Fri, Jul 12, 2024
Volume 34, Issue 3 (6-2024)
JHNM 2024, 34(3): 262-269 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Mazloum H, Razaghi N, Behnam Vashani H, Pourbadakhshan N. Effect of Animation Display of Urinary Catheterization on the Anxiety of Mothers With Hospitalized Children: A Quasi-experimental Study. JHNM 2024; 34 (3) :262-269
URL: http://hnmj.gums.ac.ir/article-1-2375-en.html
URL: http://hnmj.gums.ac.ir/article-1-2375-en.html



1- MSc in Nursing, Research Committee, School of Nursing and Midwifery, Mashhad University of Medical Sciences, Mashhad, Iran.
2- Assistant Professor, Department of Pediatric Nursing, Nursing and Midwifery Care Research Center, Mashhad University of Medical Sciences, Mashhad, Iran. ,Razaghin@mums.ac.ir
3- Instructor, Department of Pediatric Nursing, Nursing and Midwifery Care Research Center, Mashhad University of Medical Sciences, Mashhad, Iran.
4- Assistant Professor, Department of Pediatric, Faculty of Medicine, Mashhad University of Medical Sciences, Mashhad, Iran.
2- Assistant Professor, Department of Pediatric Nursing, Nursing and Midwifery Care Research Center, Mashhad University of Medical Sciences, Mashhad, Iran. ,
3- Instructor, Department of Pediatric Nursing, Nursing and Midwifery Care Research Center, Mashhad University of Medical Sciences, Mashhad, Iran.
4- Assistant Professor, Department of Pediatric, Faculty of Medicine, Mashhad University of Medical Sciences, Mashhad, Iran.
Full-Text [PDF 564 kb]
(31 Downloads)
| Abstract (HTML) (109 Views)
Full-Text: (16 Views)
Introduction
Urinary catheterization is a common and, at the same time, an uncomfortable procedure for hospitalized children. It is used to drain urine or inject an x-ray solution to study the anatomy or function of the urinary system [1]. Common diagnostic methods (such as urinalysis and urine culture) to test urinary tract infections in children require a urine sample, usually obtained in younger children by urethral catheterization or suprapubic aspiration. These invasive and potentially painful methods may be uncomfortable for parents and children; nonetheless, they are more popular than non-invasive options, such as urine collection bags [2]. Catheterization is a painful and traumatic experience for most children, and the avoidance of urinary catheterization may affect the desired clinical management [3].
Some parents are deeply worried about their child’s experiences of having painful procedures and do not approve of these operations [4]. The performance of invasive methods, such as urinary catheterization, in children is usually a source of emotional distress for their parents, bringing them a considerable amount of stress and anxiety [5]. Parents’ anxiety is often associated with the severity of their children’s illness and treatment methods and is more frequently observed during treatment procedures [6]. They always complain about the incomplete information provided by the medical staff about their child’s condition and treatment [7]. Parents must be informed of diagnostic and treatment options to make wise choices about their child’s care. The key components of family-centered care include parental involvement in care decisions, incorporating their knowledge and preferences into the treatment plan, and communicating diagnostic and treatment information in understandable language [2].
Today, we are witnessing a rise in the use of technology to increase the quality of medical services [8]. Medical animation videos can increase the quality of medical services in different sectors [9]. Paton et al. demonstrated that multimedia education significantly reduced parents’ anxiety during the informed consent process before surgery. This method improves the knowledge and awareness of parents; moreover, it reduces anxiety and may improve parents’ long-term understanding and satisfaction in the healthcare process [10].
Cohen et al. examined short video interventions for parents of children undergoing vaccination. The results of the stated study pointed to a significant improvement in parents’ behavior [11]. Based on the Brown et al. study, there is insufficient research on parents’ anxiety, which is an essential aspect of designing interventions [12]. Currently, in pediatric departments in hospitals, urinary catheterization typically provokes anxiety in children’s parents, and they wonder whether the catheterization will cause harm to their children or not.
Despite the usual explanations doctors and nurses provide about this procedure, sometimes, parents do not consent to insert a urinary catheter. Therefore, it is necessary to use appropriate interventions based on modern educational methods to reduce the anxiety of parents of hospitalized children [10]. To the best of our knowledge, few studies have been conducted on this matter; therefore, the present study aimed to assess the effect of the display animation of urinary catheterization on the anxiety of mothers with hospitalized children in Mashhad City, Iran.
Materials and Methods
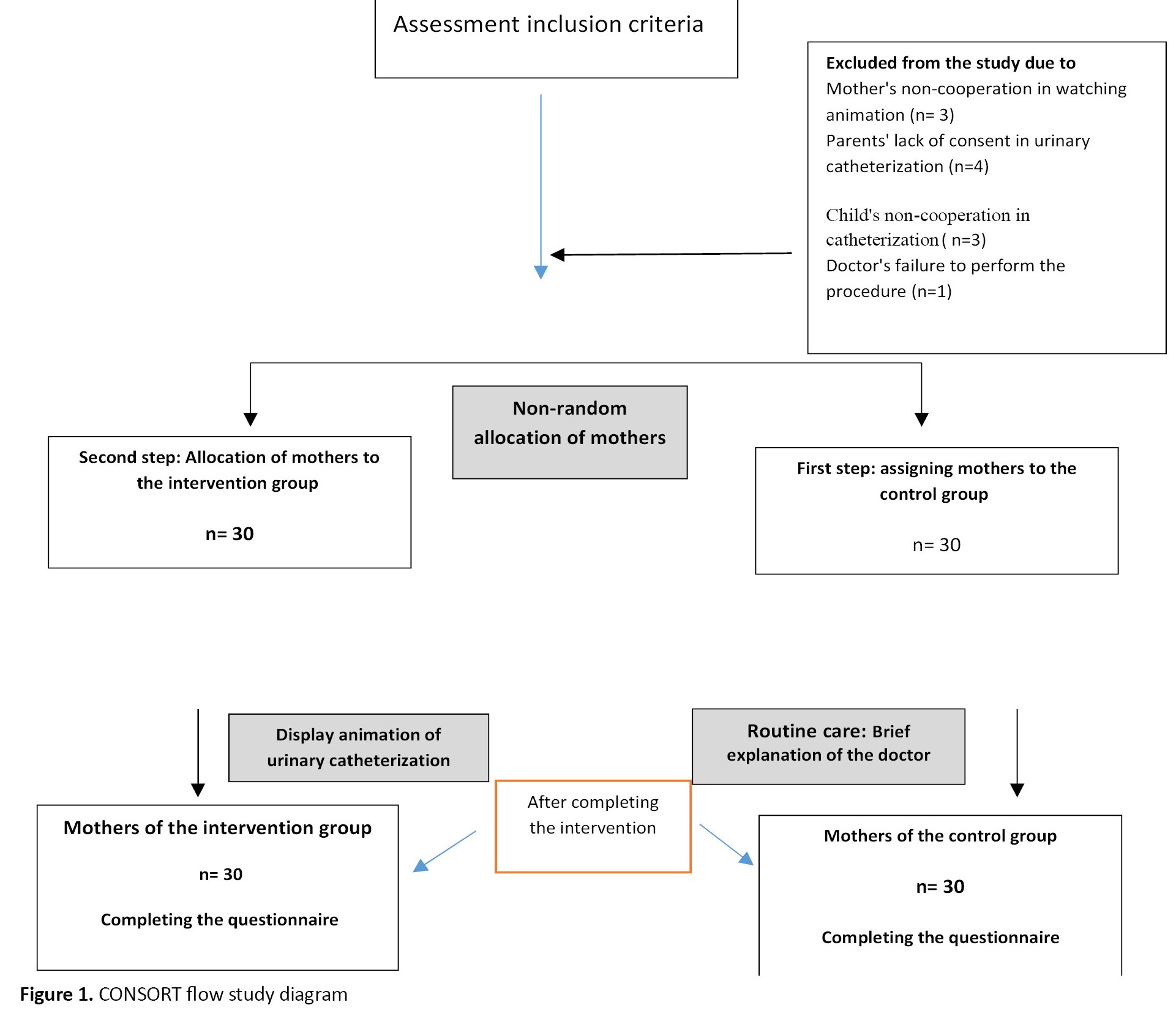
This quasi-experimental study with an intervention and control group was conducted on 60 mothers of hospitalized children aged 1 month to 12 years in the emergency wards of one of the children’s teaching hospitals affiliated with Mashhad University of Medical Sciences between February 2022 and September 2022. A total of 72 mothers were included in the research and allocated to intervention and control groups (n=36 in each group). Among these, 7 samples from the intervention group and 5 from the control group were excluded from the study for reasons mentioned in Figure 1.
 Finally, 30 mothers were included in the study in each group.
Finally, 30 mothers were included in the study in each group.
The “comparison of two independent population means” formula was used to determine the sample size. Since no exact similar research regarding intervention and dependent variables was found, the sample size was estimated based on the parameters obtained in the pilot study. The sample size was determined considering a significant level of 0.05 and test power (B=0.20) of 80%, and the Mean±SD anxiety of 10 mothers from the control and intervention groups were 14.33±6.24 and 5.88±4.62. Finally, 60 children and their mothers (30 in each group) entered the study.
Children and mothers were included in the study if they met the inclusion criteria. The inclusion criteria included a physician’s prescription to insert a urinary catheter for the child, no previous experience with urinary catheterization, mothers’ willingness and consent to participate in the study, no prior training on how to perform urinary catheterization, mother’s reading and writing literacy, and the presence of mothers in the treatment process. The exclusion criteria at the beginning of the study were the presence of any known mental disorders in the mother (such as depression and attention disorder, bipolar disorder by self-expression) and major anomaly in the child (immune deficiency, other digestive abnormality, metabolic disease, heart disease based on medical records). The exclusion criteria during the study were withdrawal from the study, occurrence of any emergency condition during catheter insertion, or urinary retention.
The research instruments included a demographic characteristics form, an informed consent form to participate, and Spielberger state-trait anxiety inventory (STAI). Demographic characteristics form included questions about age, sex, employment status, mother’s education, and economic situation. The STAI includes 40 self-reporting questions, from which the first 20 are state questions measuring state anxiety. The subjects must express their feelings at the present moment when the researcher fills out the form. The items are rated on a 4-point Likert scale, ranging from 1 to 4. A score of 4 correlates with greater anxiety and 10 scales of state anxiety are scored accordingly. A higher score indicates no anxiety for scoring other items (10 items on state anxiety). The scores range from 20 to 80 (20-40=mild anxiety, 41-60=moderate anxiety, and 61-80=severe anxiety) [13]. Mahram translated the questionnaire into Persian and examined its reliability and validity; we used this Persian version of the tool [14]. In the present study, the internal consistency was measured by the Cronbach α coefficient, which was equal to 0.89.
This research consisted of two stages: In the first stage, animation videos on inserting a urinary catheter were prepared separately for male and female children. This 5-minute animation video included images, sound, text, and relaxing music. Moreover, the reasons for catheterization, the complications caused by avoiding catheterization, as well as the disadvantages and advantages of catheterization were referred to in the videos. These videos were prepared with the help of animation experts at the Ferdowsi University of Mashhad. They were used after approval by the Faculty of Nursing and Midwifery professors of Mashhad University of Medical Sciences. The animation content was prepared based on the latest valid references [15, 16] and with the approval of expert professors, including a pediatrician and two members of the Pediatric Nursing Faculty. In preparing this educational animation, such standards as setting educational goals, content simplicity, short but comprehensive sentences, and removing unnecessary or specialized sentences were considered.
While communicating with the mothers of children hospitalized in the emergency room, the researcher obtained their written consent to participate in the research. The samples received oral explanations about the goals and research method for 15 minutes. Demographic characteristics form, and STAI were completed for mothers of hospitalized children in the control and intervention groups before the intervention.
To prevent the exchange of information between mothers, after the draw, the control group and the intervention group were first entered into the study. In the control group, mothers of hospitalized children were given general explanations about the method used by the doctor or nurse at the patient’s bedside before performing urinary catheterization. In the intervention group, mothers watched the animation video about this procedure before catheterization via the researcher’s laptop in the hospital’s conference room. Animation videos were prepared separately for male and female children and lasted 5 minutes. They were displayed to mothers according to the gender of their children. After the intervention, STAI was completed for mothers of hospitalized children in both control and intervention groups.
After entering data in SPSS software version 23, data were analyzed using descriptive (frequency, Mean±SD) and inferential (the independent t-test, the chi-square test) statistics to compare between-group and within-group mean differences. Also, the Kolmogorov–Smirnov test assessed the normality of data distribution. The level of significance of statistical tests was considered P<0.05.
Results
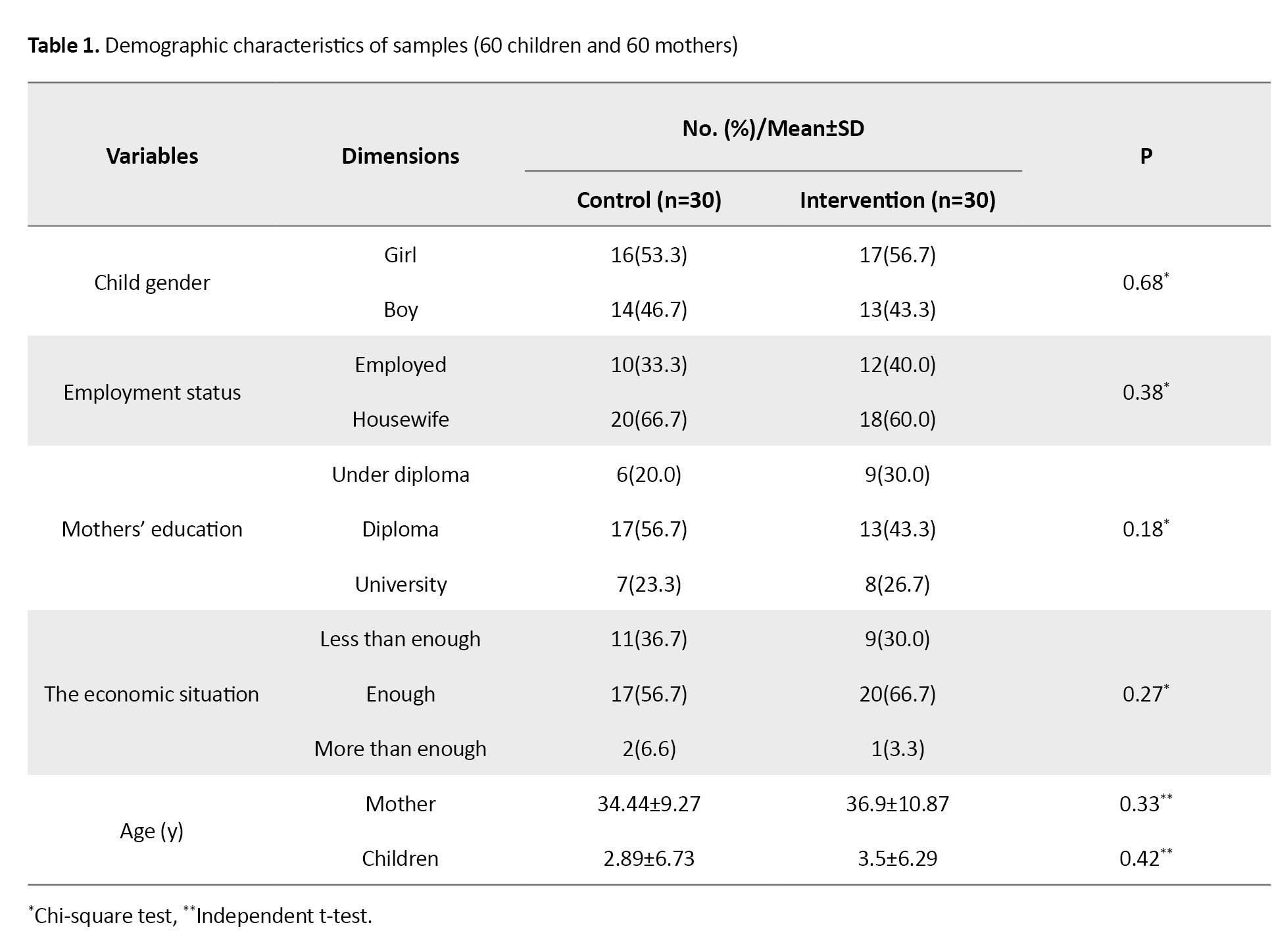
The Mean±SD ages of mothers in the intervention and control groups were 36.9±10.87 and 34.44±9.27 years, respectively. The Mean±SD ages of children in the intervention and control groups were 3.5±6.29 and 2.89±6.73 years, respectively. Other demographic data of mothers and children are presented in Table 1.
The Kolmogorov-Smirnov test was used to assess the distribution of quantitative variables. The test results indicated that all quantitative demographic and intervening variables in this research had a normal distribution.
The result of the independent t-test revealed no statistically significant difference between the two groups in terms of the mean age of hospitalized children and their mothers. Moreover, the chi-square test result found no significant difference between the two groups of mothers in terms of their children’s gender and their level of education. Therefore, the two groups of mothers of the studied children were homogeneous regarding these variables.
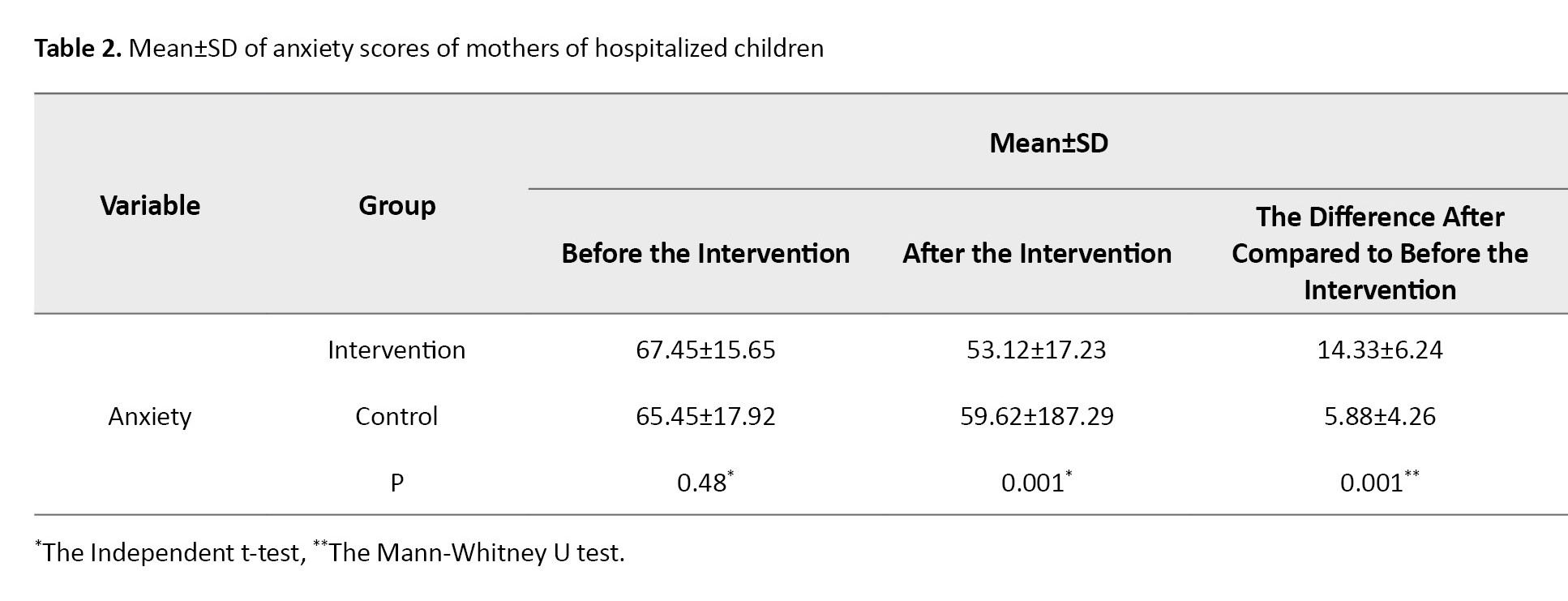
The independent t-test within the group illustrated that in the stage before watching the animation video, the mean anxiety score of the mothers of hospitalized children in the two groups did not significantly differ (P=0.480), and the two groups were homogeneous regarding this variable. Nonetheless, the independent t-test results indicated a significant difference between the two groups after displaying the animation video (P=0.001). In the intervention group, the mean anxiety score decreased from 65.45±5.65 to 53.12±17.23 (Table 2).
Discussion
To determine the effect of display animation of urinary catheterization on the state anxiety of mothers with hospitalized children, the results demonstrated a significant decrease in their anxiety after the intervention. Moreover, a more marked reduction occurred in state anxiety scores after the intervention in the intervention group compared to that in the control group. In a literature review, a study similar to the current research was not found; therefore, the researcher tried to use the results of other studies in this section.
The findings of the present study indicate the high levels of anxiety among mothers in the intervention group before the intervention. Therefore, appropriate interventions must be made to alleviate their stress and enhance the informed consent process. The anxiety experienced by mothers before their children undergo invasive procedures can affect the treatment process [6]. Parental anxiety is associated with distress and problematic behaviors in children during and after hospitalization. In addition, unanswered questions and misinformation about invasive procedures can increase parental anxiety [12]. Children and their parents prefer to be informed about surgical intervention, anesthesia, possible pain problems, and other invasive procedures they may undergo during hospitalization [17, 18].
In this regard, according to a study by Paton et al., multimedia education significantly reduced parents’ anxiety during the informed consent process. According to the stated research, this method improves the knowledge and awareness of parents, lowers anxiety, and may improve parents’ long-term understanding and satisfaction in the healthcare process [10]. The results of the present research are consistent with the results of their study; nonetheless, the present study used animation videos to show urinary catheterization to the intervention group to control their anxiety.
The study by Book et al. demonstrated that the display of a 6-minute online video significantly reduced the anxiety of parents of children with inguinal hernia before surgery compared to the control group. Moreover, it enhanced the consent process and increased parental knowledge [19]. The present research results are consistent with the results of their study. The similarity in the research population (parents of children) can justify this consistency. However, it differed from the present study in which the educational animation video was not presented online, and the procedure performed on children differed. In general, the provision of accurate information can be a positive factor in reducing the anxiety of parents before their children undergo any aggressive procedure.
On the other hand, the study by Torres-Lagares et al. reported that watching a video of the removal of an inferior third molar surgery increased patients’ anxiety levels [20]. One of the reasons for this discrepancy is the difference in the content of the educational video, signifying that the educational content plays a key role in the anxiety level of people. In their study, all the surgical steps were shown, which can cause anxiety. It seems the most appropriate is to provide patients with the information they require in an adequate format.
The results of a study titled» parental educational intervention to facilitate informed consent» by Lin et al. showed that educational video-assisted informed consent was superior to the conventional process of obtaining parental consent in the emergency department and reduced anxiety [21]. The results of the present research were consist with their results. This consistency can be ascribed to the use of educational animation videos, although the treatment procedure was different in the study by Lin et al. Modern portable electronic devices, such as smartphones and tablets, as well as access to the Internet, open up new opportunities for information transfer. The good feature of the animation video used in the current study was its small file size and comprehensibility. Therefore, it can be easily accessed by parents through mobile phones. Also, they can be localized and provided in the native language of every country in medical centers. Further research is recommended to assess the effect of these variables. In a meta-analysis study conducted by Feeley et al. on 21 articles published from 2009 to 2020, the findings indicate an overall positive impact of using animation in improving viewers’ learning in various health and clinical fields, including surgery and diabetes [22]. Providing appropriate educational content and allowing parents to decide when and how often to watch the video will reduce their anxiety [23]. It is suggested that the effectiveness of this intervention be tested over other invasive methods, and its effect on anxiety should be investigated.
One of our limitations in this study was that during the COVID-19 pandemic, access to samples was difficult. The individual and cultural differences of the mothers participating in the research were other limitations of the present study, and it is suggested that the effect of this intervention on mothers’ anxiety in other cultures be evaluated as well.
The present study indicates that displaying an animation of urinary catheterization before the procedure reduces mothers’ anxiety levels. It is suggested to use this educational method before urinary catheterization in children, and because it reduces maternal anxiety, it may improve parental satisfaction with the healthcare process.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of Mashhad University of Medical Sciences (IR.MUMS.NURSE.REC.1400.054), receiving the letter of introduction and making necessary coordinating with the officials of this hospital. Written informed consent was obtained from all participants.
Funding
This study was extracted from the Master’s thesis of the Hadi Mazloum, approved by Department of Pediatric Nursing, School of Nursing and Midwifery, Mashhad University of Medical Sciences and was funded by Mashhad University of Medical Sciences (Grant No.: 990783).
Authors' contributions
Data collection: Hadi Mazloum and Nafiseh Pourbadakhshan; Writing the original draft: Naghmeh Razaghi; Study design, methodology, data analysis and final review: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors would like to thank the mothers who participated in this study.
References
Urinary catheterization is a common and, at the same time, an uncomfortable procedure for hospitalized children. It is used to drain urine or inject an x-ray solution to study the anatomy or function of the urinary system [1]. Common diagnostic methods (such as urinalysis and urine culture) to test urinary tract infections in children require a urine sample, usually obtained in younger children by urethral catheterization or suprapubic aspiration. These invasive and potentially painful methods may be uncomfortable for parents and children; nonetheless, they are more popular than non-invasive options, such as urine collection bags [2]. Catheterization is a painful and traumatic experience for most children, and the avoidance of urinary catheterization may affect the desired clinical management [3].
Some parents are deeply worried about their child’s experiences of having painful procedures and do not approve of these operations [4]. The performance of invasive methods, such as urinary catheterization, in children is usually a source of emotional distress for their parents, bringing them a considerable amount of stress and anxiety [5]. Parents’ anxiety is often associated with the severity of their children’s illness and treatment methods and is more frequently observed during treatment procedures [6]. They always complain about the incomplete information provided by the medical staff about their child’s condition and treatment [7]. Parents must be informed of diagnostic and treatment options to make wise choices about their child’s care. The key components of family-centered care include parental involvement in care decisions, incorporating their knowledge and preferences into the treatment plan, and communicating diagnostic and treatment information in understandable language [2].
Today, we are witnessing a rise in the use of technology to increase the quality of medical services [8]. Medical animation videos can increase the quality of medical services in different sectors [9]. Paton et al. demonstrated that multimedia education significantly reduced parents’ anxiety during the informed consent process before surgery. This method improves the knowledge and awareness of parents; moreover, it reduces anxiety and may improve parents’ long-term understanding and satisfaction in the healthcare process [10].
Cohen et al. examined short video interventions for parents of children undergoing vaccination. The results of the stated study pointed to a significant improvement in parents’ behavior [11]. Based on the Brown et al. study, there is insufficient research on parents’ anxiety, which is an essential aspect of designing interventions [12]. Currently, in pediatric departments in hospitals, urinary catheterization typically provokes anxiety in children’s parents, and they wonder whether the catheterization will cause harm to their children or not.
Despite the usual explanations doctors and nurses provide about this procedure, sometimes, parents do not consent to insert a urinary catheter. Therefore, it is necessary to use appropriate interventions based on modern educational methods to reduce the anxiety of parents of hospitalized children [10]. To the best of our knowledge, few studies have been conducted on this matter; therefore, the present study aimed to assess the effect of the display animation of urinary catheterization on the anxiety of mothers with hospitalized children in Mashhad City, Iran.
Materials and Methods
This quasi-experimental study with an intervention and control group was conducted on 60 mothers of hospitalized children aged 1 month to 12 years in the emergency wards of one of the children’s teaching hospitals affiliated with Mashhad University of Medical Sciences between February 2022 and September 2022. A total of 72 mothers were included in the research and allocated to intervention and control groups (n=36 in each group). Among these, 7 samples from the intervention group and 5 from the control group were excluded from the study for reasons mentioned in Figure 1.
The “comparison of two independent population means” formula was used to determine the sample size. Since no exact similar research regarding intervention and dependent variables was found, the sample size was estimated based on the parameters obtained in the pilot study. The sample size was determined considering a significant level of 0.05 and test power (B=0.20) of 80%, and the Mean±SD anxiety of 10 mothers from the control and intervention groups were 14.33±6.24 and 5.88±4.62. Finally, 60 children and their mothers (30 in each group) entered the study.
Children and mothers were included in the study if they met the inclusion criteria. The inclusion criteria included a physician’s prescription to insert a urinary catheter for the child, no previous experience with urinary catheterization, mothers’ willingness and consent to participate in the study, no prior training on how to perform urinary catheterization, mother’s reading and writing literacy, and the presence of mothers in the treatment process. The exclusion criteria at the beginning of the study were the presence of any known mental disorders in the mother (such as depression and attention disorder, bipolar disorder by self-expression) and major anomaly in the child (immune deficiency, other digestive abnormality, metabolic disease, heart disease based on medical records). The exclusion criteria during the study were withdrawal from the study, occurrence of any emergency condition during catheter insertion, or urinary retention.
The research instruments included a demographic characteristics form, an informed consent form to participate, and Spielberger state-trait anxiety inventory (STAI). Demographic characteristics form included questions about age, sex, employment status, mother’s education, and economic situation. The STAI includes 40 self-reporting questions, from which the first 20 are state questions measuring state anxiety. The subjects must express their feelings at the present moment when the researcher fills out the form. The items are rated on a 4-point Likert scale, ranging from 1 to 4. A score of 4 correlates with greater anxiety and 10 scales of state anxiety are scored accordingly. A higher score indicates no anxiety for scoring other items (10 items on state anxiety). The scores range from 20 to 80 (20-40=mild anxiety, 41-60=moderate anxiety, and 61-80=severe anxiety) [13]. Mahram translated the questionnaire into Persian and examined its reliability and validity; we used this Persian version of the tool [14]. In the present study, the internal consistency was measured by the Cronbach α coefficient, which was equal to 0.89.
This research consisted of two stages: In the first stage, animation videos on inserting a urinary catheter were prepared separately for male and female children. This 5-minute animation video included images, sound, text, and relaxing music. Moreover, the reasons for catheterization, the complications caused by avoiding catheterization, as well as the disadvantages and advantages of catheterization were referred to in the videos. These videos were prepared with the help of animation experts at the Ferdowsi University of Mashhad. They were used after approval by the Faculty of Nursing and Midwifery professors of Mashhad University of Medical Sciences. The animation content was prepared based on the latest valid references [15, 16] and with the approval of expert professors, including a pediatrician and two members of the Pediatric Nursing Faculty. In preparing this educational animation, such standards as setting educational goals, content simplicity, short but comprehensive sentences, and removing unnecessary or specialized sentences were considered.
While communicating with the mothers of children hospitalized in the emergency room, the researcher obtained their written consent to participate in the research. The samples received oral explanations about the goals and research method for 15 minutes. Demographic characteristics form, and STAI were completed for mothers of hospitalized children in the control and intervention groups before the intervention.
To prevent the exchange of information between mothers, after the draw, the control group and the intervention group were first entered into the study. In the control group, mothers of hospitalized children were given general explanations about the method used by the doctor or nurse at the patient’s bedside before performing urinary catheterization. In the intervention group, mothers watched the animation video about this procedure before catheterization via the researcher’s laptop in the hospital’s conference room. Animation videos were prepared separately for male and female children and lasted 5 minutes. They were displayed to mothers according to the gender of their children. After the intervention, STAI was completed for mothers of hospitalized children in both control and intervention groups.
After entering data in SPSS software version 23, data were analyzed using descriptive (frequency, Mean±SD) and inferential (the independent t-test, the chi-square test) statistics to compare between-group and within-group mean differences. Also, the Kolmogorov–Smirnov test assessed the normality of data distribution. The level of significance of statistical tests was considered P<0.05.
Results
The Mean±SD ages of mothers in the intervention and control groups were 36.9±10.87 and 34.44±9.27 years, respectively. The Mean±SD ages of children in the intervention and control groups were 3.5±6.29 and 2.89±6.73 years, respectively. Other demographic data of mothers and children are presented in Table 1.
The Kolmogorov-Smirnov test was used to assess the distribution of quantitative variables. The test results indicated that all quantitative demographic and intervening variables in this research had a normal distribution.
The result of the independent t-test revealed no statistically significant difference between the two groups in terms of the mean age of hospitalized children and their mothers. Moreover, the chi-square test result found no significant difference between the two groups of mothers in terms of their children’s gender and their level of education. Therefore, the two groups of mothers of the studied children were homogeneous regarding these variables.
The independent t-test within the group illustrated that in the stage before watching the animation video, the mean anxiety score of the mothers of hospitalized children in the two groups did not significantly differ (P=0.480), and the two groups were homogeneous regarding this variable. Nonetheless, the independent t-test results indicated a significant difference between the two groups after displaying the animation video (P=0.001). In the intervention group, the mean anxiety score decreased from 65.45±5.65 to 53.12±17.23 (Table 2).
Discussion
To determine the effect of display animation of urinary catheterization on the state anxiety of mothers with hospitalized children, the results demonstrated a significant decrease in their anxiety after the intervention. Moreover, a more marked reduction occurred in state anxiety scores after the intervention in the intervention group compared to that in the control group. In a literature review, a study similar to the current research was not found; therefore, the researcher tried to use the results of other studies in this section.
The findings of the present study indicate the high levels of anxiety among mothers in the intervention group before the intervention. Therefore, appropriate interventions must be made to alleviate their stress and enhance the informed consent process. The anxiety experienced by mothers before their children undergo invasive procedures can affect the treatment process [6]. Parental anxiety is associated with distress and problematic behaviors in children during and after hospitalization. In addition, unanswered questions and misinformation about invasive procedures can increase parental anxiety [12]. Children and their parents prefer to be informed about surgical intervention, anesthesia, possible pain problems, and other invasive procedures they may undergo during hospitalization [17, 18].
In this regard, according to a study by Paton et al., multimedia education significantly reduced parents’ anxiety during the informed consent process. According to the stated research, this method improves the knowledge and awareness of parents, lowers anxiety, and may improve parents’ long-term understanding and satisfaction in the healthcare process [10]. The results of the present research are consistent with the results of their study; nonetheless, the present study used animation videos to show urinary catheterization to the intervention group to control their anxiety.
The study by Book et al. demonstrated that the display of a 6-minute online video significantly reduced the anxiety of parents of children with inguinal hernia before surgery compared to the control group. Moreover, it enhanced the consent process and increased parental knowledge [19]. The present research results are consistent with the results of their study. The similarity in the research population (parents of children) can justify this consistency. However, it differed from the present study in which the educational animation video was not presented online, and the procedure performed on children differed. In general, the provision of accurate information can be a positive factor in reducing the anxiety of parents before their children undergo any aggressive procedure.
On the other hand, the study by Torres-Lagares et al. reported that watching a video of the removal of an inferior third molar surgery increased patients’ anxiety levels [20]. One of the reasons for this discrepancy is the difference in the content of the educational video, signifying that the educational content plays a key role in the anxiety level of people. In their study, all the surgical steps were shown, which can cause anxiety. It seems the most appropriate is to provide patients with the information they require in an adequate format.
The results of a study titled» parental educational intervention to facilitate informed consent» by Lin et al. showed that educational video-assisted informed consent was superior to the conventional process of obtaining parental consent in the emergency department and reduced anxiety [21]. The results of the present research were consist with their results. This consistency can be ascribed to the use of educational animation videos, although the treatment procedure was different in the study by Lin et al. Modern portable electronic devices, such as smartphones and tablets, as well as access to the Internet, open up new opportunities for information transfer. The good feature of the animation video used in the current study was its small file size and comprehensibility. Therefore, it can be easily accessed by parents through mobile phones. Also, they can be localized and provided in the native language of every country in medical centers. Further research is recommended to assess the effect of these variables. In a meta-analysis study conducted by Feeley et al. on 21 articles published from 2009 to 2020, the findings indicate an overall positive impact of using animation in improving viewers’ learning in various health and clinical fields, including surgery and diabetes [22]. Providing appropriate educational content and allowing parents to decide when and how often to watch the video will reduce their anxiety [23]. It is suggested that the effectiveness of this intervention be tested over other invasive methods, and its effect on anxiety should be investigated.
One of our limitations in this study was that during the COVID-19 pandemic, access to samples was difficult. The individual and cultural differences of the mothers participating in the research were other limitations of the present study, and it is suggested that the effect of this intervention on mothers’ anxiety in other cultures be evaluated as well.
The present study indicates that displaying an animation of urinary catheterization before the procedure reduces mothers’ anxiety levels. It is suggested to use this educational method before urinary catheterization in children, and because it reduces maternal anxiety, it may improve parental satisfaction with the healthcare process.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of Mashhad University of Medical Sciences (IR.MUMS.NURSE.REC.1400.054), receiving the letter of introduction and making necessary coordinating with the officials of this hospital. Written informed consent was obtained from all participants.
Funding
This study was extracted from the Master’s thesis of the Hadi Mazloum, approved by Department of Pediatric Nursing, School of Nursing and Midwifery, Mashhad University of Medical Sciences and was funded by Mashhad University of Medical Sciences (Grant No.: 990783).
Authors' contributions
Data collection: Hadi Mazloum and Nafiseh Pourbadakhshan; Writing the original draft: Naghmeh Razaghi; Study design, methodology, data analysis and final review: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors would like to thank the mothers who participated in this study.
References
- Boots BK, Edmundson EE. A controlled, randomised trial comparing single to multiple application lidocaine analgesia in paediatric patients undergoing urethral catheterisation procedures. J Clin Nurs. 2010; 19(5-6):744-8. [PMID]
- Gates A, Shulhan J, Featherstone R, Scott SD, Hartling L. A systematic review of parents’ experiences and information needs related to their child’s urinary tract infection. Patient Educ Couns. 2018; 101(7):1207-15. [DOI:10.1016/j.pec.2018.01.014] [PMID]
- Kleiber C, McCarthy AM. Parent behavior and child distress during urethral catheterization. J Soc Pediatr Nurs. 1999; 4(3):95-104. [[DOI:10.1111/j.1744-6155.1999.tb00042.x] [PMID]
- Piira T, Sugiura T, Champion GD, Donnelly N, Cole AS. The role of parental presence in the context of children’s medical procedures: A systematic review. Child Care Health Dev. 2005; 31(2):233-43. [DOI:10.1111/j.1365-2214.2004.00466.x] [PMID]
- Çamur Z, Sarıkaya Karabudak S. The effect of parental participation in the care of hospitalized children on parent satisfaction and parent and child anxiety: Randomized controlled trial. Int J Nurs Pract. 2021; 27(5):e12910. [DOI:10.1111/ijn.12910] [PMID]
- Pouresmail Z, Razaghi N, Rabbani Javadi A, Minaei Moghaddam S. [Evaluation of hospitalization anxiety in children and its relationship with maternal anxiety (Persian)]. Iran J Pediatr Nurs. 2022;9(1):12-21. [Link]
- Zarei N, Negarandeh R. The relationship between unmet needs of parents with hospitalized children and the level of parental anxiety in Iran. J Pediatr Nurs. 2021; 57:e74-e78. [DOI:10.1016/j.pedn.2020.11.010] [PMID]
- King PK, Martin SJ, Betka EM. Patient awareness and expectations of pharmacist services during hospital stay. J Pharm Pract. 2017; 30(5):506-15. [DOI:10.1177/0897190016665541] [PMID]
- Chakravarthy B, Somasundaram S, Mogi J, Burns R, Hoonpongsimanont W, Wiechmann W, et al. Randomized pilot trial measuring knowledge acquisition of opioid education in emergency department patients using a novel media platform. Subst Abus. 2018; 39(1):27-31. [DOI:10.1080/08897077.2017.1375061] [PMID]
- Paton EA, Davis SK, Gaylord N, Cao X, Gosain A. Impact of a multimedia teaching tool on parental anxiety and knowledge during the informed consent process. Pediatr Surg Int. 2018; 34(12):1345-52. [DOI:10.1007/s00383-018-4352-z] [PMID]
- Cohen LL, Rodrigues NP, Lim CS, Bearden DJ, Welkom JS, Joffe NE, et al. Automated parent-training for preschooler immunization pain relief: A randomized controlled trial. J Pediatr Psychol. 2015; 40(5):526-34. [DOI:10.1093/jpepsy/jsu162] [PMID]
- Brown EA, De Young A, Kimble R, Kenardy J. Review of a parent’s influence on pediatric procedural distress and recovery. Clin Child Fam Psychol Rev. 2018; 21(2):224-45. [DOI:10.1007/s10567-017-0252-3] [PMID]
- Ramanaiah NV, Franzen M, Schill T. A Psychometric Study of the State-Trait Anxiety Inventory. J Pers Assess. 1983; 47(5):531-5. [Link]
- Mahram B. [Standardization speilberger state-trait anxiety inventory in Mashad city (Persian)] [MA thesis]. Tehran: Allameh Tabatabai University; 1994. [Link]
- Wong DL, Hockenberry MJ, Wilson D, Winkelstein ML, Kline NE. Wong’s nursing care of infants and children. St. Louis: Mosby; 2003. [Link]
- Bowden VR, Greenberg CS. Pediatric nursing procedures. Pennsylvania: Lippincott Williams & Wilkins; 2012. [Link]
- Härter V, Barkmann C, Wiessner C, Rupprecht M, Reinshagen K, Trah J. Effects of educational video on pre-operative anxiety in children-A randomized controlled trial. Front Pediatr. 2021; 9:640236.[DOI:10.3389/fped.2021.640236] [PMID]
- Aranha PR, Dsouza SN. Preoperative information needs of parents: A descriptive survey.J Res Nurs. 2019; 24(5):305-14. [DOI:10.1177/1744987118821708] [PMID]
- Book F, Goedeke J, Poplawski A, Muensterer OJ. Access to an online video enhances the consent process, increases knowledge, and decreases anxiety of caregivers with children scheduled for inguinal hernia repair: A randomized controlled study. J Pediatr Surg. 2020; 55(1):18-28. [DOI:10.1016/j.jpedsurg.2019.09.047] [PMID]
- Torres-Lagares D, Heras-Meseguer M, Azcárate-Velázquez F, Hita-Iglesias P, Ruiz-de-León-Hernández G, Hernández-Pacheco E, et al. The effects of informed consent format on preoperative anxiety in patients undergoing inferior third molar surgery. Med Oral Patol Oral Cir Bucal. 2014; 19(3):e270-3. [DOI:10.4317/medoral.19480] [PMID]
- Lin YK, Yeh YS, Chen CW, Lee WC, Lin CJ, Kuo LC, et al. parental educational intervention to facilitate informed consent for pediatric procedural sedation in the emergency department: A parallel group randomized controlled trial. Healthcare (Basel). 2022; 10(12):2353. [DOI:10.3390/healthcare10122353] [PMID]
- Feeley TH, Keller M, Kayler L. Using animated videos to increase patient knowledge: A meta-analytic review. Health Educ Behav. 2023; 50(2):240-9. [DOI:10.1177/10901981221116791] [PMID]
- Vongkiatkajorn K, Brown EA, Donaldson A, Rich V, Paterson R, Kenardy J, et al. The effect of a parental preparation video [Take5] on child and parent anxiety during anaesthetic induction: A protocol for a randomised controlled trial. Trials. 2023; 24(1):446.[DOI:10.1186/s13063-023-07480-0] [PMID]
Article Type : Research |
Subject:
General
Received: 2023/06/9 | Accepted: 2024/04/12 | Published: 2024/07/1
Received: 2023/06/9 | Accepted: 2024/04/12 | Published: 2024/07/1
Send email to the article author
| Rights and permissions | |
 | This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
