Sun, Apr 28, 2024
Volume 34, Issue 2 (2-2024)
JHNM 2024, 34(2): 151-158 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Khalajinia Z, Sharifi M H, Ahangari R, Mousavi F S, Vahedian M. Prevalence and Risk Factors of Third-and Fourth-degree Perineal Tears During Vaginal Delivery Among Women in Qom, Iran. JHNM 2024; 34 (2) :151-158
URL: http://hnmj.gums.ac.ir/article-1-2307-en.html
URL: http://hnmj.gums.ac.ir/article-1-2307-en.html
Zohre Khalajinia1 

 , Mohammad Hassan Sharifi2 , Roghayyeh Ahangari3 , Fatemeh Sadat Mousavi * 4, Mostafa Vahedian5
, Mohammad Hassan Sharifi2 , Roghayyeh Ahangari3 , Fatemeh Sadat Mousavi * 4, Mostafa Vahedian5
, Mohammad Hassan Sharifi2 , Roghayyeh Ahangari3 , Fatemeh Sadat Mousavi * 4, Mostafa Vahedian5
1- Associated Professor, Department of Midwifery, School of Nursing and Midwifery, Qom University of Medical Sciences. Qom, Iran.
2- MD, Medicine School, Qom University of Medical Sciences, Qom, Iran.
3- Assistant Professor, Department of Obstetrics and Gynecology, School of Medicine, Nekouei-Hedayati-Forghani Hospital, Qom University of Medical Sciences, Qom, Iran.
4- Instructor, Department of Midwifery, School of Nursing and Midwifery, Qom University of Medical Sciences, Qom, Iran. , mousavif.1990@gmail.com
5- Assistant Professor, Neuroscience Research Center, Qom University of Medical Sciences, Qom, Iran.
2- MD, Medicine School, Qom University of Medical Sciences, Qom, Iran.
3- Assistant Professor, Department of Obstetrics and Gynecology, School of Medicine, Nekouei-Hedayati-Forghani Hospital, Qom University of Medical Sciences, Qom, Iran.
4- Instructor, Department of Midwifery, School of Nursing and Midwifery, Qom University of Medical Sciences, Qom, Iran. , mousavif.1990@gmail.com
5- Assistant Professor, Neuroscience Research Center, Qom University of Medical Sciences, Qom, Iran.
Full-Text [PDF 567 kb]
(89 Downloads)
| Abstract (HTML) (167 Views)
Full-Text: (32 Views)
Introduction
Perineal tear during childbirth is common and may be caused by episiotomy and/or spontaneous tear of the perineum [1]. Perineum tears are classified into four degrees. First- and second-degree tears involve injury to only the vaginal mucosa and perineal muscles (mild). Third- and fourth-degree tears involve injury to the anal sphincter and the rectal mucosa, respectively (severe) [2]. More than 85% of women during normal vaginal delivery (NVD) experience some kind of perineal tears during the passage of the baby through the vagina, most of which are mild tears [3]. Mild perineal tears are very common and have been reported to occur in 73% of primiparous deliveries. Severe perineal tears are much less common. Reported prevalence rates vary from 0.1 to 8% in different populations. In some countries, a significant increase has been recorded in the last three decades [4]. In Iran, the prevalence of third- and fourth-degree perineal tears is in a range from 0.16% to 0.36% [5]. Anal sphincter injury occurs only in severe perineal tears, which cause significant complications compared to first- or second-degree perineal tears. Abscess formation, wound rupture, rectovaginal fistula (an abnormal connection between the rectum and vagina), and fecal incontinence have been reported following anal sphincter injury. Failure to properly treat such injuries may cause both short-term and long-term complications, including urinary and fecal incontinence, bleeding, infection, pain, painful intercourse, sexual dysfunction, and reduced quality of life [1]. Anal sphincter injury is one of the most common complaints in medical court cases, which causes tension for the patient and those involved in childbirth [6]. Despite the mentioned complications, there is no agreement on preventive measures and clinical management of severe perineal tears. Identifying the risk factors of these tears can help in their prevention. For this reason, clinical guidelines emphasize the importance of knowing the factors contributing to severe perineal tears. However, there is conflicting information about the importance of obstetric factors causing these tears [5].
The factors mentioned in the literature are Asian race, being prime par, mother’s age, persistent occiput posterior, prolongation of the second phase of labor, high birth weight, labor induction with oxytocin, low work experience of the laborer, gestational diabetes, passing the due date of delivery, delivery with vacuum, and episiotomy [1, 3-5, 7]. Since the studies conducted in this field are limited, especially in Iran, this study was conducted to determine the prevalence of severe perineal tears during NVD in Qom, Iran, and find its risk factors.
Materials and Methods
This is a descriptive-analytical, retrospective study with a case-control design, which was conducted on the medical records of women who gave birth from March 2010 to March 2019 in three teaching hospitals in Qom. Inclusion criteria included singleton pregnancy with cephalic presentation and gestational age greater than 20 weeks (or fetal weight greater than 500 g when gestational age is unknown). Incomplete files and the data of mothers with cesarean section were excluded. Information was collected using a checklist surveying demographic information, previous medical history, and obstetric information. The extracted information included mother’s age, mother’s history of illness, mother’s body mass index (BMI), gestational age, gravidity, parity, type of perineal tear, type of spinal anesthesia, use/non-use of narcotic drugs for pain relief, length of the active phase of the first stage of labor, length of the second stage of labor, length of hospitalization until delivery, length of water breaking, having/not having an episiotomy, position of the fetus during delivery (occiput posterior or occiput anterior), use of oxytocin to induce labor, mode of delivery, instrumental delivery, occurrence/not occurrence of shoulder dystocia, and race, weight and sex of the newborn.
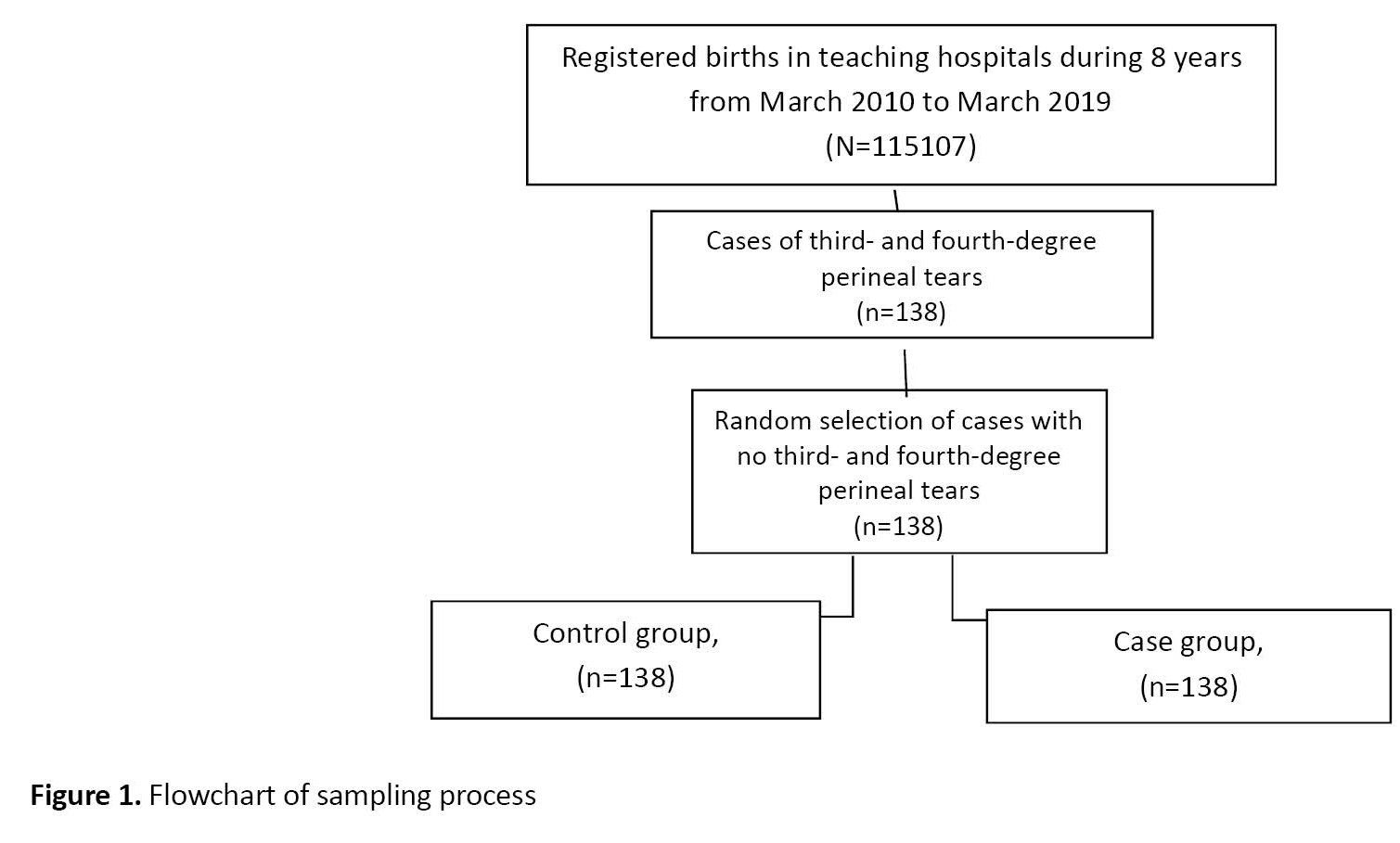
After the approval of the ethics committee of Qom University of Medical Sciences and obtaining permission from the hospital managers, the vaginal delivery registration system of the hospitals was checked. Then, cases of third- and fourth-degree perineal tears were searched, their clinical files were examined, and their information was extracted. Considering that among the 115,107 births performed in these hospitals, 138 cases had third- and fourth-degree tears, the same number of cases of women with no severe tears were randomly selected based on the inclusion criteria. Finally, there were 138 women in each case and control group (Figure 1).
 After collecting the data, they were entered into SPSS software, version 22. Mean±SD were used to describe quantitative data, and frequency and percentage were used to describe qualitative data. The statistical tests used for data analysis included an independent t-test, chi-square test, Fisher’s exact test, and multivariate logistic regression analysis. The significance level was set at 0.05.
After collecting the data, they were entered into SPSS software, version 22. Mean±SD were used to describe quantitative data, and frequency and percentage were used to describe qualitative data. The statistical tests used for data analysis included an independent t-test, chi-square test, Fisher’s exact test, and multivariate logistic regression analysis. The significance level was set at 0.05.
Results
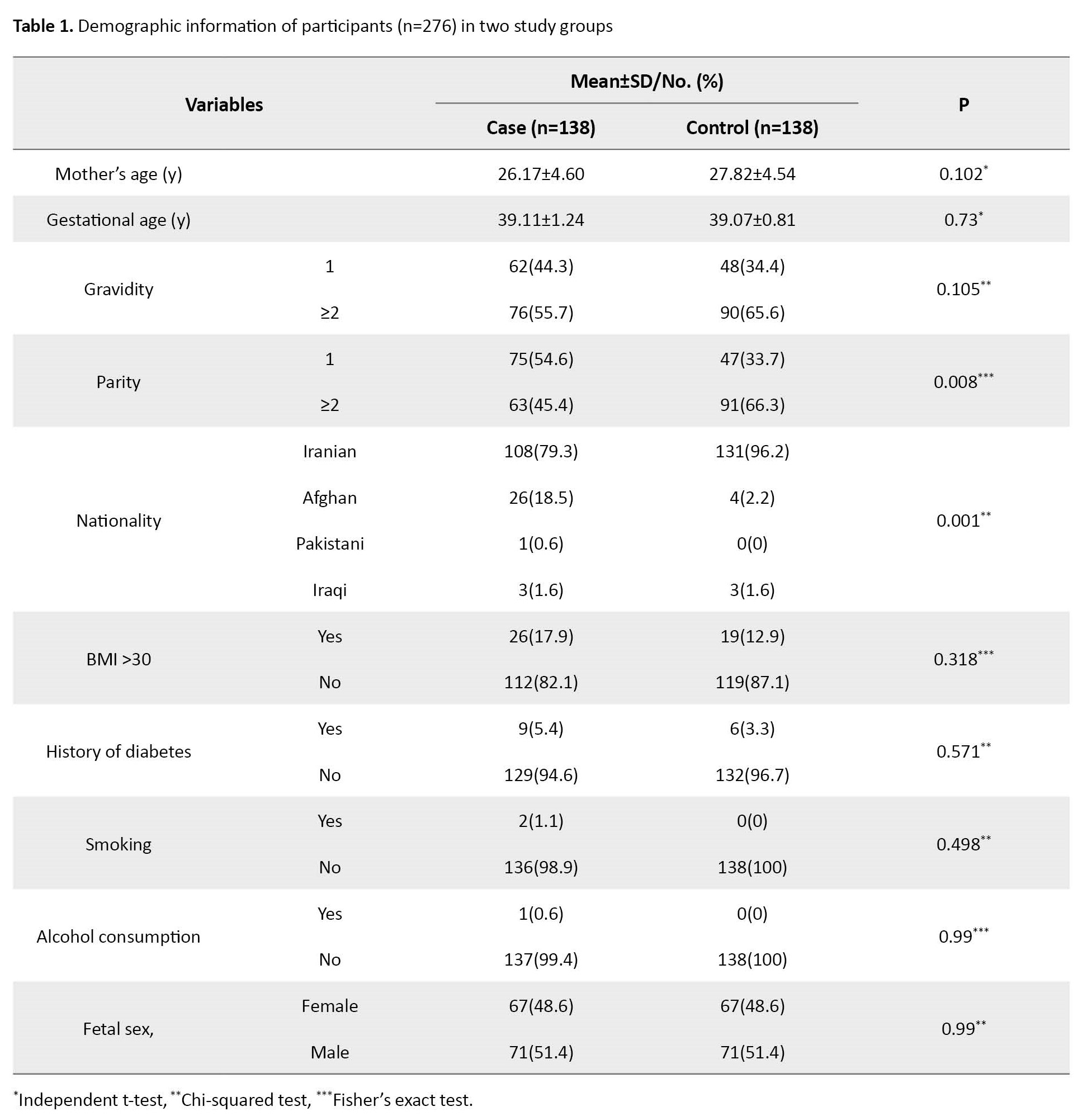
In this study, 276 cases (138 in each group) were examined, whose mean age was 27.00±4.64 years and their gestational age was 39.09±1.05 weeks. None of the mothers consumed alcohol, and only two were smokers. The nationality of most of the mothers (n=239, 71.6%) was Iranian and most of them had male babies (51.4%). Of 138 women with third- and fourth-degree perineal tears, 127 had third-degree tears and 11 had fourth-degree tears. In other words, the prevalence of severe perineal tears was 0.12%, of which 92% was for third-degree tears and 8% was for fourth-degree tears.
There was a statistically significant difference between the two cases and control groups in terms of nationality, such that the number of Afghan mothers in the case group was higher (P=0.001). The prevalence of severe perineal tears in primiparous women was higher than in multiparous women. A small number of women (5.9% in the case group and 3.7% in the control group) were diabetics, and there was no significant difference between the two groups. Moreover, only two women in the case group were smokers, and there was no significant difference between the two groups in this regard. In terms of other demographic variables, including mother’s age, gestational age, number of pregnancies, mother’s BMI, and infant’s sex, there were no significant differences between the two groups, either (Table 1).
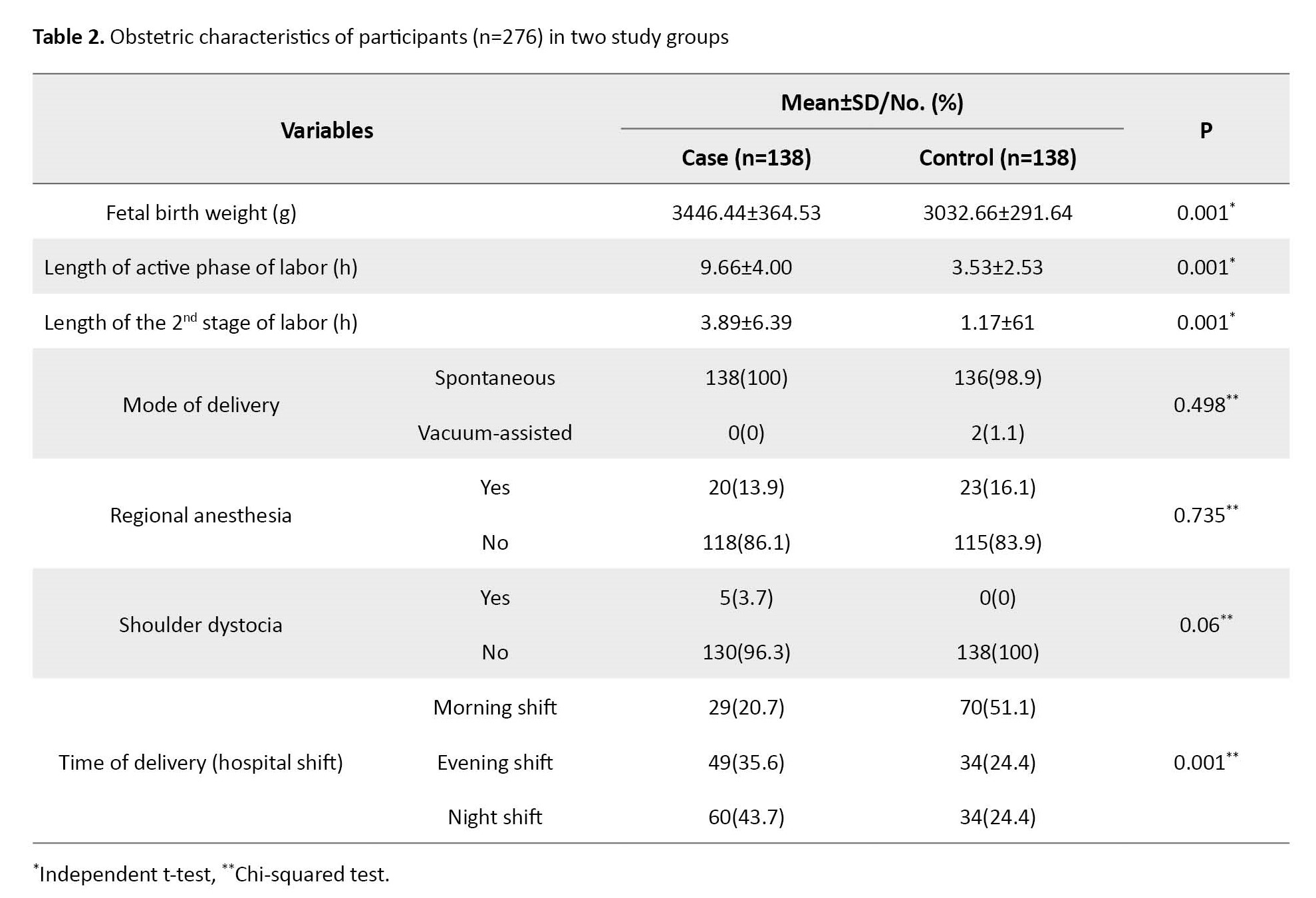
The length of the active phase of the first stage of labor and the length of the second stage of labor in the case group were significantly longer than in the control group (P=0.001). The birth weight of infants in the case group was significantly higher than in the control group (P=0.001). A high number of women in the control group (51.1%) gave birth in the morning shift, while most of the women in the case group (43.7%) gave birth in the night shift, and this difference between the two groups was significant (P=0.001). Since a small number of women had vacuum-assisted delivery and shoulder dystocia during childbirth, there was no significant difference in this regard between the two groups. In terms of regional anesthesia, number of prenatal care visits, oxytocin stimulation, having episiotomy, and suffering from preeclampsia no significant difference was observed between the two groups either (Table 2).
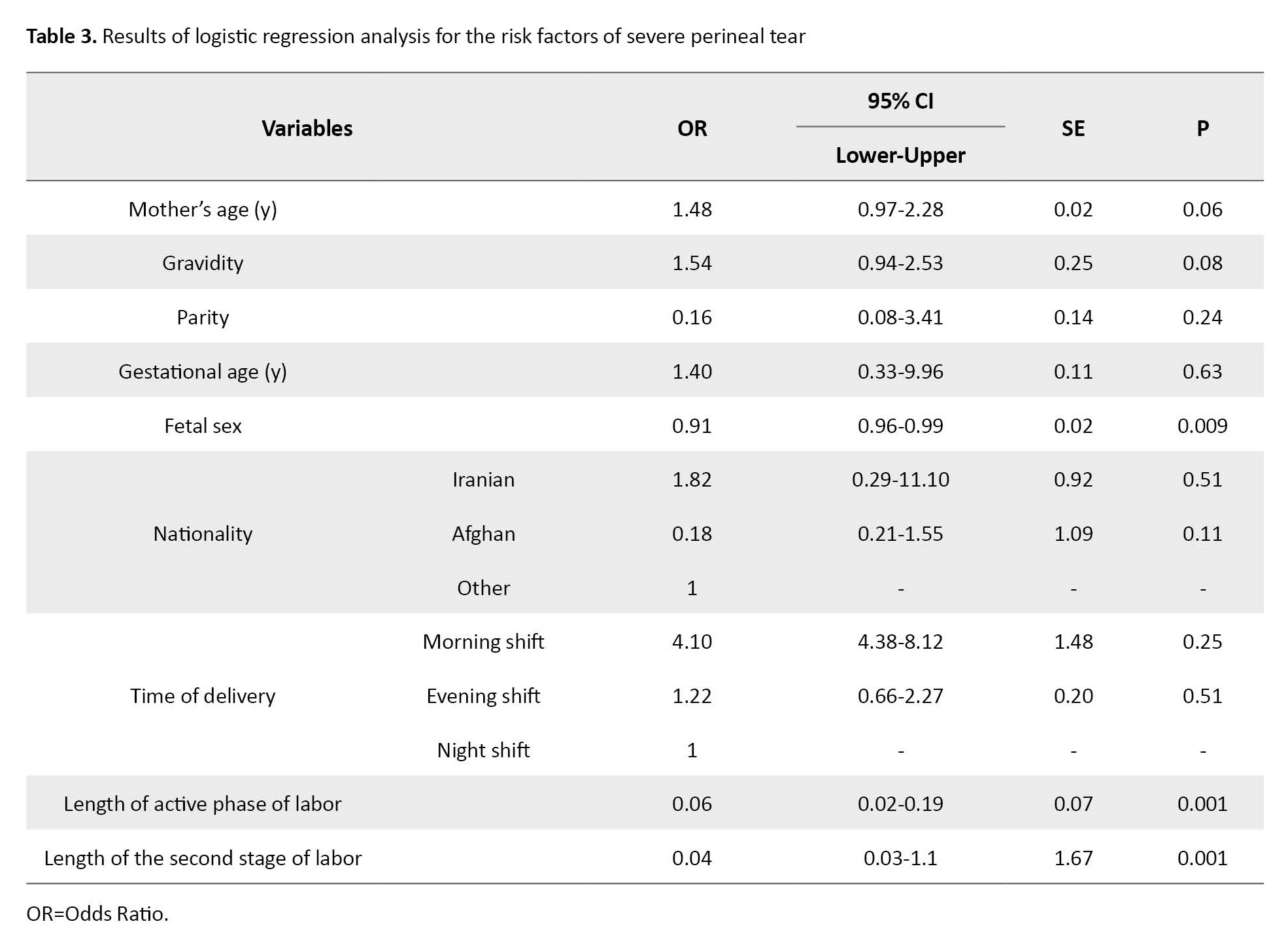
The results of the multivariate logistic regression analysis showed that only the variables of infant’s birth weight (OR=0.91, 95% CI; 0.96%, 0.99%, P=0.009), length of the active phase of labor (OR=0.06, 95% CI; 0.02%, 0.19%, P=0.001) and length of the second stage of labor (OR=0.04, 95% CI; 0.03%-1.1%, P=0.001) were the significant predictors of severe perineal tear (Table 3).
Discussion
The purpose of this study was to determine the prevalence of severe perineal tears during NVD and its risk factors among women in Qom, Iran. The results showed a very low prevalence of severe perineal tears, which is lower than or close to the rates reported in other studies [4, 5, 8, 9]. The prevalence of severe perineal tears can vary significantly based on study population, place, and time [4]. Based on the results of this study, the majority of women who had severe perineal tears were Afghan. In another study conducted in Iran, fourth-degree perineal tears were more common in women with Afghan nationality than those with Iranian nationality, which can be due to less prenatal care of these women or their poor nutritional status and lower standard of living [10]. In some other studies, Asian race was introduced as a risk factor for severe perineal tear [11, 12].
Another factor that was significantly different between the two case and control groups was the parity. In Egbe et al.’s study, that present study was in consistent with them, the rate of severe perineal tears in primipara women was significantly higher than in multipara women. In fact, the elasticity of the perineum in a woman who has never given birth is greater than in women who have had a history of previous childbirth [13]. This can justify the high incidence of severe perineal tears in these women. Abdelhakim et al., in a meta-analysis of 11 clinical trials with 3467 samples, reported that perineal massage in late pregnancy can significantly reduce severe perineal tears during childbirth [14].
In the present study, the length of the first and second stages of labor was also significantly different between the two groups, so that this period of time was longer in the case group than in the control group. Other studies also have reported that the length of the second stage of labor has a significant relationship with the incidence of severe perineal tears [5, 13, 15]. In Loripour et al.’s study, although severe perineal tears were associated with prolongation of the second stage of labor, it had no significant relationship with the length of the first stage of labor [5].
The difference between the two groups was also significant in terms of the birth weight of the newborns, which has been reported as a risk factor in several studies [1, 2, 5, 16, 17]. However, in the studies by Loripour et al. and Ampt et al., the birth weight was not a risk factor for severe perineal tears [5, 18]. This discrepancy may be due to difference in the number of samples. In the current study, the number of women in each case and control group was 138, while in Loripour et al.’s study, there were 32 women in the case group and 129 in the control group.
There was no significant difference between women with and without severe perineal tears in receiving regional anesthesia. The results of a cohort study on 61,308 women also showed that receiving epidural anesthesia during labor was not related to the occurrence of severe perineal tears [19]. In our study, the women with and without severe perineal tears were not different based on their age, which is consistent with other study conducted in Iran [5], but is against the results of other studies [13, 20]. Maybe the reason for this discrepancy is that, unlike the study of Suto et al. [20], most Iranian nulliparous women are not old.
One of the important risk factors for severe perineal tears reported in several studies is shoulder dystocia during childbirth [15, 21, 22]. In our study, women with shoulder dystocia were only in the case group (n=5), and none of the women in the control group had shoulder dystocia. The difference between the two groups was not statistically significant. In most studies, forceps or vacuum-assisted delivery had a significant relationship with severe perineal tears [5, 23, 24]. In the present study, no significant difference was found between the two groups in this factor, which may be due to the small number of assisted deliveries.
There was a significant difference between women with and without severe perineal tears in terms of the time of delivery. A high percentage of women in the control group gave birth in the morning, while a high percentage of women in the case group gave birth in the night. This is probably because the women and the laborers are energetic in the morning but tired or sleepy in the night, which has a considerable effect on the occurrence of perineal tears. The studies conducted in four hospitals in the United States [25] and on neonatal intensive care unit workers [26], as well as the results of a review study [27] showed that working night shifts can cause fatigue in staff and reduce their efficiency.
One of the strengths of the present study is the examination of a large number of births during 8 years and a comprehensive examination of the information of cases recorded in the medical files. One of the limitations of the present study was that the information in some medical files was incomplete. Therefore, it is recommended to conduct a prospective cohort study for a more detailed investigation of the risk factors for severe perineal tears in Iran.
According to the results of this study, the high birth weight of newborns and the prolongation of the first and second stages of labor are the risk factors predicting the occurrence of severe perineal tears. Therefore, paying attention to these risk factors and being aware of them can help prevent the occurrence of severe perineal tears with appropriate and timely interventions.
Ethical Considerations
Compliance with ethical guidelines
The study was approved by the Ethics Committee of Qom University of Medical Sciences (Code: IR.MUQ.REC.1399.208). Informed consent was obtained from all participants, and they were assured of the confidentiality of their information.
Funding
This article was extracted from a medical thesis of Mohammad hassan Sharifi, approved by Zohre Khalajinia and Roghayyeh Ahangariapproved by the ethics committee of Qom University of Medical Sciences.
Authors' contributions
Conceptualization and study design: Zohre Khalajinia, Roghayyeh Ahangari, Fatemeh Sadat Mousavi; Data collection: Mohammad Hassan Sharifi; Data analysis and data interpretation: Mostafa Vahedian, Drafting the manuscript: Fatemeh Sadat Mousavi, Zohre Khalajinia and Mohammad Hassan Sharifi; Review and final approval of manuscript: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors would like to thank the officials of teaching hospitals in Qom for allowing us access to the patient data.
References
Perineal tear during childbirth is common and may be caused by episiotomy and/or spontaneous tear of the perineum [1]. Perineum tears are classified into four degrees. First- and second-degree tears involve injury to only the vaginal mucosa and perineal muscles (mild). Third- and fourth-degree tears involve injury to the anal sphincter and the rectal mucosa, respectively (severe) [2]. More than 85% of women during normal vaginal delivery (NVD) experience some kind of perineal tears during the passage of the baby through the vagina, most of which are mild tears [3]. Mild perineal tears are very common and have been reported to occur in 73% of primiparous deliveries. Severe perineal tears are much less common. Reported prevalence rates vary from 0.1 to 8% in different populations. In some countries, a significant increase has been recorded in the last three decades [4]. In Iran, the prevalence of third- and fourth-degree perineal tears is in a range from 0.16% to 0.36% [5]. Anal sphincter injury occurs only in severe perineal tears, which cause significant complications compared to first- or second-degree perineal tears. Abscess formation, wound rupture, rectovaginal fistula (an abnormal connection between the rectum and vagina), and fecal incontinence have been reported following anal sphincter injury. Failure to properly treat such injuries may cause both short-term and long-term complications, including urinary and fecal incontinence, bleeding, infection, pain, painful intercourse, sexual dysfunction, and reduced quality of life [1]. Anal sphincter injury is one of the most common complaints in medical court cases, which causes tension for the patient and those involved in childbirth [6]. Despite the mentioned complications, there is no agreement on preventive measures and clinical management of severe perineal tears. Identifying the risk factors of these tears can help in their prevention. For this reason, clinical guidelines emphasize the importance of knowing the factors contributing to severe perineal tears. However, there is conflicting information about the importance of obstetric factors causing these tears [5].
The factors mentioned in the literature are Asian race, being prime par, mother’s age, persistent occiput posterior, prolongation of the second phase of labor, high birth weight, labor induction with oxytocin, low work experience of the laborer, gestational diabetes, passing the due date of delivery, delivery with vacuum, and episiotomy [1, 3-5, 7]. Since the studies conducted in this field are limited, especially in Iran, this study was conducted to determine the prevalence of severe perineal tears during NVD in Qom, Iran, and find its risk factors.
Materials and Methods
This is a descriptive-analytical, retrospective study with a case-control design, which was conducted on the medical records of women who gave birth from March 2010 to March 2019 in three teaching hospitals in Qom. Inclusion criteria included singleton pregnancy with cephalic presentation and gestational age greater than 20 weeks (or fetal weight greater than 500 g when gestational age is unknown). Incomplete files and the data of mothers with cesarean section were excluded. Information was collected using a checklist surveying demographic information, previous medical history, and obstetric information. The extracted information included mother’s age, mother’s history of illness, mother’s body mass index (BMI), gestational age, gravidity, parity, type of perineal tear, type of spinal anesthesia, use/non-use of narcotic drugs for pain relief, length of the active phase of the first stage of labor, length of the second stage of labor, length of hospitalization until delivery, length of water breaking, having/not having an episiotomy, position of the fetus during delivery (occiput posterior or occiput anterior), use of oxytocin to induce labor, mode of delivery, instrumental delivery, occurrence/not occurrence of shoulder dystocia, and race, weight and sex of the newborn.
After the approval of the ethics committee of Qom University of Medical Sciences and obtaining permission from the hospital managers, the vaginal delivery registration system of the hospitals was checked. Then, cases of third- and fourth-degree perineal tears were searched, their clinical files were examined, and their information was extracted. Considering that among the 115,107 births performed in these hospitals, 138 cases had third- and fourth-degree tears, the same number of cases of women with no severe tears were randomly selected based on the inclusion criteria. Finally, there were 138 women in each case and control group (Figure 1).
Results
In this study, 276 cases (138 in each group) were examined, whose mean age was 27.00±4.64 years and their gestational age was 39.09±1.05 weeks. None of the mothers consumed alcohol, and only two were smokers. The nationality of most of the mothers (n=239, 71.6%) was Iranian and most of them had male babies (51.4%). Of 138 women with third- and fourth-degree perineal tears, 127 had third-degree tears and 11 had fourth-degree tears. In other words, the prevalence of severe perineal tears was 0.12%, of which 92% was for third-degree tears and 8% was for fourth-degree tears.
There was a statistically significant difference between the two cases and control groups in terms of nationality, such that the number of Afghan mothers in the case group was higher (P=0.001). The prevalence of severe perineal tears in primiparous women was higher than in multiparous women. A small number of women (5.9% in the case group and 3.7% in the control group) were diabetics, and there was no significant difference between the two groups. Moreover, only two women in the case group were smokers, and there was no significant difference between the two groups in this regard. In terms of other demographic variables, including mother’s age, gestational age, number of pregnancies, mother’s BMI, and infant’s sex, there were no significant differences between the two groups, either (Table 1).
The length of the active phase of the first stage of labor and the length of the second stage of labor in the case group were significantly longer than in the control group (P=0.001). The birth weight of infants in the case group was significantly higher than in the control group (P=0.001). A high number of women in the control group (51.1%) gave birth in the morning shift, while most of the women in the case group (43.7%) gave birth in the night shift, and this difference between the two groups was significant (P=0.001). Since a small number of women had vacuum-assisted delivery and shoulder dystocia during childbirth, there was no significant difference in this regard between the two groups. In terms of regional anesthesia, number of prenatal care visits, oxytocin stimulation, having episiotomy, and suffering from preeclampsia no significant difference was observed between the two groups either (Table 2).
The results of the multivariate logistic regression analysis showed that only the variables of infant’s birth weight (OR=0.91, 95% CI; 0.96%, 0.99%, P=0.009), length of the active phase of labor (OR=0.06, 95% CI; 0.02%, 0.19%, P=0.001) and length of the second stage of labor (OR=0.04, 95% CI; 0.03%-1.1%, P=0.001) were the significant predictors of severe perineal tear (Table 3).
Discussion
The purpose of this study was to determine the prevalence of severe perineal tears during NVD and its risk factors among women in Qom, Iran. The results showed a very low prevalence of severe perineal tears, which is lower than or close to the rates reported in other studies [4, 5, 8, 9]. The prevalence of severe perineal tears can vary significantly based on study population, place, and time [4]. Based on the results of this study, the majority of women who had severe perineal tears were Afghan. In another study conducted in Iran, fourth-degree perineal tears were more common in women with Afghan nationality than those with Iranian nationality, which can be due to less prenatal care of these women or their poor nutritional status and lower standard of living [10]. In some other studies, Asian race was introduced as a risk factor for severe perineal tear [11, 12].
Another factor that was significantly different between the two case and control groups was the parity. In Egbe et al.’s study, that present study was in consistent with them, the rate of severe perineal tears in primipara women was significantly higher than in multipara women. In fact, the elasticity of the perineum in a woman who has never given birth is greater than in women who have had a history of previous childbirth [13]. This can justify the high incidence of severe perineal tears in these women. Abdelhakim et al., in a meta-analysis of 11 clinical trials with 3467 samples, reported that perineal massage in late pregnancy can significantly reduce severe perineal tears during childbirth [14].
In the present study, the length of the first and second stages of labor was also significantly different between the two groups, so that this period of time was longer in the case group than in the control group. Other studies also have reported that the length of the second stage of labor has a significant relationship with the incidence of severe perineal tears [5, 13, 15]. In Loripour et al.’s study, although severe perineal tears were associated with prolongation of the second stage of labor, it had no significant relationship with the length of the first stage of labor [5].
The difference between the two groups was also significant in terms of the birth weight of the newborns, which has been reported as a risk factor in several studies [1, 2, 5, 16, 17]. However, in the studies by Loripour et al. and Ampt et al., the birth weight was not a risk factor for severe perineal tears [5, 18]. This discrepancy may be due to difference in the number of samples. In the current study, the number of women in each case and control group was 138, while in Loripour et al.’s study, there were 32 women in the case group and 129 in the control group.
There was no significant difference between women with and without severe perineal tears in receiving regional anesthesia. The results of a cohort study on 61,308 women also showed that receiving epidural anesthesia during labor was not related to the occurrence of severe perineal tears [19]. In our study, the women with and without severe perineal tears were not different based on their age, which is consistent with other study conducted in Iran [5], but is against the results of other studies [13, 20]. Maybe the reason for this discrepancy is that, unlike the study of Suto et al. [20], most Iranian nulliparous women are not old.
One of the important risk factors for severe perineal tears reported in several studies is shoulder dystocia during childbirth [15, 21, 22]. In our study, women with shoulder dystocia were only in the case group (n=5), and none of the women in the control group had shoulder dystocia. The difference between the two groups was not statistically significant. In most studies, forceps or vacuum-assisted delivery had a significant relationship with severe perineal tears [5, 23, 24]. In the present study, no significant difference was found between the two groups in this factor, which may be due to the small number of assisted deliveries.
There was a significant difference between women with and without severe perineal tears in terms of the time of delivery. A high percentage of women in the control group gave birth in the morning, while a high percentage of women in the case group gave birth in the night. This is probably because the women and the laborers are energetic in the morning but tired or sleepy in the night, which has a considerable effect on the occurrence of perineal tears. The studies conducted in four hospitals in the United States [25] and on neonatal intensive care unit workers [26], as well as the results of a review study [27] showed that working night shifts can cause fatigue in staff and reduce their efficiency.
One of the strengths of the present study is the examination of a large number of births during 8 years and a comprehensive examination of the information of cases recorded in the medical files. One of the limitations of the present study was that the information in some medical files was incomplete. Therefore, it is recommended to conduct a prospective cohort study for a more detailed investigation of the risk factors for severe perineal tears in Iran.
According to the results of this study, the high birth weight of newborns and the prolongation of the first and second stages of labor are the risk factors predicting the occurrence of severe perineal tears. Therefore, paying attention to these risk factors and being aware of them can help prevent the occurrence of severe perineal tears with appropriate and timely interventions.
Ethical Considerations
Compliance with ethical guidelines
The study was approved by the Ethics Committee of Qom University of Medical Sciences (Code: IR.MUQ.REC.1399.208). Informed consent was obtained from all participants, and they were assured of the confidentiality of their information.
Funding
This article was extracted from a medical thesis of Mohammad hassan Sharifi, approved by Zohre Khalajinia and Roghayyeh Ahangariapproved by the ethics committee of Qom University of Medical Sciences.
Authors' contributions
Conceptualization and study design: Zohre Khalajinia, Roghayyeh Ahangari, Fatemeh Sadat Mousavi; Data collection: Mohammad Hassan Sharifi; Data analysis and data interpretation: Mostafa Vahedian, Drafting the manuscript: Fatemeh Sadat Mousavi, Zohre Khalajinia and Mohammad Hassan Sharifi; Review and final approval of manuscript: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors would like to thank the officials of teaching hospitals in Qom for allowing us access to the patient data.
References
- Jahani Shourab N, Mirteimouri M, Latifnejad Roudsari R. [A case series of severe perineal lacerations during normal childbirth (Persian)]. Iran J Obstet Gynecol Infertil. 2018; 21(8):103-14. [Link]
- von Theobald P, Bohrer M, Lorrain S, Iacobelli S. Risk factors associated with severe perineal tears: A five-year study. J Gynecol Obstet Hum Reprod. 2020; 49(7):101820. [DOI:10.1016/j.jogoh.2020.101820] [PMID]
- Lopes GA, Leister N, Riesco MLG. Perineal care and outcomes in a birth center. TextoContexto-Enfermagem. 2019; 28. [DOI:10.1590/1980-265X-TCE-2018-0168]
- Groutz A, Hasson J, Wengier A, Gold R, Skornick-Rapaport A, Lessing JB, et al. Third-and fourth-degree perineal tears: prevalence and risk factors in the third millennium. Am J Obstet Gynecol. 2011; 204(4):347.e1-4. [DOI:10.1016/j.ajog.2010.11.019] [PMID]
- Loripour M, Najar Mohiabadi M, Allahbakhshi Nasab P, Sayadi A. [Prevalence of third and fourth degree of perineal lacerations during vaginal delivery and some related factors in Nik Nafs maternity of Rafsanjan in 2015-2017 (Persian)]. Iran J Obstet Gynecol Infertil. 2021; 24(6):10-6. [DOI:10.22038/IJOGI.2021.18733]
- Keriakos R, Gopinath D. Obstetric anal sphincter injuries. J Acute Dis. 2015; 4(4):259-65. [DOI:10.1016/j.joad.2015.04.014]
- Pergialiotis V, Bellos I, Fanaki M, Vrachnis N, Doumouchtsis SK. Risk factors for severe perineal trauma during childbirth: An updated meta-analysis. Eur J Obstet Gynecol Reprod Biol. 2020; 247:94-100. [DOI:10.1016/j.ejogrb.2020.02.025] [PMID]
- Nóbrega MA, Pereira GMV, Brito LGO, Luz AG, Lajos GJ. Severe perineal trauma in a Brazilian southeastern tertiary hospital: A retrospective cohort study. Female Pelvic Med Reconstr Surg. 2021; 27(2):e301-e5. [DOI:10.1097/SPV.0000000000000910] [PMID]
- Sánchez-Ávila MT, Galván-Caudillo M, Cantú-Pompa JJ, Vázquez-Romero N, Martínez-López JP, Matías-Barrios VM, et al. Prevalence of high-grade perineal tear during labor in Mexican adolescents.Colomb Med (Cali). 2018; 49(4):261-4. [DOI:10.25100/cm.v49i4.3515] [PMID]
- Zafarghandi N, Hadavand S, Zayeri F, Hamzeloo L. [Risk factors associated with forth-degree laceration during vaginal delivery (Persian)]. Tehran Univ Med J. 2006; 64(7):65-74. [Link]
- Mandelbaum A, Doshi U, Chaiken SR, Garg B, Katlaps I, Caughey AB. Influence of race/ethnicity on maternal outcomes among nulliparous patients undergoing operative vaginal delivery. Am J Obstet Gynecol. 2023; 228(1):S610. [DOI:10.1016/j.ajog.2022.11.1035]
- Albar M, Aviram A, Anabusi S, Huang T, Tunde-Byass M, Mei-Dan E. Maternal ethnicity and the risk of obstetrical anal sphincter injury: A retrospective cohort study. J Obstet Gynaecol Can. 2021; 43(4):469-73. [DOI:10.1016/j.jogc.2020.08.016] [PMID]
- Egbe T, Kadzem L, Takang W, Tchounzou R, Egbe E, Mbu R. Prevalence and risk factors of perineal tears at the limbe regional hospital, cameroon. Int J Reprod Fertil Sex Health. 2016; 3(3):70-8. [DOI:10.19070/2377-1887-1600013]
- Abdelhakim AM, Eldesouky E, Elmagd IA, Mohammed A, Farag EA, Mohammed AE, et al. Antenatal perineal massage benefits in reducing perineal trauma and postpartum morbidities: A systematic review and meta-analysis of randomized controlled trials. Int Urogynecol J. 2020; 31(9):1735-45. [DOI:10.1007/s00192-020-04302-8] [PMID]
- Simic M, Cnattingius S, Petersson G, Sandström A, Stephansson O. Duration of second stage of labor and instrumental delivery as risk factors for severe perineal lacerations: Population-based study. BMC Pregnancy Childbirth. 2017; 17(1):72. [DOI:10.1186/s12884-017-1251-6] [PMID]
- Frigerio M, Manodoro S, Bernasconi DP, Verri D, Milani R, Vergani P. Incidence and risk factors of third-and fourth-degree perineal tears in a single Italian scenario. Eur J Obstet Gynecol Reprod Biol. 2018; 221:139-43. [DOI:10.1016/j.ejogrb.2017.12.042] [PMID]
- Wilson AN, Homer CSE. Third-and fourth-degree tears: A review of the current evidence for prevention and management. Aust N Z J Obstet Gynaecol. 2020; 60(2):175-82. [DOI:10.1111/ajo.13127] [PMID]
- Ampt AJ, Ford JB, Roberts CL, Morris JM. Trends in obstetric anal sphincter injuries and associated risk factors for vaginal singleton term births in New South Wales 2001-2009. Aust N Z J Obstet Gynaecol. 2013; 53(1):9-16. [DOI:10.1111/ajo.12038] [PMID]
- Loewenberg-Weisband Y, Grisaru-Granovsky S, Ioscovich A, Samueloff A, Calderon-Margalit R. Epidural analgesia and severe perineal tears: A literature review and large cohort study. J Matern Fetal Neonatal Med. 2014; 27(18):1864-9. [DOI:10.3109/14767058.2014.889113] [PMID]
- Suto M, Takehara K, Misago C, Matsui M. Prevalence of perineal lacerations in women giving birth at midwife-led birth centers in Japan: A retrospective descriptive study. J Midwifery Womens Health. 2015; 60(4):419-27. [DOI:10.1111/jmwh.12324] [PMID]
- Gurol-Urganci I, Cromwell DA, Edozien LC, Mahmood TA, Adams EJ, Richmond DH, et al. Third-and fourth-degree perineal tears among primiparous women in England between 2000 and 2012: Time trends and risk factors. BJOG. 2013; 120(12):1516-25. [DOI:10.1111/1471-0528.12363] [PMID]
- Hehir MP, Rubeo Z, Flood K, Mardy AH, O'Herlihy C, Boylan PC, et al. Anal sphincter injury in vaginal deliveries complicated by shoulder dystocia. Int Urogynecol J. 2018; 29(3):377-81. [DOI:10.1007/s00192-017-3351-2] [PMID]
- Barca JA, Bravo C, Pintado-Recarte MP, Cueto-Hernández I, Ruiz-Labarta J, Cuñarro Y, et al. Risk factors in third and fourth degree perineal tears in women in a tertiary centre: An observational ambispective cohort study. J Pers Med. 2021; 11(8):685. [DOI:10.3390/jpm11080685] [PMID]
- Gommesen D, Nohr EA, Drue HC, Qvist N, Rasch V. Obstetric perineal tears: Risk Factors, wound infection and dehiscence: A prospective cohort study. Arch Gynecol Obstet. 2019; 300(1):67-77. [DOI:10.1007/s00404-019-05165-1] [PMID]
- McElroy SF, Olney A, Hunt C, Glennon C. Shift work and hospital employees: A descriptive multi-site study. Int J Nurs Stud. 2020; 112:103746. [DOI:10.1016/j.ijnurstu.2020.103746] [PMID]
- Anvekar AP, Nathan EA, Doherty DA, Patole SK. Effect of shift work on fatigue and sleep in neonatal registrars. Plos One. 2021; 16(1):e0245428. [DOI:10.1371/journal.pone.0245428] [PMID]
- Alahmadi BA, Alharbi MF. Work-related fatigue factors among hospital nurses: An integrative literature review. Nurse Media J Nurs. 2018; 8(2):113-33. [DOI:10.14710/nmjn.v8i2.19554]
Article Type : Research |
Subject:
General
Received: 2024/02/24 | Accepted: 2024/02/21 | Published: 2024/02/21
Received: 2024/02/24 | Accepted: 2024/02/21 | Published: 2024/02/21
Send email to the article author
| Rights and permissions | |
 | This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Articles Copyright © The Author(s).
Owned by Guilan University of Medical Sciences.
Co-published by Negah Institute for Scientific Communication.
Contact Information
JHNM Office, Guilan University of Medical Sciences P.O.Box 41635-1873, Rasht, Iran
Journal Tel: +9813 33553202
Publisher Tel: +9821 453 55 555; +9821 453 55 000
Email: holisticnmj@gmail.com, nursjournal@gums.ac.ir
