Results
Two hundred forty-five older people, all of whom had an AMT score greater than 7, were included in the study. The sample consisted of 50.6% males and 49.4% females. The mean age of the samples was 67.66±6.059 years, and all were residents of the town. The occupational status of most people was as follows: 42.4% of households, 82% lived with their spouses, 81.2% were married, 50.6% had incomes above 315 USD, and 30.6% had a level of education below a diploma. About 61.2% had an underlying disease; most of them, 25.7%, had four children. In most households, 53.1% had at least one employed family member, and 34.3% had three or more people living together. Table 1 provides demographic information.
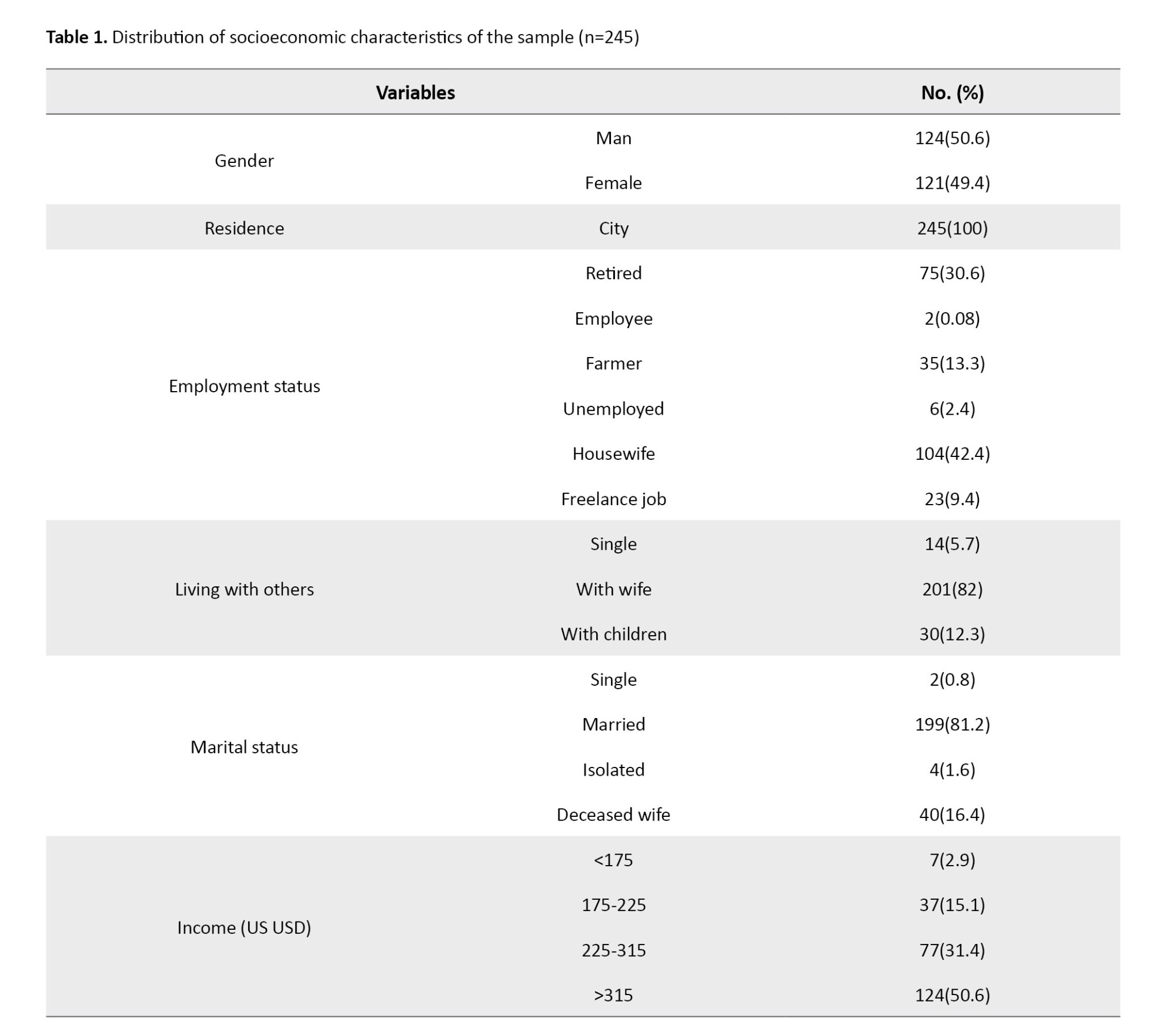
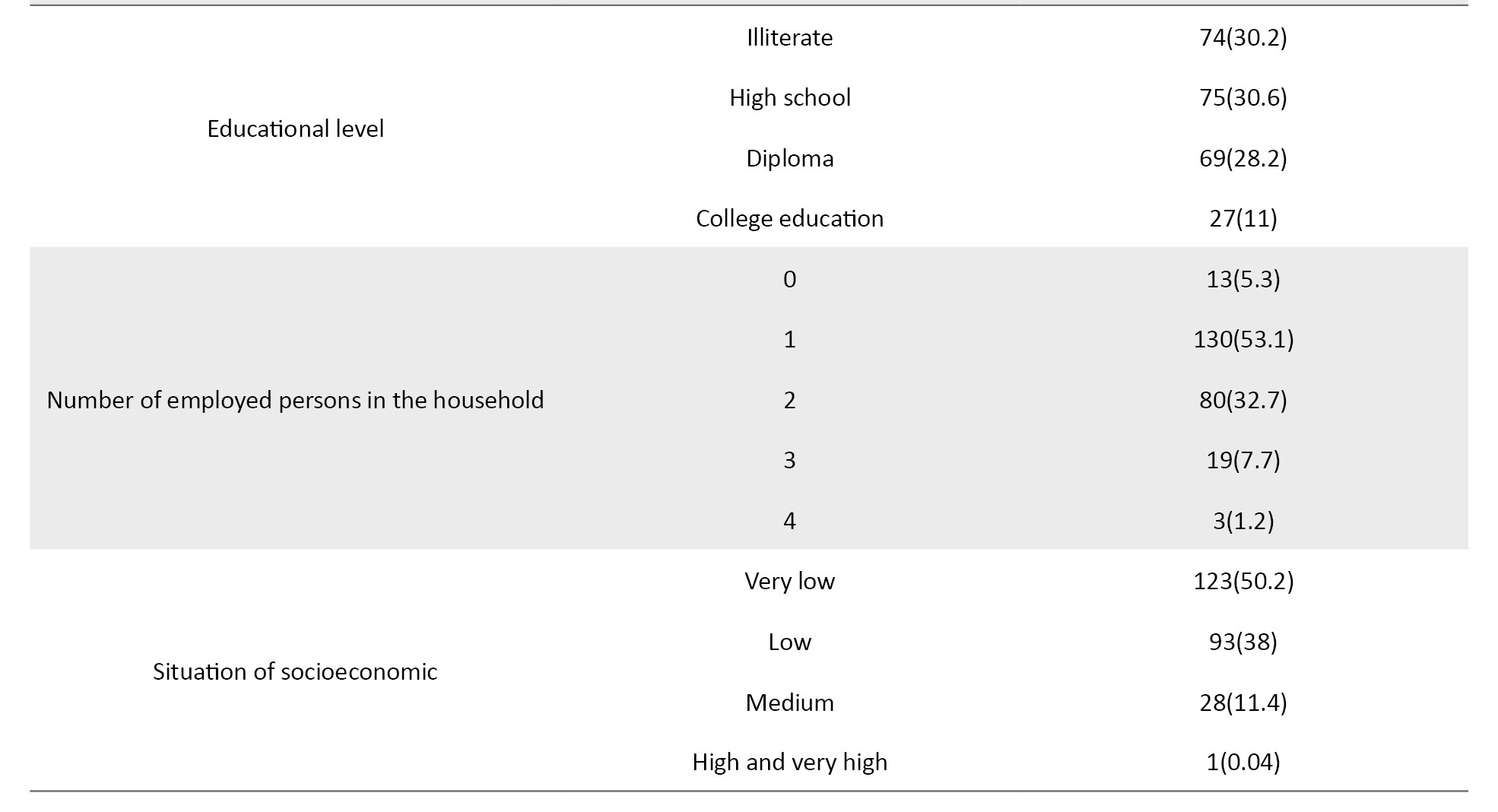
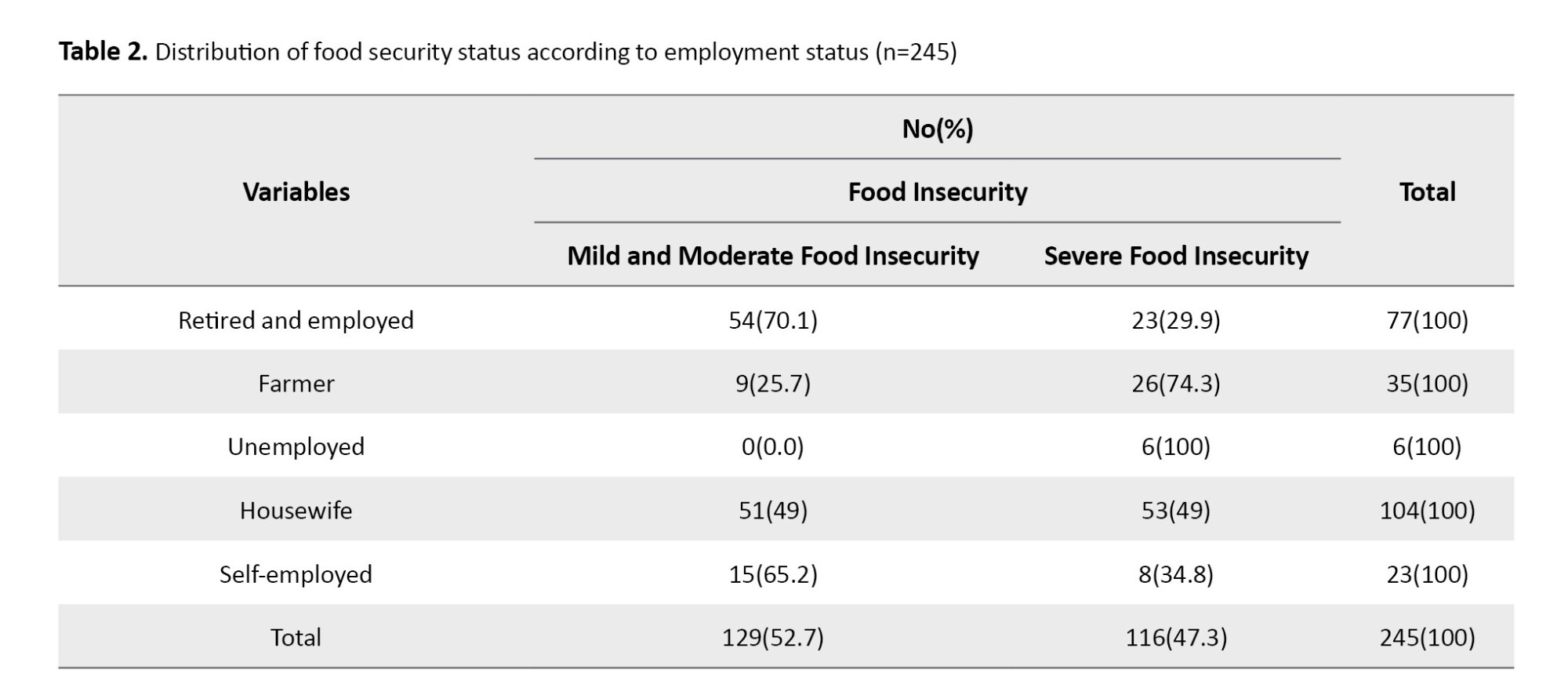
Table 2 shows that, in terms of SES, 74% of individuals with a very low SES experience severe food insecurity, while only 3.4% of those with a high or very high SES experience food insecurity. In terms of food security, 0.4% had complete food security, 11.8% had mild insecurity, 43.7% had moderate food insecurity, and 44.1% also had severe food insecurity.
For statistical analysis, descriptive statistics and descriptive indicators, such as Mean±SD, ratio, and univariate chi-square tests, will be used to illustrate the simultaneous effect of independent variables on severe food insecurity through multiple logistic regression (Table 3).
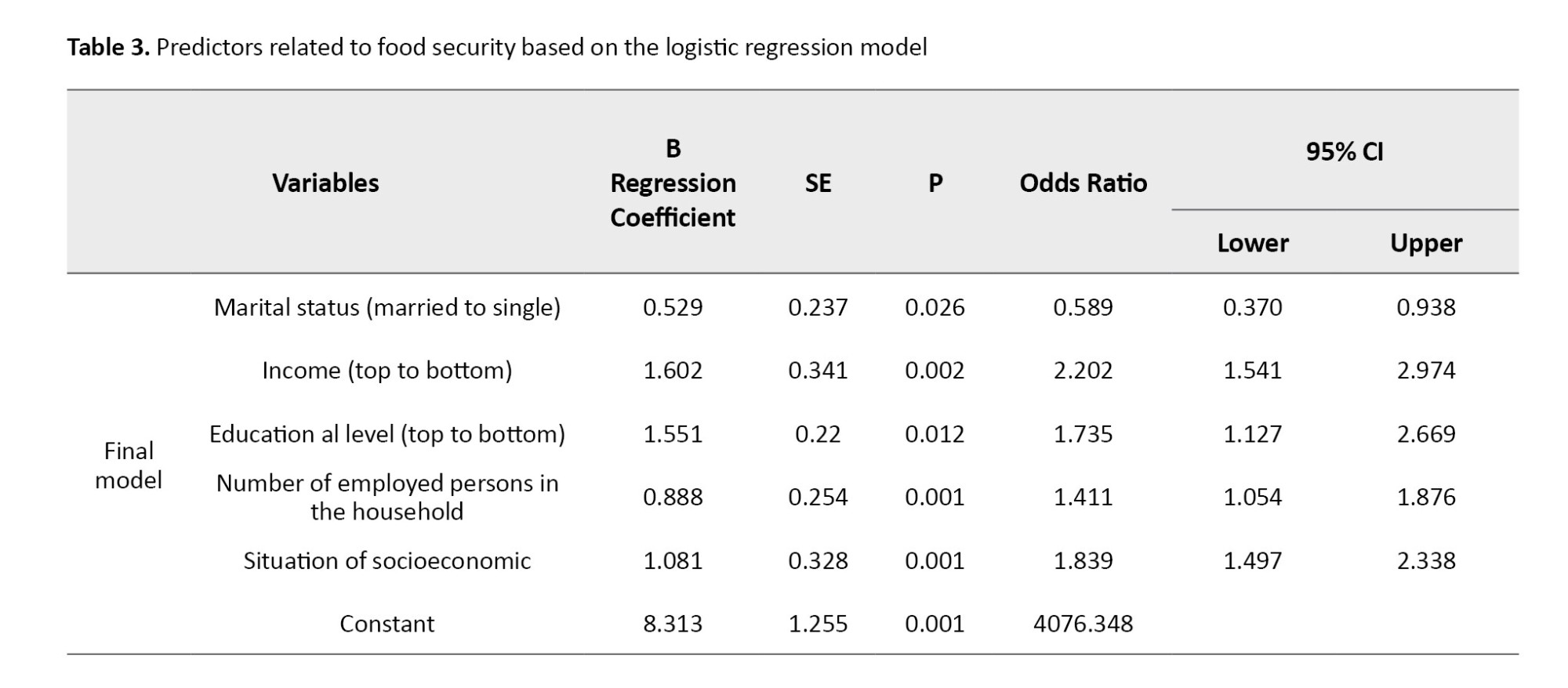
The results indicate that, at a 95% Confidence Level (CI), the relationships between food security and job status, marital status, living with others, income, education, the number of family employees, and the number of people living together are statistically significant. However, the relationship between food insecurity and gender, underlying disease, and number of children is not significant. A significant relationship exists between SES and an individual’s food security (P=0.01). The mean food insecurity index is 14.37±5.123. At a 95% confidence level, the relationship between food security and situation of socioeconomic (OR=1.839, 95% CI, 1.497, 2.338, P=0.001), marital status (OR=0.589, 95% CI, 370,0.938, P=0.001), income (OR=2.202, 95% CI, 1.541, 2.974, P=0.001), education (OR=1.735, 95% CI, 1.127, 2.669, P=0.001), the number of family workers(OR=1.411, 95% CI, 1.054, 1.876, P=0.001) were significant.
Discussion
This study aimed to determine the relationship between food insecurity and its socioeconomic factors in older patients referred to comprehensive health centers in East Guilan.
In a study, those hospitalized were mostly 75 years of age or older and widowed. Those who were hospitalized were more likely to have a lower education level or lower income than those who were not hospitalized [22], which aligns with our results. However, in the other study, no significant differences were observed between the two groups in terms of age, sex, or marital status. There was also no significant difference between the two groups in terms of household size and number of employed persons [23]. In another study, it was shown that people with older age, more children, lower income, and a life without a spouse (living alone or with children) had poorer nutritional status [24]. However, in the Seivwright et al. study, despite low income being the strongest and most consistent predictor of food insecurity in previous studies, the study found no significant differences in food insecurity between people of different genders, cultural identity, education level, household composition, labor force participation status, and income source which is incoherent with the results of the present study [25].
The present study was in line with Placzek’s study, which showed that socioeconomic and demographic factors play an important role in shaping the (unhealthy) diet. Households with higher income and education levels typically consume less unhealthy food and more healthy food. Higher education levels increase the likelihood that people will be more aware of diet and nutrition, as well as how to prepare and cook food [26]. Additionally, other studies [27-29] have shown that SES is associated with food insecurity, which is consistent with the results of the present study. Bayat et al. found that 44.1% of the participants were food insecure, while 55.9% had high food security [30].
The study reveals high levels of food insecurity among older individuals with low SES, and significant positive associations are found with job status, living with others, income, education, the number of employed family members, and the number of people living together. Considering that nearly half of the study’s sample suffered from severe food insecurity, it is also necessary to pay attention to this problem in this segment of the vulnerable population due to various factors significantly related to this issue. To reduce the food insecurity of older adults, policies covering this age group with age-appropriate food baskets and improving their mental health should be considered.
Several factors limited the present study. First, the economic situation could not be accurately calculated and was judged based on the opinions of the samples. Second, the main variable was assessed using a questionnaire, and all the limitations resulting from this data collection method are also present in our study. Notably, the older participants were asked about the past month, which may have resulted in a recall bias due to their specific recall conditions.
It is recommended that the relationship between food security and SES be examined in various regions and cities of Iran, as well as across different populations, and that the results from these regions and populations be compared. Further studies should be conducted across various age groups, and other food security and SES questionnaires should be utilized in future studies.
This study reveals that food insecurity is prevalent among older individuals with low SES. A significant positive relationship is found between food insecurity and employment status, living with others, income, education, the number of employed family members, and the number of people living together. Considering that nearly half of the older individuals studied suffered from severe food insecurity, and also considering various factors that had a significant relationship with this problem in this study, the need to address this issue in this vulnerable population of society has become more urgent than ever. To reduce food insecurity among older adults, policies should be considered to provide them with food baskets tailored to their age and improve their mental health.
Ethical Considerations
Compliance with ethical guidelines
The study was approved by the Ethics Committee of Guilan University of Medical Sciences, Rasht Iran (Code: IR.GUMS.REC.1401.414). All ethical principles of research were observed in this article. At each stage of the study, research units could refuse to continue collaborating if they were unwilling to do so. Informed consent was obtained from all participants. They were also reminded that, if desired, the results of the investigation will be made available to them, and their information will be kept confidential.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Data collection: Marziye Shabani; Data analysis: Zahra Atrkar Roshan; Draft preparation: Marziye Shabani, Parand Pourghane, and Marjan Mahdavi Roshan; Supervision: Parand Pourghane; Final approval: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The researchers would like to thank and express their gratitude to all participants in the present study.
References
The increase in the older population in countries is associated with greater vulnerability and disability. These negative health consequences have a direct impact on access to sufficient food and food insecurity. The older the head of household, the lower the likelihood of food security in the family [1, 2]. Experimental evidence shows that the prevalence of food insecurity among older people is very high due to physical limitations, poor heart conditions, social isolation, and lack of means of transport [3].
Food security is defined as a situation in which all people have access to adequate, safe, and nutritious food at all times to maintain a healthy and active life [4]. Food insecurity, on the other hand, exists when individuals lack full social, economic, and physical access to adequate and healthy food at all times, thereby failing to meet their nutritional needs for a healthy and active life [5]. Household food insecurity, which occurs when a person or family lacks access to food due to financial or other constraints, is a growing public health problem in most developed countries, especially in cases where there is inequality in food sharing [6].
Food insecurity affects more than 820 million people worldwide [7]. The results of recent research in Iran have shown that 73% of urban households experience food security, while 27% face food insecurity [8]. Food insecurity is a major risk factor for malnutrition and has negative consequences for the health of the population [9, 10].
Meanwhile, nutritional poverty in older adults who sometimes have poor dietary patterns is associated with a higher risk of malnutrition, weakness, worsening health conditions, disability, adverse effects on their quality of life and health, and functional impairments. Lack of home, isolation, gender, financial vulnerability, and poor health statistically have significant associations with food insecurity [11].
Population aging is a global challenge for the social and economic development of the world. With advances in the health system, the overall population and, consequently, the older population worldwide have increased, particularly in the 21st century, thereby increasing the need to address this issue [12, 13]. It is estimated that over the next 30 years, the older population will comprise approximately 20% of the world’s population, resulting in a total of two billion older individuals by 2050, meaning that for every five people in the world, one will be aged 65 or older [14].
Additionally, Iran, as a developing country, is also rapidly aging due to changes in various health policies over the past few decades [15]. According to the 2016 census of the Iranian Statistics Center, the total older population of the country is estimated to be 7,414,091 people, and the number of older people in Guilan (the oldest province in the country) is 335,313 (163,438 men and 171,875 women) [16].
Considering the older population of Guilan Province in Iran, this study aimed to investigate food insecurity and socioeconomic factors affecting it among older people visiting comprehensive health centers in the east of Guilan.
Materials and Methods
The study sample for this cross-sectional analytical study consisted of 245 older individuals attending comprehensive health centers in East Guilan. The study sample size was determined based on the results of a similar study [2], which found that 43% of its samples experienced food insecurity (p=0.43, d=0.06, α=0.05). The sampling method employed a multi-stage cluster design. Six clusters were selected from the comprehensive health centers in East Guilan, located in 6 cities (Langerud, Lahijan, Astana, Rudsar, Siahkal, and Amlash). Then one center was randomly selected from each city. Then, the seniors in question were chosen systematically at random at each center.
The inclusion criteria were as follows: 60 years and older, willingness to participate in the study, having health records in comprehensive urban health service centers ability to answer questionnaires through interviews, score above 7 in the Abbreviated Mental Test (AMT) cognitive status test, and completion of the questionnaire.
The research tools included the demographic profile questionnaire, the Household Food Insecurity Access Score (HFIAS), the food security questionnaire, and the Socioeconomic Status (SES) questionnaire. Qualified samples were first assessed with the AMT instrument and entered into the study if they had normal cognitive status. AMT is a cognitive test, originally presented by Hodkinson. This test consisted of 10 questions assessing distant memory, close memory, attention, and orientation. The correct answer to each question scores 1, and an overall score lower than 7 indicates cognitive impairment [17]. The reliability and validity of the questionnaire in Iran were determined by Bakhtiari et al. in older adults [18].
The HFIAS food insecurity questionnaire (in terms of access) consists of 9 questions about the occurrence of food insecurity, followed by recurrence, ranked by severity of food insecurity (in terms of access). For each question (phrase), 4 response options are considered about the number of times the situation has been experienced, including asking how many times (0=never, 1=rarely [once or twice], 2=sometimes [three to ten times], 3=often [more than ten times] during the one-month time frame (30 days ago). In assessing food insecurity (in terms of accessibility) in the community, the data from this questionnaire can be used both quantitatively and qualitatively to evaluate food insecurity in the studied community. The HFIAS score is a continuous measure of an older person’s food insecurity over the past month, derived from a total of occurrence codes answered by the older for 9 questions. The lowest score is 0, and the highest score is 27. The higher the elder’s score, the more food insecurity they experienced. The household food insecurity access prevalence qualitative measure is also used to report the frequency of food insecurity (in terms of access) among older and regional decision-makers. This criterion divides the older population into 4 groups based on insecurity: Food-safe (0-1 points), food-insecure, including mild (2-7 points), moderate (8-14 points), and severe (15-27 points). The higher the number of positive responses of the older to the questions or the more frequently they experienced insecure situations, the more likely they were to be classified as insecure [19].
The SES questionnaire of powerhouse, which comprises four components: Income level, economic class, education, and housing status, along with a total of six demographic questions and five main questions. The measurement comparison of the questions in this questionnaire has five options, and the scoring method is in order from very low (1) to very high (5). Eslami et al. confirmed the validity and internal consistency of this questionnaire [20]. A researcher-made questionnaire, based on similar studies, was used to determine economic and social status [20, 21].
Data collection in this study began with the use of the AMT test in the first step to assess cognitive status. If there was no cognitive impairment, the subjects were included in the study. Following this, demographic characteristics (such as age, gender, marital status, education, occupation, and income), the HFIAS food security questionnaire, and the SES questionnaire were completed.
For statistical analysis, descriptive statistics were employed, and descriptive indicators such as Mean±SD, and univariate chi-square tests were utilized. The simultaneous effect of independent variables on severe food insecurity was shown through multiple logistic regression. Data analysis was performed using SPSS software, version 16.
Results
Two hundred forty-five older people, all of whom had an AMT score greater than 7, were included in the study. The sample consisted of 50.6% males and 49.4% females. The mean age of the samples was 67.66±6.059 years, and all were residents of the town. The occupational status of most people was as follows: 42.4% of households, 82% lived with their spouses, 81.2% were married, 50.6% had incomes above 315 USD, and 30.6% had a level of education below a diploma. About 61.2% had an underlying disease; most of them, 25.7%, had four children. In most households, 53.1% had at least one employed family member, and 34.3% had three or more people living together. Table 1 provides demographic information.
Table 2 shows that, in terms of SES, 74% of individuals with a very low SES experience severe food insecurity, while only 3.4% of those with a high or very high SES experience food insecurity. In terms of food security, 0.4% had complete food security, 11.8% had mild insecurity, 43.7% had moderate food insecurity, and 44.1% also had severe food insecurity.
For statistical analysis, descriptive statistics and descriptive indicators, such as Mean±SD, ratio, and univariate chi-square tests, will be used to illustrate the simultaneous effect of independent variables on severe food insecurity through multiple logistic regression (Table 3).
The results indicate that, at a 95% Confidence Level (CI), the relationships between food security and job status, marital status, living with others, income, education, the number of family employees, and the number of people living together are statistically significant. However, the relationship between food insecurity and gender, underlying disease, and number of children is not significant. A significant relationship exists between SES and an individual’s food security (P=0.01). The mean food insecurity index is 14.37±5.123. At a 95% confidence level, the relationship between food security and situation of socioeconomic (OR=1.839, 95% CI, 1.497, 2.338, P=0.001), marital status (OR=0.589, 95% CI, 370,0.938, P=0.001), income (OR=2.202, 95% CI, 1.541, 2.974, P=0.001), education (OR=1.735, 95% CI, 1.127, 2.669, P=0.001), the number of family workers(OR=1.411, 95% CI, 1.054, 1.876, P=0.001) were significant.
Discussion
This study aimed to determine the relationship between food insecurity and its socioeconomic factors in older patients referred to comprehensive health centers in East Guilan.
In a study, those hospitalized were mostly 75 years of age or older and widowed. Those who were hospitalized were more likely to have a lower education level or lower income than those who were not hospitalized [22], which aligns with our results. However, in the other study, no significant differences were observed between the two groups in terms of age, sex, or marital status. There was also no significant difference between the two groups in terms of household size and number of employed persons [23]. In another study, it was shown that people with older age, more children, lower income, and a life without a spouse (living alone or with children) had poorer nutritional status [24]. However, in the Seivwright et al. study, despite low income being the strongest and most consistent predictor of food insecurity in previous studies, the study found no significant differences in food insecurity between people of different genders, cultural identity, education level, household composition, labor force participation status, and income source which is incoherent with the results of the present study [25].
The present study was in line with Placzek’s study, which showed that socioeconomic and demographic factors play an important role in shaping the (unhealthy) diet. Households with higher income and education levels typically consume less unhealthy food and more healthy food. Higher education levels increase the likelihood that people will be more aware of diet and nutrition, as well as how to prepare and cook food [26]. Additionally, other studies [27-29] have shown that SES is associated with food insecurity, which is consistent with the results of the present study. Bayat et al. found that 44.1% of the participants were food insecure, while 55.9% had high food security [30].
The study reveals high levels of food insecurity among older individuals with low SES, and significant positive associations are found with job status, living with others, income, education, the number of employed family members, and the number of people living together. Considering that nearly half of the study’s sample suffered from severe food insecurity, it is also necessary to pay attention to this problem in this segment of the vulnerable population due to various factors significantly related to this issue. To reduce the food insecurity of older adults, policies covering this age group with age-appropriate food baskets and improving their mental health should be considered.
Several factors limited the present study. First, the economic situation could not be accurately calculated and was judged based on the opinions of the samples. Second, the main variable was assessed using a questionnaire, and all the limitations resulting from this data collection method are also present in our study. Notably, the older participants were asked about the past month, which may have resulted in a recall bias due to their specific recall conditions.
It is recommended that the relationship between food security and SES be examined in various regions and cities of Iran, as well as across different populations, and that the results from these regions and populations be compared. Further studies should be conducted across various age groups, and other food security and SES questionnaires should be utilized in future studies.
This study reveals that food insecurity is prevalent among older individuals with low SES. A significant positive relationship is found between food insecurity and employment status, living with others, income, education, the number of employed family members, and the number of people living together. Considering that nearly half of the older individuals studied suffered from severe food insecurity, and also considering various factors that had a significant relationship with this problem in this study, the need to address this issue in this vulnerable population of society has become more urgent than ever. To reduce food insecurity among older adults, policies should be considered to provide them with food baskets tailored to their age and improve their mental health.
Ethical Considerations
Compliance with ethical guidelines
The study was approved by the Ethics Committee of Guilan University of Medical Sciences, Rasht Iran (Code: IR.GUMS.REC.1401.414). All ethical principles of research were observed in this article. At each stage of the study, research units could refuse to continue collaborating if they were unwilling to do so. Informed consent was obtained from all participants. They were also reminded that, if desired, the results of the investigation will be made available to them, and their information will be kept confidential.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Data collection: Marziye Shabani; Data analysis: Zahra Atrkar Roshan; Draft preparation: Marziye Shabani, Parand Pourghane, and Marjan Mahdavi Roshan; Supervision: Parand Pourghane; Final approval: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The researchers would like to thank and express their gratitude to all participants in the present study.
References
- Fernandes, S. G., Rodrigues, A. M., Nunes, C., Santos, O., Gregório, M. J., & de Sousa, R. D., et al. (2018). Food Insecurity in Older Adults: Results from the epidemiology of chronic diseases cohort study 3. Frontiers in Medicine, 5, 203. [DOI:10.3389/fmed.2018.00203] [PMID]
- Shakiba M, Salari A, Mahdavi-Roshan M. Food insecurity status and associated factors among rural households in the north of Iran. Nutr Health. 2021; 27(3):301-7. [DOI:10.1177/0260106021996840] [PMID]
- Saenz JL, Kessler J, Nelson E. Food insecurity across the life-course and cognitive function among older Mexican Adults. Nutrients. 2022; 14(7):1462. [DOI:10.3390/nu14071462] [PMID]
- Dasgupta P, Bhattacherjee S, Das DK. Food security in households of people living with human immunodeficiency virus/acquired immunodeficiency syndrome: A cross-sectional study in a subdivision of Darjeeling District, West Bengal. J Prev Med Public Health. 2016; 49(4):240-8. [DOI:10.3961/jpmph.16.023] [PMID]
- Pak TY, Kim G. Food stamps, food insecurity, and health outcomes among elderly Americans. Prev Med. 2020; 130:105871.[DOI:10.1016/j.ypmed.2019.105871] [PMID]
- Pollard CM, Booth S. Food insecurity and hunger in rich countries-it is time for action against inequality. Int J Environ Res Public Health. 2019; 16(10):1804. [DOI:10.3390/ijerph16101804] [PMID]
- Akbari M, Pishbahar E, Dashti G. [Investigation of factors influencing food insecurity in Iranian families using generalized ordered logit model (Persian)]. Agric Econ Dev. 2021; 29(2):109-35. [DOI:10.30490/aead.2021.341962.1201]
- Grimaccia E, Naccarato A. Food insecurity in Europe: A gender perspective. Soc Indic Res. 2022; 161(2-3):649-67. [DOI:10.1007/s11205-020-02387-8] [PMID]
- De Araujo ML, de Deus Mendonça R, Lopes Filho JD, Lopes ACS. Association between food insecurity and food intake. Nutrition. 2018; 54:54-9. [DOI:10.1016/j.nut.2018.02.023]
- Lepore MJ, Rochford H. Addressing food insecurity and malnourishment among older adults: the critical role of Older Americans Act Nutrition Programs. Public Policy Aging Rep. 2019; 29(2):56-61. [DOI:10.1093/ppar/prz003]
- Vilar-Compte M, Martínez-Martínez O, Orta-Alemán D, Perez-Escamilla R. Functional limitations, depression, and cash assistance are associated with food insecurity among older urban adults in Mexico City. J Health Care Poor Underserved. 2016; 27(3):1537-54. [DOI:10.1353/hpu.2016.0130] [PMID]
- Bai Y, Bian F, Zhang L, Cao Y. The impact of social support on the health of the rural elderly in China. Int J Environ Res Public Health. 2020; 17(6):2004. [PMID]
- Deshpande SK, Hasegawa RB, Weiss J, Small DS. The association between adolescent football participation and early adulthood depression. PLoS One. 2020; 15(3):e0229978. [PMID]
- Kannus P, Niemi S, Sievänen H, Parkkari J. Declining incidence in fall-induced deaths of older adults: Finnish statistics during 1971-2015. Aging Clin Exp Res. 2018; 30(9):1111-5.[DOI:10.1007/s40520-018-0898-9] [PMID]
- Iranmanesh R, Dasht Bozorgi Z. [The effect of health-oriented lifestyle training on psychological well-being, blood pressure and death anxiety of elderly women (Persian)]. Aging Psychol. 2019; 4(4):263-73. [Link]
- Statistical Centre of Iran. [Selected findings of national population and housing census 2016 (Persian)]. Tehran: Statistical Centre of Iran; 2017. [Link]
- Hodkinson HM. Evaluation of a mental test score for assessment of mental impairment in the elderly. Age Ageing. 1972 ; 1(4):233-8.[DOI:10.1093/ageing/1.4.233] [PMID]
- Bakhtiari F, Foroughan M, Fakhrzadeh H, Nazari N, Najafi B, Alizadeh M, et al. [Validation of the Persian version of Abbreviated Mental Test (AMT) in elderly residents of Kahrizak charity foundation (Persian)]. Iran J Diabetes Metab. 2014;13(6):487-94. [Link]
- Pakravan-Charvadeh MR, Khan HA, Flora C. Spatial analysis of food security in Iran: Associated factors and governmental support policies. J Public Health Policy. 2020; 41(3):351-74. [DOI:10.1057/s41271-020-00221-6] [PMID]
- Eslami A, Mahmoudi A, Khabiri M, Najafiyan Razavi SM. [The role of socioeconomic conditions in the citizens’ motivation for participating in public sports (Persian)]. Appl Res Sport Manage. 2014; 2(3):89-104. [Link]
- Ghodratnama A, Heidarinejad S, Davoodi I. [The relationship between socio - economic status and the rate of physical activity in Shahid Chamran University Students of Ahwaz (Persian)]. Sport Manage J. 2013; 5(16):5-20. [DOI:10.22059/jsm.2013.30410]
- Bergmans RS, Mezuk B, Zivin K. Food insecurity and geriatric hospitalization. Int J Environ Res Public Health. 2019; 16(13):2294. [DOI:10.3390/ijerph16132294] [PMID]
- Janzadeh H, Mozaffari-Khosravi H, Javadi M. The association of food insecurity, inflammation, and several socioeconomic factors with type 2 diabetes: A case-control study. J Nutr Food Secur. 2020; 5(1):38-46. [DOI:10.18502/jnfs.v5i1.2317]
- Bakhtiari A, Pourali M, Omidvar S. Nutrition assessment and geriatric associated conditions among community dwelling Iranian elderly people. BMC Geriatr. 2020; 20(1):278. [DOI:10.1186/s12877-020-01668-8] [PMID]
- Seivwright AN, Callis Z, Flatau P. Food insecurity and socioeconomic disadvantage in Australia. Int J Environ Res Public Health. 2020; 17(2):559. [DOI:10.3390/ijerph17020559] [PMID]
- Placzek O. Socio-economic and demographic aspects of food security and nutrition. OECD Food, Agriculture and Fisheries Papers. 2021; 150:1-43. [DOI:10.1787/49d7059f-en]
- Chakraborty S, Banerjee S, Saha I. Prevalence and determinants of geriatric malnutrition among rural populations: A Community based cross-sectional Study in Eastern India. Soc Determ Health. 2020; 6:e30-e. [DOI:10.22037/sdh.v6i1.33892]
- Robbins R, Porter Starr KN, Addison O, Parker EA, Wherry SJ, Ikpe S, et al. Prevalence and socio-economic determinates of food insecurity in Veterans: Findings from National Health and Nutrition Examination Survey. Public Health Nutr. 2023; 26(7):1478-87.[DOI:10.1017/S1368980023000538] [PMID]
- Ogunniyi AI, Omotoso SO, Salman KK, Omotayo AO, Olagunju KO, Aremu AO. Socio-economic drivers of food security among rural households in Nigeria: Evidence from smallholder maize farmers. Social Indicators Research. 2021; 155:583-99. [DOI:10.1007/s11205-020-02590-7]
- Bayat B, Izadi A, Askari G, Piran F, Zolfaghai H. Food insecurity and depressive symptoms among university students: A cross-sectional study from Iran. J Nutr Food Secur. 2021. [DOI:10.18502/jnfs.v6i1.5295]
Article Type : Research |
Subject:
Special
Received: 2024/08/8 | Accepted: 2025/02/23 | Published: 2025/06/10
Received: 2024/08/8 | Accepted: 2025/02/23 | Published: 2025/06/10
Send email to the article author
| Rights and permissions | |
 | This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
