Fri, Jul 12, 2024
Volume 34, Issue 3 (6-2024)
JHNM 2024, 34(3): 237-244 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Yulita Ichwan E, Dwi Fitriani C, Nirmala Sari G. Effectiveness of Audiovisual Media on Childbirth Support and Pregnancy Anxiety: A Quasi-experimental Study. JHNM 2024; 34 (3) :237-244
URL: http://hnmj.gums.ac.ir/article-1-2372-en.html
URL: http://hnmj.gums.ac.ir/article-1-2372-en.html



1- Associate Professor, Department of Midwifery, Polytechnic of Health, Ministry of Health Jakarta III, Jakarta, Indonesia. , ericka.eyi@gmail.com
2- Student of Bachelor of Applied Science in Midwifery, Polytechnic of Health, Ministry of Health Jakarta III, Jakarta, Indonesia.
3- Associate Professor, Department of Midwifery, Polytechnic of Health, Ministry of Health Jakarta III, Jakarta, Indonesia.
2- Student of Bachelor of Applied Science in Midwifery, Polytechnic of Health, Ministry of Health Jakarta III, Jakarta, Indonesia.
3- Associate Professor, Department of Midwifery, Polytechnic of Health, Ministry of Health Jakarta III, Jakarta, Indonesia.
Full-Text [PDF 466 kb]
(53 Downloads)
| Abstract (HTML) (194 Views)
Full-Text: (25 Views)
Introduction
Pregnancy is a natural event experienced by a woman. Changes in metabolism and hormonal systems in the body will affect physical and psychological conditions during pregnancy [1]. Anxiety is a manifestation of psychological changes that occur during pregnancy. Anxiety during pregnancy may occur throughout the pregnancy period from the first trimester to the last trimester [2]. Research in Brazil states that the prevalence of anxiety in pregnant women is around 26%, and 42.9% of it occurs in the third trimester [3]. Research in Pakistan found that out of 200 pregnant women, 70% experienced anxiety and 57.5% developed depression [4]. Anxiety during pregnancy that cannot be appropriately handled will have a negative impact on pregnancy outcomes [3, 5].
Anxiety in pregnant women has been proven to develop into a mental disorder, and it is more common to occur during the third trimester of pregnancy due to the rising fear caused by the approaching delivery process [6]. Several previous studies have shown that anxiety in pregnancy is closely related to the occurrence of pre-term birth, low birth weight, and abnormalities in newborns [7, 8]. Anxiety may also inhibit the labor process because of the release of catecholamine hormones that prevent uterine contractions [9].
Support and assistance given by the closest people are essential to reduce the level of anxiety during pregnancy. A grounded theory on husband's support states that involving the husband in providing support during pregnancy can make a wife feel more comfortable physically and emotionally and strengthen the couple's relationship [10]. A longitudinal study covering 176 pregnant women in Los Angeles found that partner support was effective in reducing cases of prenatal anxiety in the middle to late trimesters [11].
However, not all husbands understand that support during pregnancy is essential for every pregnant woman. A study in Nepal found that most husbands had little knowledge about forms of support during pregnancy, childbirth and the puerperium. The result of this study was closely related to labor preparation, which was not carried out properly due to the partner's poor knowledge [12]. The husband is one of the keys to enabling mothers to maintain positive emotions during pregnancy. Protective effects produced by increasing the partner's support may prevent adverse pregnancy outcomes [13]. A positive attitude and good support from husbands will make the pregnancy process fun and the condition of the fetus consistently solid and healthy [14].
Education about the role of husbands during pregnancy is necessary so husbands become aware and can support their partners during pregnancy [15]. A study that looks at the influence of husbands as supporters in promoting reproductive and sexual health states that media use in health promotion is essential as a strategy to improve cognitive behavior that demands changes for better health [16]. There have been many programs to increase husbands' knowledge about the importance of supporting mothers during pregnancy, but this knowledge is still rarely applied. Providing an education with audiovisual media improves the knowledge and attitudes of a person toward certain behaviors [17, 18]. It is necessary to assess the effectiveness of audiovisual media as an educational tool in increasing the husband's support during pregnancy as well as reducing the level of anxiety in pregnant women. This study aims to examine the effectiveness of audiovisual media as an educational tool in increasing husbands' support for women during pregnancy and assess its efficacy in reducing the level of anxiety in pregnant women between the pre-test and post-test stages.
Materials and Methods
This quasi-experimental study employed a pre-test-post-test design given to participants without a control group. The post-test was given after 7 days of intervention using the same measuring instruments (a questionnaire about pregnancy support for husbands and an anxiety measurement tool for pregnant women).
This study's sample comprised a group of pregnant women and their husbands visiting a prenatal clinic in Jakarta, Indonesia, where the study took place for three months (January-March 2022). These respondents were selected using a purposive sampling technique based on the inclusion and exclusion criteria. The inclusion criteria were pregnant women at ≥27 weeks of gestation, pregnant women in good health with no complications, without a history of depression or psychiatric disorders and or currently being treated for mental disorders, pregnant women whose partners were willing to receive health education about support during pregnancy according to the schedule of intervention stage in this research, and husband accompanies the antenatal check-up. Meanwhile, pregnant women with severe medical conditions, significant mental health problems, or substance abuse were not included to reduce risks and ensure accurate data. Those who could not speak Indonesian or read the questionnaire well were excluded from the study to ensure the research's communication process and ethical integrity. For some of the following cases, pregnant mothers and husbands were excluded as samples (exclusion criteria), namely pregnant women without their husbands' assistance during antenatal care or their husbands unwilling to be research respondents. Based on criteria for samples and calculations, 60 couples of mothers and husbands were drawn to serve as respondents in this study. The sample calculation was based on the sample calculation for a pre-test study using 1 group without control or comparison [19, 20].
The researchers developed the questionnaire used in this study and underwent an assessment for both validity and reliability. To assess validity, we focused on content validity and construct validity. Content validity was evaluated through expert review, while construct validity was assessed by examining the internal consistency among question items using the Pearson product-moment correlation coefficient. A high correlation among items indicates they likely measure the same underlying concept. A Pearson correlation coefficient (r) >0.361 was acceptable. Reliability was assessed through the Cronbach α, which measures the internal consistency of the questionnaire. A high Cronbach α indicates strong reliability, with a value of α=0.914, suggesting that the questionnaire items consistently measure the same construct.
In this study, a questionnaire was designed to evaluate the support husbands provided during their partners' pregnancy. The questionnaire contained 22 questions, each rated from 1 (strongly disagree) to 4 (strongly agree). The total possible score for the questionnaire ranged from 22 to 88. We established specific thresholds to categorize the levels of the husband's support. Before the intervention, a score above 66 indicated "good" support, while a score of 66 or below was labeled "poor." This threshold was derived from the mean score for the husband's support in the pre-test phase. After the intervention, the threshold for "good" support was raised to a score >71≥ indicating "poor" support. This adjustment was based on statistical analysis, considering the intervention's anticipated effect. The new threshold highlights a clear distinction between higher and lower levels of support after the intervention, suggesting that the intervention may have contributed to improved support. It also provides a more distinct separation between pre- and post-intervention support levels. The scientific content of the questionnaire has been reviewed by midwifery experts who are representatives of midwife scientists in Indonesian midwife organizations.
The level of anxiety in pregnant women was measured during the pre-test and post-test processes using an instrument called the hamilton anxiety rating scale (HARS), which has been translated into Indonesian. HARS is a tool for measuring anxiety in terms of general symptoms that may occur in pregnant women. HARS consists of 14 items, each of which has a possible score from 0 (no symptoms) to 4 (severe symptoms), and the total score is 56 [21]. HARS score >17 indicates that the respondent has moderate-severe anxiety and HARS score ≤17 means that the respondent has no mild anxiety [22].
Questionnaires for husbands include questions about respondents' characteristics, the role of husbands, what they have done to support pregnant women, and what the pregnant women received in it. The same questionnaire was given in the pre-test and post-test processes. In addition, the characteristics of respondents were screened using a data collection questionnaire. Characteristics of respondents assessed in this study were the mother's age, husband's age, mother's education, husband's education, mother's occupation, husband's occupation and parity. The data collection process started by giving a pre-test in the form of a questionnaire to respondents to assess the husband's support during pregnancy and the level of anxiety of pregnant women during pregnancy.
Next, after the pre-test was given to husbands and pregnant women, husbands were provided with education by midwives in the research center about their role in providing support for their wives during pregnancy using educational tools in the form of audiovisual media. This media was developed as a video that displays pictures and sounds containing things that husbands can do to support mothers during pregnancy. The authors developed the audiovisual medium in the form of a video with a duration of 5.20 minutes, which was shown to the husbands when accompanying their wives during antenatal visits at the research site. Media maker experts have reviewed this educational media and it has been tested on different respondents who are different people from the research respondents. The validity of the video content has been tested to see the clarity, understanding and clear appearance of the video material images (presentation) using the content validity index (CVI), with CVI results from −1 to 1 and the media items assessed are declared valid (CVI=0.96). The scientific content of the video has been reviewed by midwifery experts who were representatives of midwife scientists in Indonesian midwife organizations.
The video was presented at least 2 times in the same period and the husbands were asked to watch it carefully. Subsequently, the husbands were allowed to ask questions regarding the content of the video. Researchers who worked as midwives at the research site carried out the pre-test, post-test and intervention processes using audio visual media.
The frequency and percentage of each category were calculated using univariate analysis. A paired different test using the Wilcoxon test (the nonparametric equivalent of the paired t-test) was administered to measure the difference between the husband's support during pregnancy before and after the intervention. The difference in the level of anxiety in pregnant women before and after the intervention was also measured using the Wilcoxon test. P<0.05 indicates a significant difference in the husband's support and level of anxiety before and after the intervention. The association between the husband's support and the level of anxiety in pregnant women after intervention was also measured to obtain an odds ratio (OR) with a 95% confidence interval (CI) regression analysis using a logistic regression model. Processed data analysis was done using SPSS software, version 21.
Results
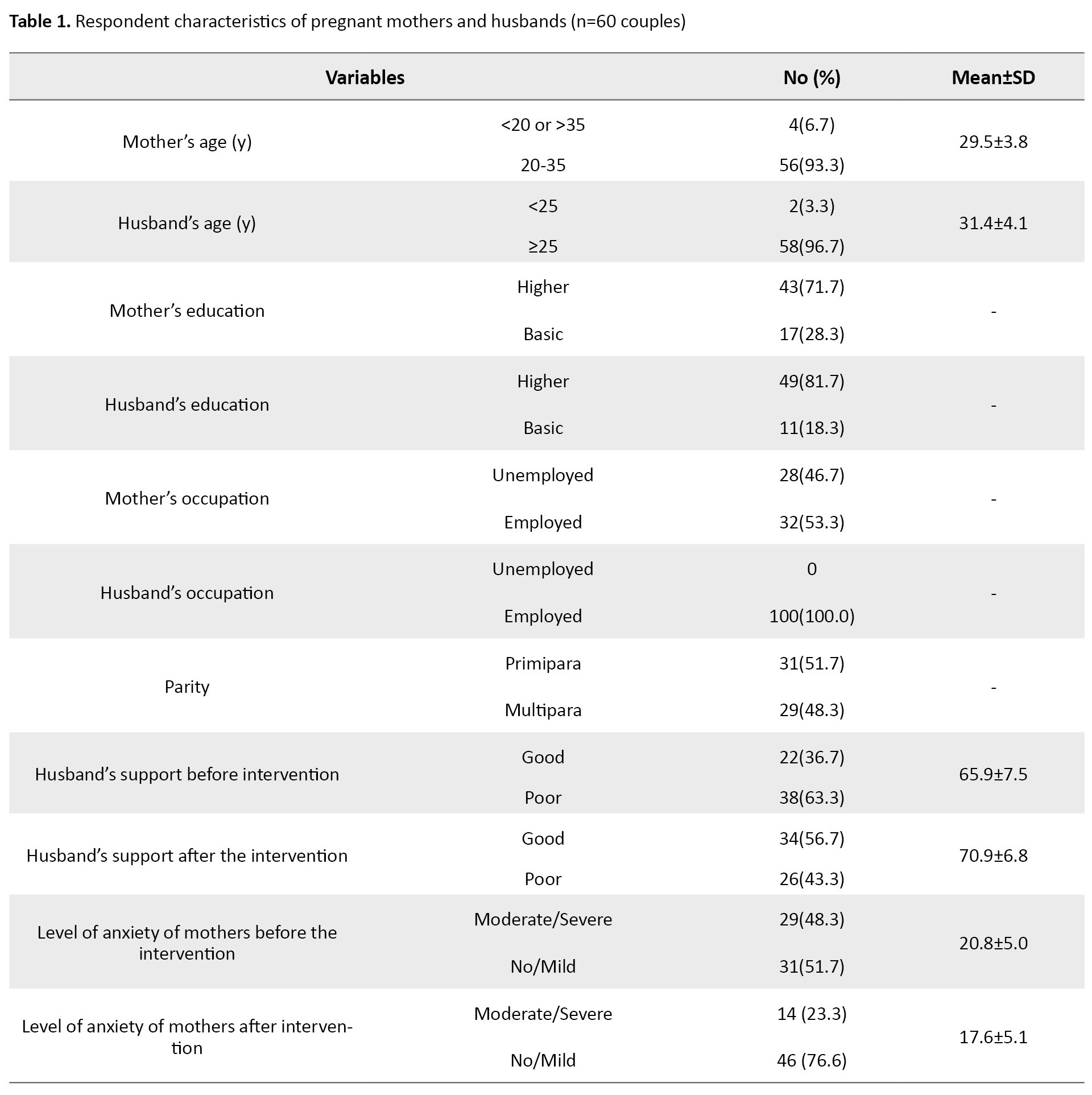
The results showed that most of the pregnant women were 20–35 years old (93.3%); the mean age of women was 29.5±3.8 years, had higher education (71.7%), employed (53.3%) and were primipara (51.7%). The characteristics of husbands were as follows: The mean age of the husband was 31.4±4.1 years, had higher education (81.7%) and employed (100%). Before the intervention, the husband's support was mostly poor (63.3%), with a mean score of 65.9±7.5. Most of the pregnant women had moderate to severe anxiety (51.7%), with a mean score of 20.8±5.0. Meanwhile, after the intervention, the husband's support during pregnancy was primarily good (56.7%), with a mean score of 70.9±6.8. The level of anxiety during pregnancy is mostly none or mild (76.6%), with the mean level of anxiety of the mother at 17.6±5.1 (Table 1).
The difference between the husband's support during pregnancy before and after intervention indicates an increase, with a mean rank of 29.50 (P=0.001). Meanwhile, the difference in the level of anxiety in pregnant women is also significant before intervention; the mean is 20.78 and after intervention, it falls to 12.60 with a mean rank of 29.00 (P=0.001). These results are shown in Table 2.
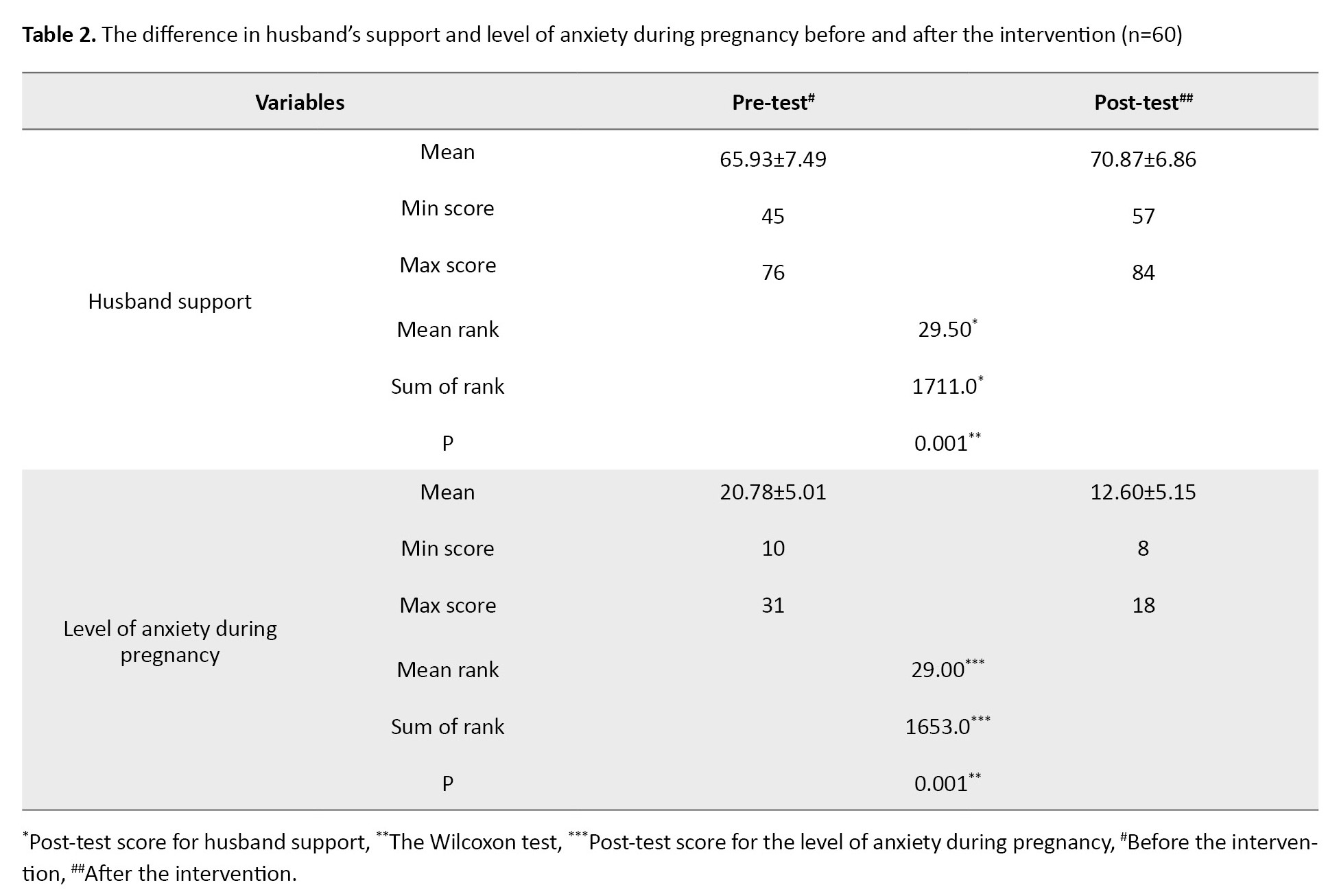
Table 3 presents the OR and 95% CI of the mother's anxiety during pregnancy after intervention based on the husband's support.
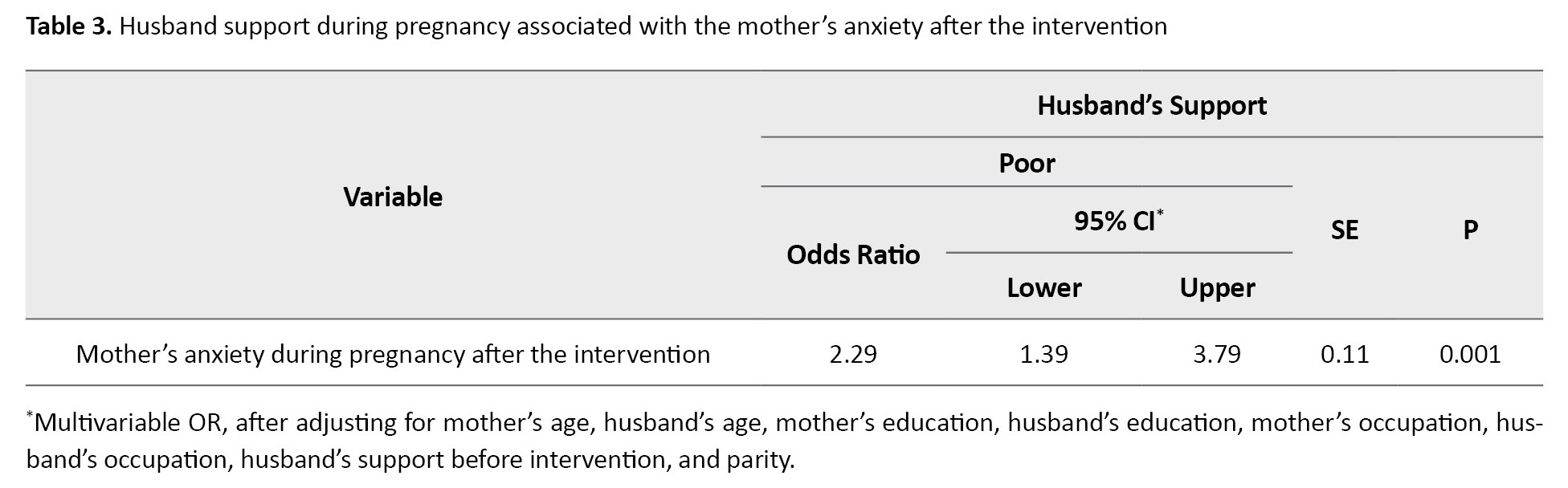
Pregnant women with a lack of husband's support will be at risk of experiencing a moderate to severe level of anxiety compared to pregnant women receiving good support from their husbands (OR=2.29, 95% CI; 1.39%, 3.79%, P=0.001).
Discussion
The results of this study indicate a difference in husband's support before and after the intervention. Husband's support during pregnancy increases after they receive education using audiovisual media about the importance of providing support during pregnancy. This finding indicates that education using audiovisual media effectively increases the husband's knowledge about the importance of supporting partners during pregnancy. A quasi-experimental study has proved the benefits of audiovisual media in improving the knowledge and attitudes of students who were given safe driving education using audiovisual media. This educational tool has proven helpful in increasing knowledge, attitudes and understanding of good driving norms [18]. In another quasi-experimental study on families in Indonesia, audiovisual media has been proven effective in improving family attitudes and behavior to prevent the transmission of dengue fever [17]. The use of audiovisual media in health education has confirmed that it improves knowledge acquisition faster and more effectively than other media [17, 18, 23]. Furthermore, it can provide more transparent and interesting information to prevent the audience from getting bored [23].
In our study, increasing the husband's support during pregnancy was beneficial in reducing the level of anxiety in pregnant women. There is a significant decrease in the level of anxiety in pregnant women after their husbands receive an education, as it increases their support for their pregnant wives. In addition, the results of this study imply that the husband's great support is closely related to a decrease in the level of anxiety in mothers during pregnancy. The results of this study are consistent with an observational cohort study in the USA, which found that lack of partner support during pregnancy was associated with a high level of anxiety in pregnant women [13]. A longitudinal study also reported that pregnant women who received solid social support from their partners showed mild emotional distress, and it impacted the babies they gave birth to, which also showed less distress responses [14]. Husband's support during pregnancy is the key to creating a sense of security in pregnant women and may also increase good perinatal outcomes for both mother and infant [10, 14]. Husbands who care about the condition of their pregnant wives will provide a psychological environment that is useful for them to develop their ability to adapt to any conditions that may occur during pregnancy [24]. With the creation of a sense of security during pregnancy, pregnant women will have a self-defense mechanism against the anxiety and fear that they may feel during pregnancy [24].
Anxiety during pregnancy should not be neglected. Anxiety has a negative impact on mothers during pregnancy, childbirth, and postpartum. The adverse effects of anxiety during pregnancy are also detected in the fetal and infancy periods [8, 25]. Increased support from the closest people in the social circle has a good impact on preventing stress and anxiety during pregnancy. Support from the closest people (husband, friends and family) plays an essential role in decreasing the level of anxiety during pregnancy [26].
This research is a quasi-experimental study with strict criteria for a sample to avoid bias in selecting respondents, but it has limitations. This study did not use a control group to which a comparison was made. It only assessed the audiovisual media method and did not compare it with other educational tools. Adding a group using other educational media as a control group may improve the study results.
In conclusion, this study has presented evidence that providing husbands with audiovisual media may increase husband's support for pregnant women during pregnancy. In addition, there is a decrease in the level of anxiety in pregnant women after their husbands receive education through audiovisual media. This study also shows that pregnant women with no support from their husbands will be at risk of experiencing moderate to severe anxiety. This study implies that it is necessary to increase husband's concern about the importance of providing support for their wives during pregnancy because it helps reduce the level of maternal anxiety. The role of health workers is crucial in delivering education through audiovisual media to improve the husband's knowledge about the importance of providing support during pregnancy.
Ethical Considerations
Compliance with ethical guidelines
The present study was approved by the Ethics Committee of University of Respati Indonesia (Code: 179/SK.KEPK/UNRI/IV/2022). All respondents were provided information about the study process and signed informed consent forms. All respondents can withdraw their consent anytime and leave the study process.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Study design: Erika Yulita Ichwan; Data collection: Chandra Dwi Fitriani; Writing the original draft: Gita Nirmala Sari; Conceptualization and data analysis: Erika Yulita Ichwan and Chandra Dwi Fitriani; Data interpretation, review, editing and final approval: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The researchers thank the Prenatal Clinic in Jakarta Capital Special Region for allowing it to be used as a research site. The researchers also thanked the midwives who helped with the research project.
References
Pregnancy is a natural event experienced by a woman. Changes in metabolism and hormonal systems in the body will affect physical and psychological conditions during pregnancy [1]. Anxiety is a manifestation of psychological changes that occur during pregnancy. Anxiety during pregnancy may occur throughout the pregnancy period from the first trimester to the last trimester [2]. Research in Brazil states that the prevalence of anxiety in pregnant women is around 26%, and 42.9% of it occurs in the third trimester [3]. Research in Pakistan found that out of 200 pregnant women, 70% experienced anxiety and 57.5% developed depression [4]. Anxiety during pregnancy that cannot be appropriately handled will have a negative impact on pregnancy outcomes [3, 5].
Anxiety in pregnant women has been proven to develop into a mental disorder, and it is more common to occur during the third trimester of pregnancy due to the rising fear caused by the approaching delivery process [6]. Several previous studies have shown that anxiety in pregnancy is closely related to the occurrence of pre-term birth, low birth weight, and abnormalities in newborns [7, 8]. Anxiety may also inhibit the labor process because of the release of catecholamine hormones that prevent uterine contractions [9].
Support and assistance given by the closest people are essential to reduce the level of anxiety during pregnancy. A grounded theory on husband's support states that involving the husband in providing support during pregnancy can make a wife feel more comfortable physically and emotionally and strengthen the couple's relationship [10]. A longitudinal study covering 176 pregnant women in Los Angeles found that partner support was effective in reducing cases of prenatal anxiety in the middle to late trimesters [11].
However, not all husbands understand that support during pregnancy is essential for every pregnant woman. A study in Nepal found that most husbands had little knowledge about forms of support during pregnancy, childbirth and the puerperium. The result of this study was closely related to labor preparation, which was not carried out properly due to the partner's poor knowledge [12]. The husband is one of the keys to enabling mothers to maintain positive emotions during pregnancy. Protective effects produced by increasing the partner's support may prevent adverse pregnancy outcomes [13]. A positive attitude and good support from husbands will make the pregnancy process fun and the condition of the fetus consistently solid and healthy [14].
Education about the role of husbands during pregnancy is necessary so husbands become aware and can support their partners during pregnancy [15]. A study that looks at the influence of husbands as supporters in promoting reproductive and sexual health states that media use in health promotion is essential as a strategy to improve cognitive behavior that demands changes for better health [16]. There have been many programs to increase husbands' knowledge about the importance of supporting mothers during pregnancy, but this knowledge is still rarely applied. Providing an education with audiovisual media improves the knowledge and attitudes of a person toward certain behaviors [17, 18]. It is necessary to assess the effectiveness of audiovisual media as an educational tool in increasing the husband's support during pregnancy as well as reducing the level of anxiety in pregnant women. This study aims to examine the effectiveness of audiovisual media as an educational tool in increasing husbands' support for women during pregnancy and assess its efficacy in reducing the level of anxiety in pregnant women between the pre-test and post-test stages.
Materials and Methods
This quasi-experimental study employed a pre-test-post-test design given to participants without a control group. The post-test was given after 7 days of intervention using the same measuring instruments (a questionnaire about pregnancy support for husbands and an anxiety measurement tool for pregnant women).
This study's sample comprised a group of pregnant women and their husbands visiting a prenatal clinic in Jakarta, Indonesia, where the study took place for three months (January-March 2022). These respondents were selected using a purposive sampling technique based on the inclusion and exclusion criteria. The inclusion criteria were pregnant women at ≥27 weeks of gestation, pregnant women in good health with no complications, without a history of depression or psychiatric disorders and or currently being treated for mental disorders, pregnant women whose partners were willing to receive health education about support during pregnancy according to the schedule of intervention stage in this research, and husband accompanies the antenatal check-up. Meanwhile, pregnant women with severe medical conditions, significant mental health problems, or substance abuse were not included to reduce risks and ensure accurate data. Those who could not speak Indonesian or read the questionnaire well were excluded from the study to ensure the research's communication process and ethical integrity. For some of the following cases, pregnant mothers and husbands were excluded as samples (exclusion criteria), namely pregnant women without their husbands' assistance during antenatal care or their husbands unwilling to be research respondents. Based on criteria for samples and calculations, 60 couples of mothers and husbands were drawn to serve as respondents in this study. The sample calculation was based on the sample calculation for a pre-test study using 1 group without control or comparison [19, 20].
The researchers developed the questionnaire used in this study and underwent an assessment for both validity and reliability. To assess validity, we focused on content validity and construct validity. Content validity was evaluated through expert review, while construct validity was assessed by examining the internal consistency among question items using the Pearson product-moment correlation coefficient. A high correlation among items indicates they likely measure the same underlying concept. A Pearson correlation coefficient (r) >0.361 was acceptable. Reliability was assessed through the Cronbach α, which measures the internal consistency of the questionnaire. A high Cronbach α indicates strong reliability, with a value of α=0.914, suggesting that the questionnaire items consistently measure the same construct.
In this study, a questionnaire was designed to evaluate the support husbands provided during their partners' pregnancy. The questionnaire contained 22 questions, each rated from 1 (strongly disagree) to 4 (strongly agree). The total possible score for the questionnaire ranged from 22 to 88. We established specific thresholds to categorize the levels of the husband's support. Before the intervention, a score above 66 indicated "good" support, while a score of 66 or below was labeled "poor." This threshold was derived from the mean score for the husband's support in the pre-test phase. After the intervention, the threshold for "good" support was raised to a score >71≥ indicating "poor" support. This adjustment was based on statistical analysis, considering the intervention's anticipated effect. The new threshold highlights a clear distinction between higher and lower levels of support after the intervention, suggesting that the intervention may have contributed to improved support. It also provides a more distinct separation between pre- and post-intervention support levels. The scientific content of the questionnaire has been reviewed by midwifery experts who are representatives of midwife scientists in Indonesian midwife organizations.
The level of anxiety in pregnant women was measured during the pre-test and post-test processes using an instrument called the hamilton anxiety rating scale (HARS), which has been translated into Indonesian. HARS is a tool for measuring anxiety in terms of general symptoms that may occur in pregnant women. HARS consists of 14 items, each of which has a possible score from 0 (no symptoms) to 4 (severe symptoms), and the total score is 56 [21]. HARS score >17 indicates that the respondent has moderate-severe anxiety and HARS score ≤17 means that the respondent has no mild anxiety [22].
Questionnaires for husbands include questions about respondents' characteristics, the role of husbands, what they have done to support pregnant women, and what the pregnant women received in it. The same questionnaire was given in the pre-test and post-test processes. In addition, the characteristics of respondents were screened using a data collection questionnaire. Characteristics of respondents assessed in this study were the mother's age, husband's age, mother's education, husband's education, mother's occupation, husband's occupation and parity. The data collection process started by giving a pre-test in the form of a questionnaire to respondents to assess the husband's support during pregnancy and the level of anxiety of pregnant women during pregnancy.
Next, after the pre-test was given to husbands and pregnant women, husbands were provided with education by midwives in the research center about their role in providing support for their wives during pregnancy using educational tools in the form of audiovisual media. This media was developed as a video that displays pictures and sounds containing things that husbands can do to support mothers during pregnancy. The authors developed the audiovisual medium in the form of a video with a duration of 5.20 minutes, which was shown to the husbands when accompanying their wives during antenatal visits at the research site. Media maker experts have reviewed this educational media and it has been tested on different respondents who are different people from the research respondents. The validity of the video content has been tested to see the clarity, understanding and clear appearance of the video material images (presentation) using the content validity index (CVI), with CVI results from −1 to 1 and the media items assessed are declared valid (CVI=0.96). The scientific content of the video has been reviewed by midwifery experts who were representatives of midwife scientists in Indonesian midwife organizations.
The video was presented at least 2 times in the same period and the husbands were asked to watch it carefully. Subsequently, the husbands were allowed to ask questions regarding the content of the video. Researchers who worked as midwives at the research site carried out the pre-test, post-test and intervention processes using audio visual media.
The frequency and percentage of each category were calculated using univariate analysis. A paired different test using the Wilcoxon test (the nonparametric equivalent of the paired t-test) was administered to measure the difference between the husband's support during pregnancy before and after the intervention. The difference in the level of anxiety in pregnant women before and after the intervention was also measured using the Wilcoxon test. P<0.05 indicates a significant difference in the husband's support and level of anxiety before and after the intervention. The association between the husband's support and the level of anxiety in pregnant women after intervention was also measured to obtain an odds ratio (OR) with a 95% confidence interval (CI) regression analysis using a logistic regression model. Processed data analysis was done using SPSS software, version 21.
Results
The results showed that most of the pregnant women were 20–35 years old (93.3%); the mean age of women was 29.5±3.8 years, had higher education (71.7%), employed (53.3%) and were primipara (51.7%). The characteristics of husbands were as follows: The mean age of the husband was 31.4±4.1 years, had higher education (81.7%) and employed (100%). Before the intervention, the husband's support was mostly poor (63.3%), with a mean score of 65.9±7.5. Most of the pregnant women had moderate to severe anxiety (51.7%), with a mean score of 20.8±5.0. Meanwhile, after the intervention, the husband's support during pregnancy was primarily good (56.7%), with a mean score of 70.9±6.8. The level of anxiety during pregnancy is mostly none or mild (76.6%), with the mean level of anxiety of the mother at 17.6±5.1 (Table 1).
The difference between the husband's support during pregnancy before and after intervention indicates an increase, with a mean rank of 29.50 (P=0.001). Meanwhile, the difference in the level of anxiety in pregnant women is also significant before intervention; the mean is 20.78 and after intervention, it falls to 12.60 with a mean rank of 29.00 (P=0.001). These results are shown in Table 2.
Table 3 presents the OR and 95% CI of the mother's anxiety during pregnancy after intervention based on the husband's support.
Pregnant women with a lack of husband's support will be at risk of experiencing a moderate to severe level of anxiety compared to pregnant women receiving good support from their husbands (OR=2.29, 95% CI; 1.39%, 3.79%, P=0.001).
Discussion
The results of this study indicate a difference in husband's support before and after the intervention. Husband's support during pregnancy increases after they receive education using audiovisual media about the importance of providing support during pregnancy. This finding indicates that education using audiovisual media effectively increases the husband's knowledge about the importance of supporting partners during pregnancy. A quasi-experimental study has proved the benefits of audiovisual media in improving the knowledge and attitudes of students who were given safe driving education using audiovisual media. This educational tool has proven helpful in increasing knowledge, attitudes and understanding of good driving norms [18]. In another quasi-experimental study on families in Indonesia, audiovisual media has been proven effective in improving family attitudes and behavior to prevent the transmission of dengue fever [17]. The use of audiovisual media in health education has confirmed that it improves knowledge acquisition faster and more effectively than other media [17, 18, 23]. Furthermore, it can provide more transparent and interesting information to prevent the audience from getting bored [23].
In our study, increasing the husband's support during pregnancy was beneficial in reducing the level of anxiety in pregnant women. There is a significant decrease in the level of anxiety in pregnant women after their husbands receive an education, as it increases their support for their pregnant wives. In addition, the results of this study imply that the husband's great support is closely related to a decrease in the level of anxiety in mothers during pregnancy. The results of this study are consistent with an observational cohort study in the USA, which found that lack of partner support during pregnancy was associated with a high level of anxiety in pregnant women [13]. A longitudinal study also reported that pregnant women who received solid social support from their partners showed mild emotional distress, and it impacted the babies they gave birth to, which also showed less distress responses [14]. Husband's support during pregnancy is the key to creating a sense of security in pregnant women and may also increase good perinatal outcomes for both mother and infant [10, 14]. Husbands who care about the condition of their pregnant wives will provide a psychological environment that is useful for them to develop their ability to adapt to any conditions that may occur during pregnancy [24]. With the creation of a sense of security during pregnancy, pregnant women will have a self-defense mechanism against the anxiety and fear that they may feel during pregnancy [24].
Anxiety during pregnancy should not be neglected. Anxiety has a negative impact on mothers during pregnancy, childbirth, and postpartum. The adverse effects of anxiety during pregnancy are also detected in the fetal and infancy periods [8, 25]. Increased support from the closest people in the social circle has a good impact on preventing stress and anxiety during pregnancy. Support from the closest people (husband, friends and family) plays an essential role in decreasing the level of anxiety during pregnancy [26].
This research is a quasi-experimental study with strict criteria for a sample to avoid bias in selecting respondents, but it has limitations. This study did not use a control group to which a comparison was made. It only assessed the audiovisual media method and did not compare it with other educational tools. Adding a group using other educational media as a control group may improve the study results.
In conclusion, this study has presented evidence that providing husbands with audiovisual media may increase husband's support for pregnant women during pregnancy. In addition, there is a decrease in the level of anxiety in pregnant women after their husbands receive education through audiovisual media. This study also shows that pregnant women with no support from their husbands will be at risk of experiencing moderate to severe anxiety. This study implies that it is necessary to increase husband's concern about the importance of providing support for their wives during pregnancy because it helps reduce the level of maternal anxiety. The role of health workers is crucial in delivering education through audiovisual media to improve the husband's knowledge about the importance of providing support during pregnancy.
Ethical Considerations
Compliance with ethical guidelines
The present study was approved by the Ethics Committee of University of Respati Indonesia (Code: 179/SK.KEPK/UNRI/IV/2022). All respondents were provided information about the study process and signed informed consent forms. All respondents can withdraw their consent anytime and leave the study process.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Study design: Erika Yulita Ichwan; Data collection: Chandra Dwi Fitriani; Writing the original draft: Gita Nirmala Sari; Conceptualization and data analysis: Erika Yulita Ichwan and Chandra Dwi Fitriani; Data interpretation, review, editing and final approval: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The researchers thank the Prenatal Clinic in Jakarta Capital Special Region for allowing it to be used as a research site. The researchers also thanked the midwives who helped with the research project.
References
- Soma-Pillay P, Nelson-Piercy C, Tolppanen H, Mebazaa A. Physiological changes in pregnancy. Cardiovasc J Afr. 2016; 27(2):89-94. [DOI:10.5830/CVJA-2016-021] [PMID] [PMCID]
- Bjelica A, Cetkovic N, Trninic-Pjevic A, Mladenovic-Segedi L. The phenomenon of pregnancy - a psychological view. Ginekol Pol. 2018; 89(2):102-6. [DOI:10.5603/GP.a2018.0017] [PMID]
- Silva MMJ, Nogueira DA, Clapis MJ, Leite EPRC. Anxiety in pregnancy: Prevalence and associated factors. Rev da Esc Enferm da USP. 2017; 51:e03253. [DOI:10.1590/s1980-220x2016048003253] [PMID]
- Irum S, Khan AA, Rabbani U, Lodhi FS, Elsous A. Frequency and risk factors of anxiety and depression among pregnant women in Abbottabad, Pakistan: A facility-based cross-sectional study. Pakistan J Med Health Sci. 2022; 16(7):465-8. [Link]
- Basharpoor S, Heydarirad H, Daryadel SJ, Heydari F, Ghamari Givi H, Kishore J. The role of perceived stress and social support among predicting anxiety in pregnant women. J Holist Nurs Midwifery. 2017; 27(2):9-16. [Link]
- Shahhosseini Z, Pourasghar M, Khalilian A, Salehi F. A review of the effects of anxiety during pregnancy on children’s health. Mater Sociomed. 2015; 27(3):200-2. [DOI:10.5455/msm.2015.27.200-202] [PMID] [PMCID]
- Dunkel Schetter C, Tanner L. Anxiety, depression and stress in pregnancy: Implications for mothers, children, research, and practice. Curr Opin Psychiatry. 2012; 25(2):141-8. [DOI:10.1097/YCO.0b013e3283503680] [PMID] [PMCID]
- Alder J, Fink N, Bitzer J, Hösli I, Holzgreve W. Depression and anxiety during pregnancy: A risk factor for obstetric, fetal and neonatal outcome? A critical review of the literature. J Matern Fetal Neonatal Med. 2007; 20(3):189-209. [DOI:10.1080/14767050701209560] [PMID]
- Aryani F. Factors affecting the primigravida anxiety during the 3rd trimester of pregnancy regarding the upcoming labor. J Ners dan Kebidanan Indones. 2018; 6(1):72-6. [Link]
- Eddy BP, Fife ST. Active husband involvement during pregnancy: A grounded theory. Fam Relat. 2021; 70(4):1222-37. [Link]
- Rini CH, Schetter CD, Hobel CJ, Glynn LM, Sandman CA. Effective social support: Antecedents and consequences of partner support during pregnancy. Pers Relat. 2006; 13(2):207-29. [DOI:10.1111/j.1475-6811.2006.00114.x]
- Bhatta B. An exploratory study of prevailing knowledge, attitude and practice of husband in regards to factors affecting in supporting activities during pregnancy, delivery and postpartum periods. J Nobel Med Coll. 2012; 1(1):45-52. [DOI:10.3126/jonmc.v1i1.7287]
- Cheng ER, Rifas-Shiman SL, Perkins ME, Rich-Edwards JW, Gillman MW, Wright R, et al. The influence of antenatal partner support on pregnancy outcomes. J Womens Health (Larchmt). 2016; 25(7):672-9. [DOI:10.1089/jwh.2015.5462] [PMID] [PMCID]
- Stapleton LR, Schetter CD, Westling E, Rini C, Glynn LM, Hobel CJ, et al. Perceived partner support in pregnancy predicts lower maternal and infant distress. J Fam Psychol. 2012; 26(3):453-63.[DOI:10.1037/a0028332] [PMID] [PMCID]
- Mosunmola S, Adekunbi F, Foluso O. Women’s perception of husbands’ support during pregnancy, labour and delivery. IOSR J Nurs Health Sci. 2014; 3(3):45-50. [DOI:10.9790/1959-03314550]
- Lewis S, Lee A, Simkhada P. The role of husbands in maternal health and safe childbirth in rural Nepal: A qualitative study. BMC Pregnancy Childbirth. 2015; 15:162. [DOI:10.1186/s12884-015-0599-8] [PMID] [PMCID]
- Arneliwati, Agrina, Dewi AP. The effectiveness of health education using audiovisual media on increasing family behavior in preventing dengue hemorrhagic fever (DHF). Enferm Clín. 2019; 29(1):30-3. [DOI:10.1016/j.enfcli.2018.11.013]
- Rahman W, Setyowati DL, Ifroh RH. Effect of health education of safety riding using audiovisual media on knowledge, attitudes and subjective norms of junior high school students in Samarinda Indonesia. Public Health Indones. 2019; 5(3):54-61. [DOI:10.36685/phi.v5i3.264]
- Tongco MDC. Purposive sampling as a tool for informant selection. Ethnobot Res Appl. 2007; 5:147-58. [Link]
- Eng J. Sample size estimation: How many individuals should be studied? Radiology. 2003; 227(2):309-13. [DOI:10.1148/radiol.2272012051] [PMID]
- Thompson E. Hamilton Rating Scale for Anxiety (HAM-A). Occup Med (Lond). 2015; 65(7):601. [DOI:10.1093/occmed/kqv054] [PMID]
- Ramdan IM. Reliability and Validity Test of the Indonesian Version of the Hamilton Anxiety Rating Scale (HAM-A) to measure work-related stress in nursing. J Ners. 2019; 14(1):33. [DOI:10.20473/jn.v13i2.10673]
- Anwar AI, Zulkifli A, Syafar M, Jafar N. Effectiveness of counseling with cartoon animation audiovisual methods in increasing tooth brushing knowledge children ages 10-12 years. Enferm Clín. 2020; 30(2):285-8. [DOI:10.1016/j.enfcli.2019.07.104]
- Duman NB, Kocak C. The effect of social support on state anxiety levels during pregnancy. Soc Behav Personal Int J. 2013; 41(7):1153-63. [DOI:10.2224/sbp.2013.41.7.1153]
- Larsson C, Sydsjö G, Josefsson A. Health, sociodemographic data, and pregnancy outcome in women with antepartum depressive symptoms. Obstet Gynecol. 2004; 104(3):459-66. [DOI:10.1097/01.AOG.0000136087.46864.e4] [PMID]
- Glazier RH, Elgar FJ, Goel V, Holzapfel S. Stress, social support, and emotional distress in a community sample of pregnant women. J Psychosom Obstet Gynaecol. 2004; 25(3-4):247-55. [DOI:10.1080/01674820400024406] [PMID]
Article Type : Research |
Subject:
General
Received: 2023/02/15 | Accepted: 2024/01/22 | Published: 2024/07/1
Received: 2023/02/15 | Accepted: 2024/01/22 | Published: 2024/07/1
Send email to the article author
| Rights and permissions | |
 | This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
