Sun, Apr 28, 2024
Volume 34, Issue 2 (2-2024)
JHNM 2024, 34(2): 107-116 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Ghorbani S, Salehin S, Nazari A M, Talebi S, Keramat A. Effect of Existential Group Therapy on Infertility Stress in Infertile Men’s Spouses. JHNM 2024; 34 (2) :107-116
URL: http://hnmj.gums.ac.ir/article-1-2303-en.html
URL: http://hnmj.gums.ac.ir/article-1-2303-en.html



1- Midwifery (MSc), Student Research Committee, School of Nursing and Midwifery, Shahroud University of Medical Sciences, Shahroud, Iran.
2- Assistant Professor, Sexual Health and Fertility Research Center, Shahroud University of Medical Sciences, Shahroud, Iran. , drbsalehin@gmail.com
3- Associate Professor, Department of Counseling, School of Nursing and Midwifery, Shahroud University of Medical Sciences, Shahroud, Iran.
4- Assistant Professor, Department of Epidemiology, School of Public Health, Shahroud University of Medical Sciences, Shahroud, Iran.
5- Professor, Center for Health Related Social and Behavioral Sciences Research, Shahroud University of Medical Sciences, Shahroud, Iran.
2- Assistant Professor, Sexual Health and Fertility Research Center, Shahroud University of Medical Sciences, Shahroud, Iran. , drbsalehin@gmail.com
3- Associate Professor, Department of Counseling, School of Nursing and Midwifery, Shahroud University of Medical Sciences, Shahroud, Iran.
4- Assistant Professor, Department of Epidemiology, School of Public Health, Shahroud University of Medical Sciences, Shahroud, Iran.
5- Professor, Center for Health Related Social and Behavioral Sciences Research, Shahroud University of Medical Sciences, Shahroud, Iran.
Full-Text [PDF 558 kb]
(133 Downloads)
| Abstract (HTML) (247 Views)
Full-Text: (60 Views)
Introduction
Infertility is a pregnancy failure after one year of regular unprotected intercourse [1]. Infertility is a common disorder all around the world, and the disorder has been even increasing in most parts of the world in recent years [2]. Studies show that about 50 to 80 million people worldwide experience some form of infertility [3]. A recent study estimated that the overall prevalence of infertility in Iran is 7.88% [4].
Infertility can be the worst experience in a couple’s life, so infertile women often consider infertility the most stressful event in their lives and describe frequent and successive courses of treatment as repeated periods of crisis [5]. Infertility is regarded as a crisis in a couple’s life with many psychological consequences [6]. In all cultures worldwide, infertility has been known as a stressful individual, marital, family, and social experience, threatening marriage stability [7].
Infertility stress comprises a set of symptoms revealed in individuals when diagnosed with infertility [8]. Infertility stress appears as a combination of five components: Social concerns, sexual concerns, communication concerns, the need to be a parent, and not accepting a child-free lifestyle [9, 10]. After the death of first-degree family members and the stress of divorce, infertility and its treatment have the most stress level for individuals [11].
A study showed that infertile men’s spouses are as stressed as infertile women in many areas because women are more engaged with diagnostic and therapeutic procedures, even in male-induced infertility [12]. Women experience more concerns than their husbands. When women’s husbands are infertile, they experience reactions such as anxiety, stress, depression, and sadness. These women are stressed due to losing the ability to become mothers [13, 14].
In most cultures, women are considered to be responsible for not having children. Men evade their responsibilities, which worsens marital problems. According to previous studies, the stressful experience of infertility can be associated with a wide range of psychological disorders, such as decreased self-esteem; increased stress, anxiety, depression, and anger; inefficiency feelings; marital problems; and cognitive and emotional problems [15, 16]. It is also noteworthy that lower stress levels are associated with higher marital quality [17].
Existential group therapy is a psychological intervention focusing on free will, autonomy, and the search for meaning. This treatment concentrates on the individual rather than the symptoms and emphasizes the capacity to make rational choices and maximize this ability [18]. Instead of depriving an individual of authority, existential group therapy emphasizes the patient-therapist relationship, honest confrontation, and change as a courageous action. Although patients cannot change the bitter events of life, this group helps them change their analysis, thinking, and perception [19]. This therapeutic approach allows individuals to search for meaning, have a purpose, and create a positive relationship with psychological factors. It gives them more adaptation ability, life satisfaction, and psychological well-being [20]. The effectiveness of this method has been confirmed in various cases [21]. In a study, existential psychotherapy increased resilience in women with infertility [22]. Group therapy helps people recognize their strengths and weaknesses, identify their values and beliefs, compare them with others, improve them, and focus on current relationships instead of external problems [23, 24]. As a dynamic method, existential group therapy emphasizes understanding four basic issues: Death, freedom, loneliness, and meaninglessness [25]. This therapy helps people realize the meaning of their lives, be responsible, and profit from opportunities [26].
Considering the importance of infertility stress in the lives of infertile men’s wives, this study was conducted to investigate the effect of existential group therapy on infertility stress in the wives of infertile men.
Materials and Methods
The present study is a randomized clinical trial with two study groups: A counseling existential therapy group and a control group. It was conducted from August 2021 to March 2022. The research population of the study included women aged 20 to 45 who were accompanying their infertile husbands. They had moderate and high infertility stress and were referred to infertility clinics in Shahrood City, Iran.
To estimate the sample size, we used the following parameters in a similar study [27] as follows: The standard deviation of the first community was 13.2, the Standard deviation of the second community was 8, the mean difference between the two communities is 11.4 at a 95% confidence interval, and considering a test power of 80%. The sample size was then estimated at 43 participants, and 10% was added for dropout. Finally, 48 women participated in the intervention and 48 women in the control group (96 participants in total).
Ninety-six women who met all the inclusion criteria participated in the study after taking informed consent. The inclusion criteria were as follows: Willing to participate in research, being 20 to 45 years old, having infertility with male factor only, lacking children from a previous marriage, having at least primary education, lacking psychiatric disorders, not being a divorced applicant, and lacking sexual dysfunction in the wife of the husband. The exclusion criteria were as follows: Getting pregnant during the study, reluctance to attend the meetings for any reason, failure to complete the questionnaires, and more than two absences from the counseling sessions.
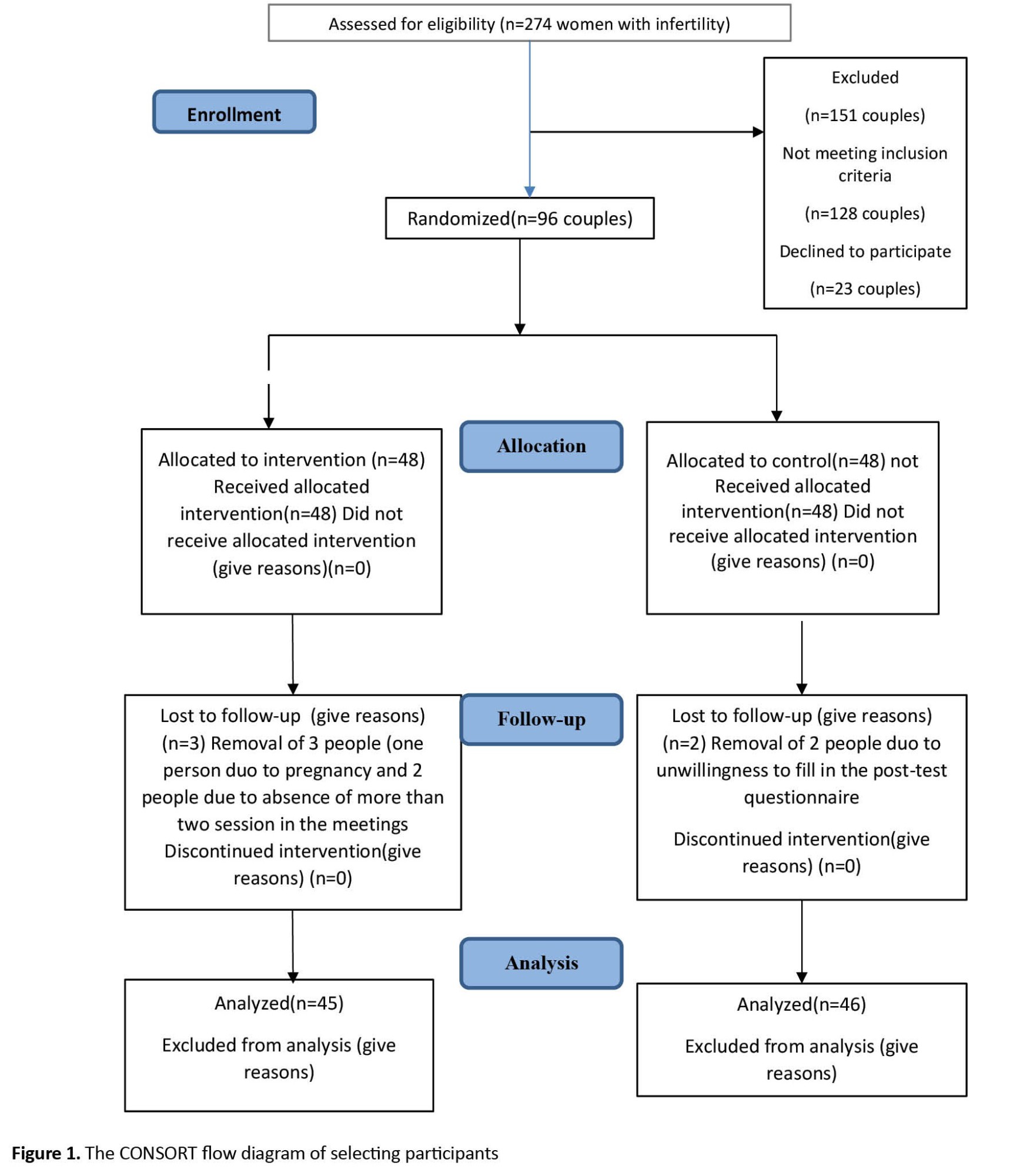
The study subjects were selected from women with a history of primary infertility and male infertility referred to the infertility center. We used a random sampling method for selecting cases and a random block in size 4 for allocation. The women of the intervention group were divided by chance into six sub-groups of 6 women each, receiving the same existential group therapy separately (eight sessions for each sub-group). The sessions were held virtually (due to the conditions of the COVID-19 pandemic). The control group did not receive any intervention other than routine follow-up of the infertility center. Figure 1 shows the process of conducting the study in summary.
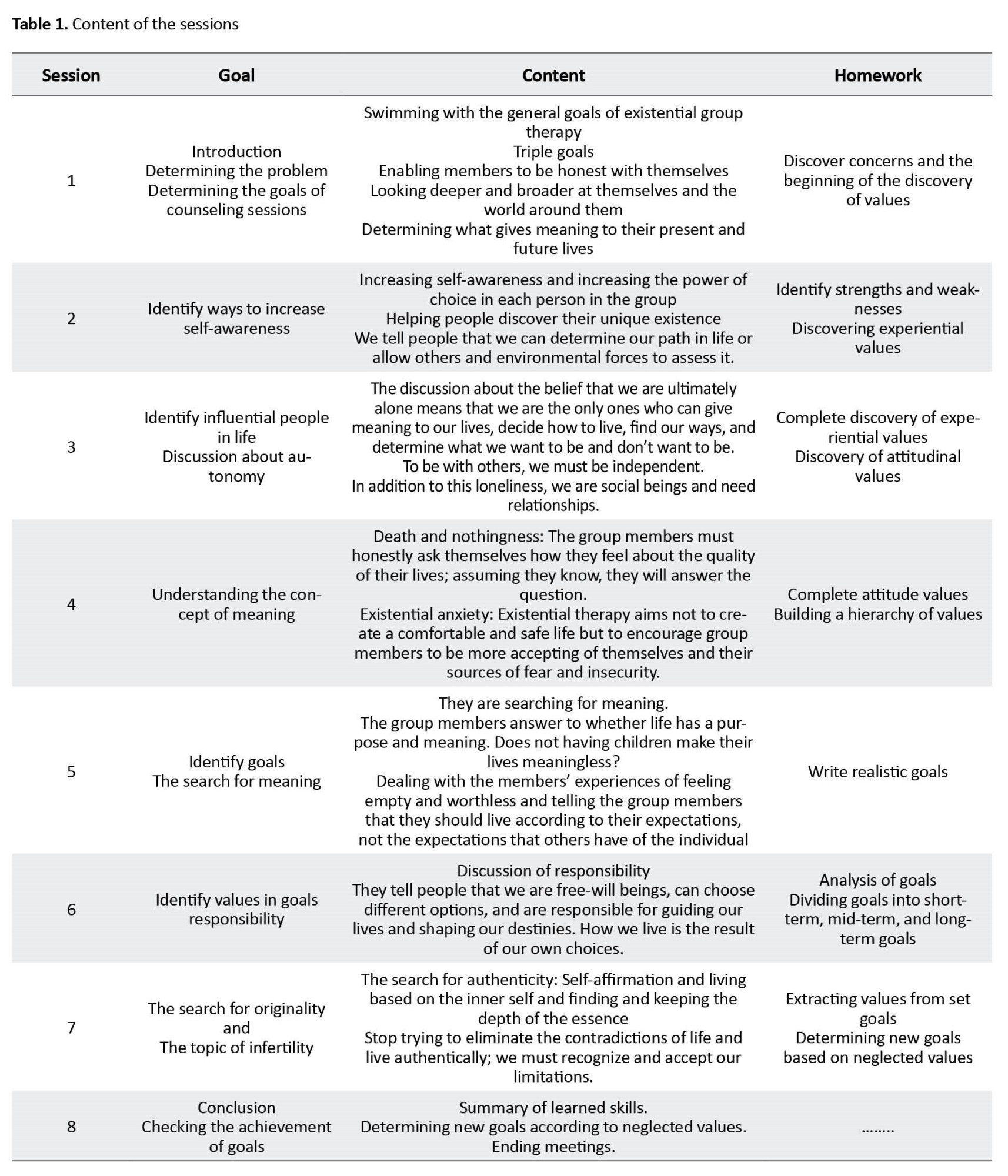
 Existential group therapy was held for the intervention group in 8 sessions [18]. Table 1 presents a summary of the content of the meetings.
Existential group therapy was held for the intervention group in 8 sessions [18]. Table 1 presents a summary of the content of the meetings.
The data collection tools for conducting this study were a demographic information questionnaire and an infertility stress questionnaire, previously designed by Newton et al. [28]. This questionnaire has 46 questions with 5 subscales: Social concerns, sexual concerns, communication concerns, childless lifestyle, and the need to be a parent. It measures the stress of infertility based on a 6-point rating scale ranging from “1” (strongly disagree) to “6” (strongly agree) with questions such as (when I’m asked about children, I don’t get upset). Considering that a high score in general stress indicates high stress in infertility, some questions are scored in reverse. The total stress level is calculated by adding all the raw scores in all five scales. The maximum score for the 10-question scale is 60, the minimum is 10, the 8-question scale is 48, and the minimum is 8. The maximum total score is 276, and the minimum is 46. Generally, a high score indicates high infertility stress.
Samani’s research confirmed the reliability of Newton’s infertility stress questionnaire in Iran [29].
The purpose of the study was explained to participants, who were included in the study after providing written informed consent. The electronically designed questionnaires were completed before the intervention and a week after the counseling sessions’ end by the intervention and control groups. The control group received routine treatment during existential group therapy for participants in the intervention group. A summary of the consultation sessions was given to the control group to observe the ethical aspects after the post-test. After completing the questionnaires, the collected information was entered into SPSS software, version 25 and subjected to statistical analysis. The normality of data was assessed using the Kolmogorov-Smirnov test. The data were analyzed by the chi-square test, Fisher exact test, and compare means t-test. A comparison of the groups was performed using the independent t-test. A comparison of stress scores before and after the intervention within each group was performed using the paired t-test.
Results
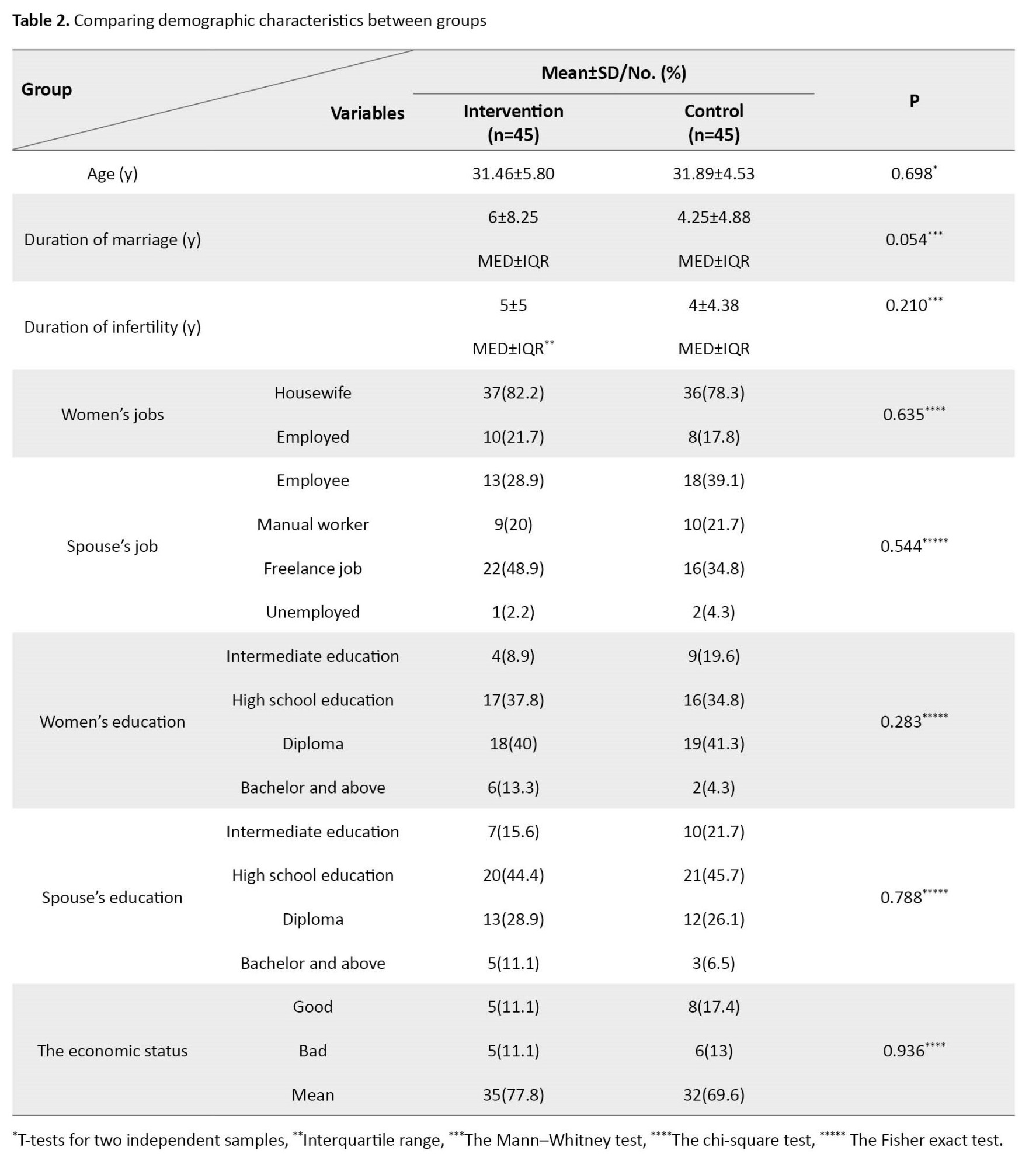
The Mean±SD of the age of the participants in the whole population is 31.68±5.17 years. In comparing the two study groups, their mean age was comparable. Of the total participants, 73 female participants (80.2%) were housewives. The participants’ percentages of employee, laborer, self-employed, and unemployed jobs were 34.1%, 20.9%, 41.8%, and 3.3%, respectively. The women’s education percentages of middle school education, diploma and post-diploma, bachelor’s and master’s degrees, and above were 14.28%, 36.28%, 40.65%, and 8.79%, respectively. The spouse's percentages of education, diploma and post-diploma, bachelor’s and master’s degree and above are 18.68%, 45.05%, 27.47%, and 8.79%, respectively. The spouse’s percentages of good, bad, and average economic status were 14.3%, 12.1%, and 73.6%, respectively. The chi-square test, Fisher exact test, and compare means t-test showed that the age, job, education, economic status, time of marriage, and duration of infertility were homogenous between the two groups. The median and interquartile range of the participants’ marriage duration in the entire population was 5. Based on the comparison test of the median of two independent societies, the duration of marriage is homogeneous in the two groups.
The median (interquartile range) of the participants’ infertility duration in the entire population is 4. Based on the comparison test of the median of two independent societies, the duration of marriage is homogeneous in two groups (Table 2).
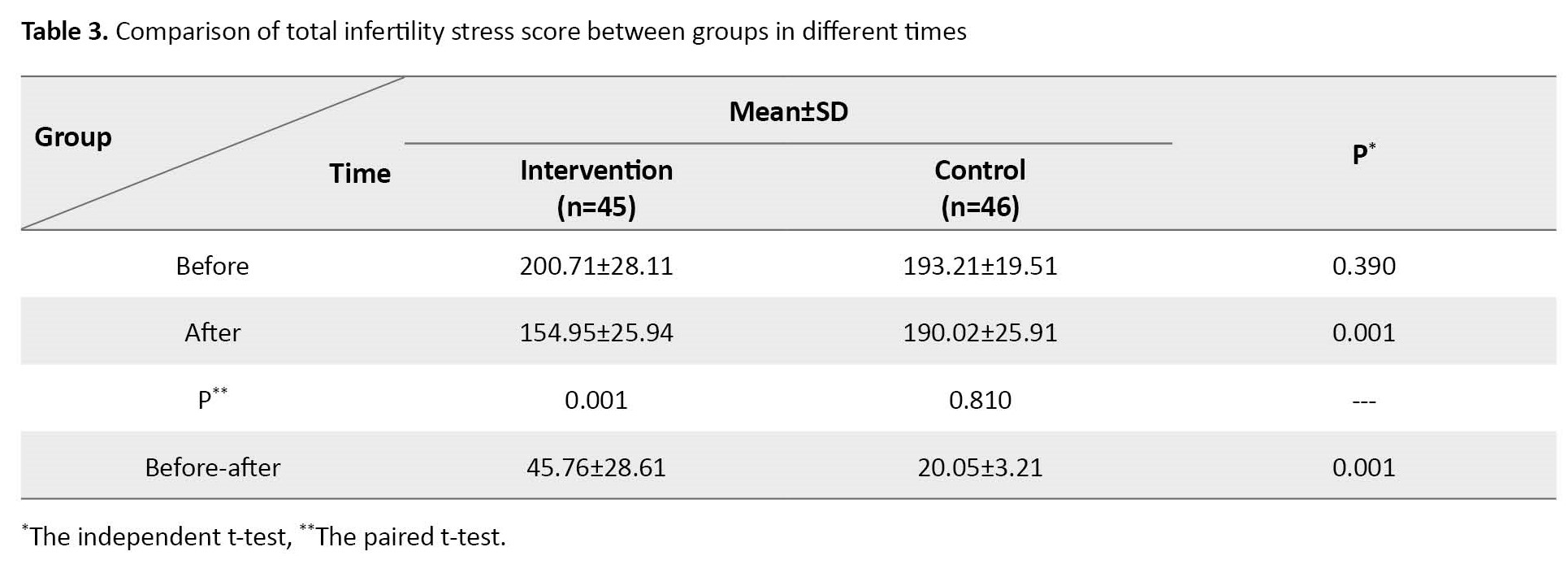
The independent t-test showed no significant difference in total infertility stress scores between the control group and intervention group before the intervention. However, total infertility stress scores significantly differed between the two groups after the intervention (P=0.001). Additionally, according to the paired t-test results, total infertility stress scores were significantly different before and after the intervention in the intervention group (P=0.001). However, the control group’s scores were not significantly different before and after the intervention (Table 3).
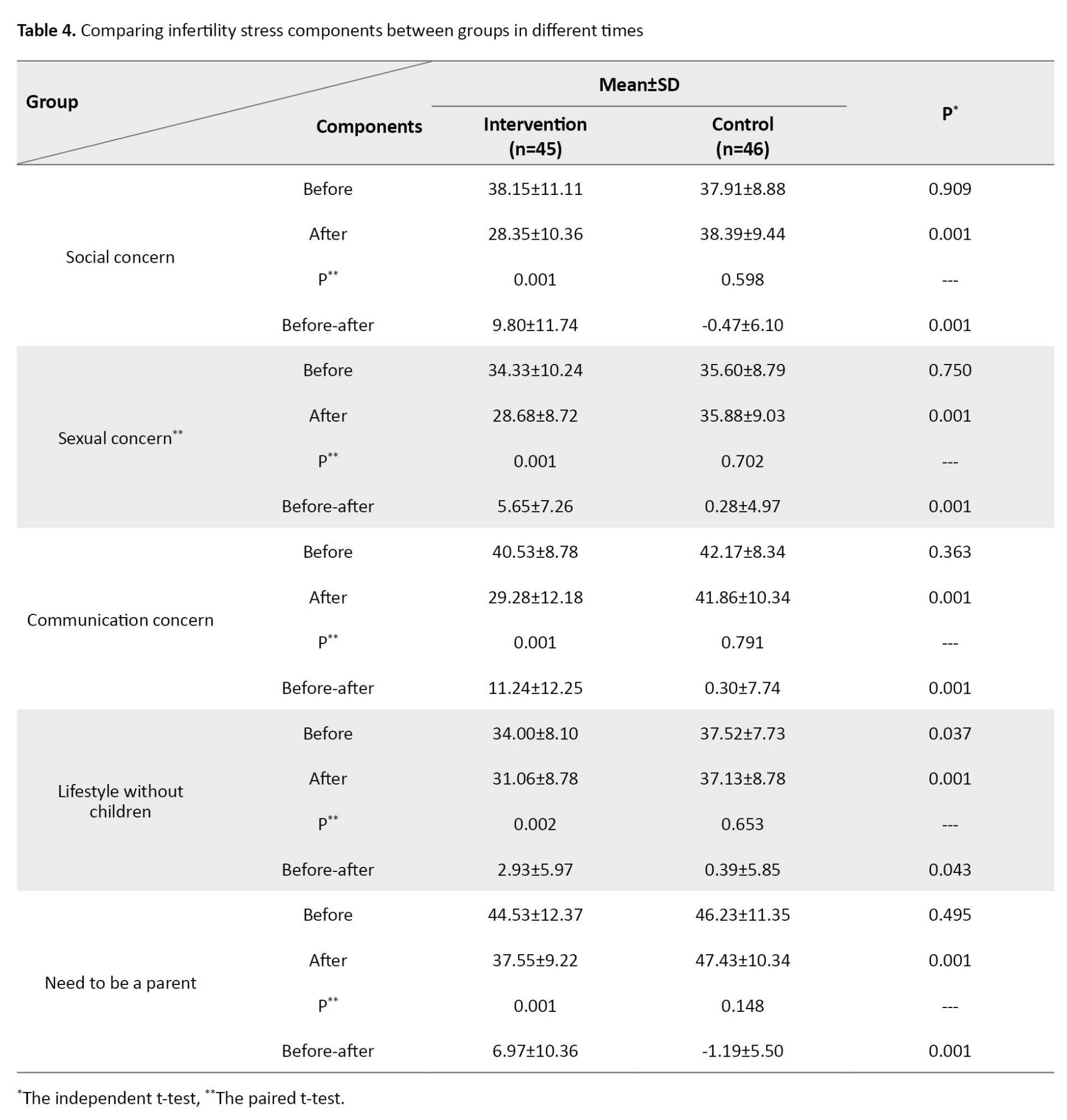
The results of the independent t-test showed no significant differences in any scales of the infertility stress questionnaire between the control group and intervention group before doing the intervention. However, all of the scales were significantly different between the two groups after doing the intervention, including social concern (P=0.001), sexual concern (P=0.001), communication concern (P=0.001), lifestyle without children (P=0.001), and need to be a parent (P=0.001).
Additionally, according to the results of the paired t-test, the scores of infertility stress in all its five components were significantly different before and after the intervention in the intervention group. However, the control group’s before and after scores were not significantly different (Table 4).
Discussion
The results showed that existential group therapy could reduce the infertility stress in infertile men’s spouses. At the same time, there were no significant differences in any subscales of the infertility stress questionnaire between the control group and intervention group before doing the intervention. The findings of the present study are in line with the results of previous research [22, 30].
Existential group therapy is a psychological intervention focusing on free will, autonomy, and the search for meaning. This treatment emphasizes the individual rather than the symptoms and people’s capacity to make rational choices and maximize their abilities [18]. Likewise, Amini et al. investigated the relationship between perceived social support and infertility stress in infertile men’s spouses. They concluded that stronger social support brings higher marital satisfaction in infertile men’s spouses [12]. As a result, existential group therapy can improve the marital status of infertile men’s wives by reducing social stress.
The difference between existential group therapy and other counseling methods is that different counseling styles try to control external events that determine a person’s behavior. In these styles, a person always needs a counselor to help him or her think. Still, in existential counseling, we intend to face people’s anxiety and ask them to examine themselves in different situations and think about the pros and cons of the situation. This method may cause stress, but we have already said that our goal is to deal with the problem and face it.
Mokhtari Sorkhani et al. conducted a study investigating the effectiveness of integrated psychological counseling with a couple therapy approach on the quality of life of infertile women. They concluded that integrated psychological counseling could improve the quality of life among infertile women [31]. Their study was consistent with the present study because they also could protect women in stressful events by using a form of group counseling.
Consistent with the present study, some other research results showed that existential psychotherapy is essential in promoting mental health and the quality of human life. In addition, studies have shown that existential psychotherapy increases people’s adaptation to stressful and intolerable situations and helps them cope with difficult and unfortunate situations by increasing resilience, which is consistent with the present study results [22, 30].
Kissane et al. studied the effect of cognitive-existential group therapy on the survival of people with breast cancer in the early stages. They concluded that cognitive group therapy could not improve survival in people with increased breast cancer, which was inconsistent with the present study’s effectiveness. The reason for the discrepancy could be that psychosocial interventions in cancer patients cannot guarantee survival. Still, they can increase the psychological well-being of people in stressful situations [32].
Indeed, the women in the intervention group did not try to deal with anxiety but wanted to accept it. In this case, it helped the wives of infertile men to realize that mourning for infertility confronts them with other possibilities, such as family breakdown, divorce, and loss of social and economic opportunities. Consequently, the wives of infertile men take responsibility for their lives. This condition gradually challenges them to realize the meaning of their lives. According to the principle of existential counseling, humans are free beings who must accept the responsibility that comes with freedom [11].
Infertility is an unintended event that an individual faces, but the individual has the ability and freedom to choose the response to that event.
Existential education and psychotherapy can help a person change his or her perspective on the situation and shape a bright future for himself or herself. The present study showed that several infertile men’s spouses are stressed in all areas, including social concerns, sexual concerns, communication concerns, worrying about a child free lifestyle, and the need to be parenthood. However, existential group therapy counseling has reduced this stress in these areas. Existential group therapy counseling can effectively reduce infertility stress in infertility treatment centers and family courts where couples intend to divorce due to infertility.
Finally, it should be noted that this study included only women whose infertility was caused by their spouses. Therefore, the results cannot be generalized to all infertile couples.
In the current study, the researcher aimed to investigate the effect of the existential group therapy approach on reducing the infertility stress of infertile men’s wives. Still, since men also experience this infertility stress, although less than women, it is suggested to investigate the effect of this.
Ethical Considerations
Compliance with ethical guidelines
This study respected all the international and national criteria for a clinical trial. Before the initiation of this study, all required official permissions were taken, including the institutional ethical code from Shahroud University of Medical Sciences (Code: IR.SHMU.REC.1399.134) and the national registration code from the Iranian Registry of Clinical Trials (Code: IRCT20210117050060N1). Informed consent was taken from the participants after detailed explanations about the study and before starting the study. They were assured of being completely free to quit the study at any point they felt uncomfortable. They were also assured about the confidentiality of their names and personal information. After completing the post-test questionnaires, an existential group therapy counseling session, which included 8 sessions, was held for the control group to maintain ethical conditions and not deprive the control group.
Funding
This article is taken from the master's thesis of Samira Ghorbani from Shahrood University, approved by the Vice-Chancellor of Graduate Education and Research, Shahrood University of Medical Sciences, Faculty of Nursing and Midwifery (code: 872).
Authors' contributions
Conceptualization, methodology investigation, project management, , data analysis, and writing the original draft: Samira Ghorbani; Conceived the study, investigated, managed the project, provided methodology, supervised, reviewed, and edited the manuscript: Shahrbanoo Salehin; Helped investigate, supervised, reviewed, and edited the manuscript: Ali Mohammad Nazari, Seyedeh Solmaz Talebi, and Afsaneh Keramat; Approve the final version of manuscript: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors thank and appreciate the support of the Department of Midwifery and the Vice Chancellor for Graduate Studies and Research of Shahroud University of Medical Sciences. The authors also thank and appreciate all the participants in this research.
References
Infertility is a pregnancy failure after one year of regular unprotected intercourse [1]. Infertility is a common disorder all around the world, and the disorder has been even increasing in most parts of the world in recent years [2]. Studies show that about 50 to 80 million people worldwide experience some form of infertility [3]. A recent study estimated that the overall prevalence of infertility in Iran is 7.88% [4].
Infertility can be the worst experience in a couple’s life, so infertile women often consider infertility the most stressful event in their lives and describe frequent and successive courses of treatment as repeated periods of crisis [5]. Infertility is regarded as a crisis in a couple’s life with many psychological consequences [6]. In all cultures worldwide, infertility has been known as a stressful individual, marital, family, and social experience, threatening marriage stability [7].
Infertility stress comprises a set of symptoms revealed in individuals when diagnosed with infertility [8]. Infertility stress appears as a combination of five components: Social concerns, sexual concerns, communication concerns, the need to be a parent, and not accepting a child-free lifestyle [9, 10]. After the death of first-degree family members and the stress of divorce, infertility and its treatment have the most stress level for individuals [11].
A study showed that infertile men’s spouses are as stressed as infertile women in many areas because women are more engaged with diagnostic and therapeutic procedures, even in male-induced infertility [12]. Women experience more concerns than their husbands. When women’s husbands are infertile, they experience reactions such as anxiety, stress, depression, and sadness. These women are stressed due to losing the ability to become mothers [13, 14].
In most cultures, women are considered to be responsible for not having children. Men evade their responsibilities, which worsens marital problems. According to previous studies, the stressful experience of infertility can be associated with a wide range of psychological disorders, such as decreased self-esteem; increased stress, anxiety, depression, and anger; inefficiency feelings; marital problems; and cognitive and emotional problems [15, 16]. It is also noteworthy that lower stress levels are associated with higher marital quality [17].
Existential group therapy is a psychological intervention focusing on free will, autonomy, and the search for meaning. This treatment concentrates on the individual rather than the symptoms and emphasizes the capacity to make rational choices and maximize this ability [18]. Instead of depriving an individual of authority, existential group therapy emphasizes the patient-therapist relationship, honest confrontation, and change as a courageous action. Although patients cannot change the bitter events of life, this group helps them change their analysis, thinking, and perception [19]. This therapeutic approach allows individuals to search for meaning, have a purpose, and create a positive relationship with psychological factors. It gives them more adaptation ability, life satisfaction, and psychological well-being [20]. The effectiveness of this method has been confirmed in various cases [21]. In a study, existential psychotherapy increased resilience in women with infertility [22]. Group therapy helps people recognize their strengths and weaknesses, identify their values and beliefs, compare them with others, improve them, and focus on current relationships instead of external problems [23, 24]. As a dynamic method, existential group therapy emphasizes understanding four basic issues: Death, freedom, loneliness, and meaninglessness [25]. This therapy helps people realize the meaning of their lives, be responsible, and profit from opportunities [26].
Considering the importance of infertility stress in the lives of infertile men’s wives, this study was conducted to investigate the effect of existential group therapy on infertility stress in the wives of infertile men.
Materials and Methods
The present study is a randomized clinical trial with two study groups: A counseling existential therapy group and a control group. It was conducted from August 2021 to March 2022. The research population of the study included women aged 20 to 45 who were accompanying their infertile husbands. They had moderate and high infertility stress and were referred to infertility clinics in Shahrood City, Iran.
To estimate the sample size, we used the following parameters in a similar study [27] as follows: The standard deviation of the first community was 13.2, the Standard deviation of the second community was 8, the mean difference between the two communities is 11.4 at a 95% confidence interval, and considering a test power of 80%. The sample size was then estimated at 43 participants, and 10% was added for dropout. Finally, 48 women participated in the intervention and 48 women in the control group (96 participants in total).
Ninety-six women who met all the inclusion criteria participated in the study after taking informed consent. The inclusion criteria were as follows: Willing to participate in research, being 20 to 45 years old, having infertility with male factor only, lacking children from a previous marriage, having at least primary education, lacking psychiatric disorders, not being a divorced applicant, and lacking sexual dysfunction in the wife of the husband. The exclusion criteria were as follows: Getting pregnant during the study, reluctance to attend the meetings for any reason, failure to complete the questionnaires, and more than two absences from the counseling sessions.
The study subjects were selected from women with a history of primary infertility and male infertility referred to the infertility center. We used a random sampling method for selecting cases and a random block in size 4 for allocation. The women of the intervention group were divided by chance into six sub-groups of 6 women each, receiving the same existential group therapy separately (eight sessions for each sub-group). The sessions were held virtually (due to the conditions of the COVID-19 pandemic). The control group did not receive any intervention other than routine follow-up of the infertility center. Figure 1 shows the process of conducting the study in summary.
The data collection tools for conducting this study were a demographic information questionnaire and an infertility stress questionnaire, previously designed by Newton et al. [28]. This questionnaire has 46 questions with 5 subscales: Social concerns, sexual concerns, communication concerns, childless lifestyle, and the need to be a parent. It measures the stress of infertility based on a 6-point rating scale ranging from “1” (strongly disagree) to “6” (strongly agree) with questions such as (when I’m asked about children, I don’t get upset). Considering that a high score in general stress indicates high stress in infertility, some questions are scored in reverse. The total stress level is calculated by adding all the raw scores in all five scales. The maximum score for the 10-question scale is 60, the minimum is 10, the 8-question scale is 48, and the minimum is 8. The maximum total score is 276, and the minimum is 46. Generally, a high score indicates high infertility stress.
Samani’s research confirmed the reliability of Newton’s infertility stress questionnaire in Iran [29].
The purpose of the study was explained to participants, who were included in the study after providing written informed consent. The electronically designed questionnaires were completed before the intervention and a week after the counseling sessions’ end by the intervention and control groups. The control group received routine treatment during existential group therapy for participants in the intervention group. A summary of the consultation sessions was given to the control group to observe the ethical aspects after the post-test. After completing the questionnaires, the collected information was entered into SPSS software, version 25 and subjected to statistical analysis. The normality of data was assessed using the Kolmogorov-Smirnov test. The data were analyzed by the chi-square test, Fisher exact test, and compare means t-test. A comparison of the groups was performed using the independent t-test. A comparison of stress scores before and after the intervention within each group was performed using the paired t-test.
Results
The Mean±SD of the age of the participants in the whole population is 31.68±5.17 years. In comparing the two study groups, their mean age was comparable. Of the total participants, 73 female participants (80.2%) were housewives. The participants’ percentages of employee, laborer, self-employed, and unemployed jobs were 34.1%, 20.9%, 41.8%, and 3.3%, respectively. The women’s education percentages of middle school education, diploma and post-diploma, bachelor’s and master’s degrees, and above were 14.28%, 36.28%, 40.65%, and 8.79%, respectively. The spouse's percentages of education, diploma and post-diploma, bachelor’s and master’s degree and above are 18.68%, 45.05%, 27.47%, and 8.79%, respectively. The spouse’s percentages of good, bad, and average economic status were 14.3%, 12.1%, and 73.6%, respectively. The chi-square test, Fisher exact test, and compare means t-test showed that the age, job, education, economic status, time of marriage, and duration of infertility were homogenous between the two groups. The median and interquartile range of the participants’ marriage duration in the entire population was 5. Based on the comparison test of the median of two independent societies, the duration of marriage is homogeneous in the two groups.
The median (interquartile range) of the participants’ infertility duration in the entire population is 4. Based on the comparison test of the median of two independent societies, the duration of marriage is homogeneous in two groups (Table 2).
The independent t-test showed no significant difference in total infertility stress scores between the control group and intervention group before the intervention. However, total infertility stress scores significantly differed between the two groups after the intervention (P=0.001). Additionally, according to the paired t-test results, total infertility stress scores were significantly different before and after the intervention in the intervention group (P=0.001). However, the control group’s scores were not significantly different before and after the intervention (Table 3).
The results of the independent t-test showed no significant differences in any scales of the infertility stress questionnaire between the control group and intervention group before doing the intervention. However, all of the scales were significantly different between the two groups after doing the intervention, including social concern (P=0.001), sexual concern (P=0.001), communication concern (P=0.001), lifestyle without children (P=0.001), and need to be a parent (P=0.001).
Additionally, according to the results of the paired t-test, the scores of infertility stress in all its five components were significantly different before and after the intervention in the intervention group. However, the control group’s before and after scores were not significantly different (Table 4).
Discussion
The results showed that existential group therapy could reduce the infertility stress in infertile men’s spouses. At the same time, there were no significant differences in any subscales of the infertility stress questionnaire between the control group and intervention group before doing the intervention. The findings of the present study are in line with the results of previous research [22, 30].
Existential group therapy is a psychological intervention focusing on free will, autonomy, and the search for meaning. This treatment emphasizes the individual rather than the symptoms and people’s capacity to make rational choices and maximize their abilities [18]. Likewise, Amini et al. investigated the relationship between perceived social support and infertility stress in infertile men’s spouses. They concluded that stronger social support brings higher marital satisfaction in infertile men’s spouses [12]. As a result, existential group therapy can improve the marital status of infertile men’s wives by reducing social stress.
The difference between existential group therapy and other counseling methods is that different counseling styles try to control external events that determine a person’s behavior. In these styles, a person always needs a counselor to help him or her think. Still, in existential counseling, we intend to face people’s anxiety and ask them to examine themselves in different situations and think about the pros and cons of the situation. This method may cause stress, but we have already said that our goal is to deal with the problem and face it.
Mokhtari Sorkhani et al. conducted a study investigating the effectiveness of integrated psychological counseling with a couple therapy approach on the quality of life of infertile women. They concluded that integrated psychological counseling could improve the quality of life among infertile women [31]. Their study was consistent with the present study because they also could protect women in stressful events by using a form of group counseling.
Consistent with the present study, some other research results showed that existential psychotherapy is essential in promoting mental health and the quality of human life. In addition, studies have shown that existential psychotherapy increases people’s adaptation to stressful and intolerable situations and helps them cope with difficult and unfortunate situations by increasing resilience, which is consistent with the present study results [22, 30].
Kissane et al. studied the effect of cognitive-existential group therapy on the survival of people with breast cancer in the early stages. They concluded that cognitive group therapy could not improve survival in people with increased breast cancer, which was inconsistent with the present study’s effectiveness. The reason for the discrepancy could be that psychosocial interventions in cancer patients cannot guarantee survival. Still, they can increase the psychological well-being of people in stressful situations [32].
Indeed, the women in the intervention group did not try to deal with anxiety but wanted to accept it. In this case, it helped the wives of infertile men to realize that mourning for infertility confronts them with other possibilities, such as family breakdown, divorce, and loss of social and economic opportunities. Consequently, the wives of infertile men take responsibility for their lives. This condition gradually challenges them to realize the meaning of their lives. According to the principle of existential counseling, humans are free beings who must accept the responsibility that comes with freedom [11].
Infertility is an unintended event that an individual faces, but the individual has the ability and freedom to choose the response to that event.
Existential education and psychotherapy can help a person change his or her perspective on the situation and shape a bright future for himself or herself. The present study showed that several infertile men’s spouses are stressed in all areas, including social concerns, sexual concerns, communication concerns, worrying about a child free lifestyle, and the need to be parenthood. However, existential group therapy counseling has reduced this stress in these areas. Existential group therapy counseling can effectively reduce infertility stress in infertility treatment centers and family courts where couples intend to divorce due to infertility.
Finally, it should be noted that this study included only women whose infertility was caused by their spouses. Therefore, the results cannot be generalized to all infertile couples.
In the current study, the researcher aimed to investigate the effect of the existential group therapy approach on reducing the infertility stress of infertile men’s wives. Still, since men also experience this infertility stress, although less than women, it is suggested to investigate the effect of this.
Ethical Considerations
Compliance with ethical guidelines
This study respected all the international and national criteria for a clinical trial. Before the initiation of this study, all required official permissions were taken, including the institutional ethical code from Shahroud University of Medical Sciences (Code: IR.SHMU.REC.1399.134) and the national registration code from the Iranian Registry of Clinical Trials (Code: IRCT20210117050060N1). Informed consent was taken from the participants after detailed explanations about the study and before starting the study. They were assured of being completely free to quit the study at any point they felt uncomfortable. They were also assured about the confidentiality of their names and personal information. After completing the post-test questionnaires, an existential group therapy counseling session, which included 8 sessions, was held for the control group to maintain ethical conditions and not deprive the control group.
Funding
This article is taken from the master's thesis of Samira Ghorbani from Shahrood University, approved by the Vice-Chancellor of Graduate Education and Research, Shahrood University of Medical Sciences, Faculty of Nursing and Midwifery (code: 872).
Authors' contributions
Conceptualization, methodology investigation, project management, , data analysis, and writing the original draft: Samira Ghorbani; Conceived the study, investigated, managed the project, provided methodology, supervised, reviewed, and edited the manuscript: Shahrbanoo Salehin; Helped investigate, supervised, reviewed, and edited the manuscript: Ali Mohammad Nazari, Seyedeh Solmaz Talebi, and Afsaneh Keramat; Approve the final version of manuscript: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors thank and appreciate the support of the Department of Midwifery and the Vice Chancellor for Graduate Studies and Research of Shahroud University of Medical Sciences. The authors also thank and appreciate all the participants in this research.
References
- RA R, Prameela J, Omkar B, Emmanuel G, Akhila S. A review on risk factors, staging and survival rates of endometrial cancer in both black and white women in infertility patients in USA. World J Curr Med Pharm Res. 2020; 2(2):152. [DOI:10.37022/WJCMPR.2020.2212]
- Abdullah A, Ahmed M, Oladokun A. Prevalence of infertility in Sudan: A systematic review and meta-analysis. Qatar Med J. 2021; 2021(3):47. [DOI:10.5339/qmj.2021.47] [PMID]
- Linconstant L. Infertility as a gendered social experience in Italy (Lombardy): Sense of self and modality of action. Reproductive governance and bodily materiality: Flesh, technologies, and knowledge. In: Guerzoni CS, Mattalucci C, editors. Bingley: Emerald; 2022. [DOI:10.1108/978-1-80071-438-020221014]
- Naz MS, Ozgoli G, Sayehmiri K. Prevalence of infertility In Iran: A systematic review and meta-analysis. Urol J. 2020; 17(4):338-45. [Link]
- Woods BM, Patrician PA, Fazeli PL, Ladores S. Infertility-related stress: A concept analysis. Nurs Forum. 2022; 57(3):437-45. [DOI:10.1111/nuf.12683] [PMID]
- Ara I, Maqbool M, Zehravi M. Psychic consequences of infertility on couples: A short commentary. Open Health. 2022; 3(1):114-9. [DOI:10.1515/openhe-2022-0022]
- Szkodziak F, Krzyżanowski J, Szkodziak P. Psychological aspects of infertility. A systematic review. J Int Med Res. 2020; 48(6):0300060520932403. [DOI:10.1177/0300060520932403] [PMID]
- Ying L, Wu LH, Wu X, Shu J, Loke AY. Endurance with partnership: A preliminary conceptual framework for couples undergoing in vitro fertilisation treatment. J Reprod Infant Psychol. 2018; 36(2):144-57. [DOI:10.1080/02646838.2017.1416335] [PMID]
- Patel A, Sharma PS, Narayan P, Binu VS, Dinesh N, Pai PJ. Prevalence and predictors of infertility-specific stress in women diagnosed with primary infertility: A clinic-based study. J Hum Reprod Sci. 2016; 9(1):28-34. [DOI:10.4103/0974-1208.178630] [PMID]
- Chaves C, Canavarro MC, Moura-Ramos M. The role of dyadic coping on the marital and emotional adjustment of couples with infertility. Fam Process. 2019; 58(2):509-23. [DOI:10.1111/famp.12364] [PMID]
- Hsu YL, Kuo BJ. Evaluations of emotional reactions and coping behaviors as well as correlated factors for infertile couples receiving assisted reproductive technologies. J Nurs Res. 2002; 10(4):291-302. [DOI:10.1097/01.JNR.0000347610.14166.52] [PMID]
- Amini L, Ghorbani B, Afshar B. [The comparison of infertility stress and perceived social support in infertile women and spouses of infertile men (Persian)]. Iran J Nurs. 2020; 32 (122):80-90. [DOI:10.29252/ijn.32.122.80]
- Moutzouri M, Sarantaki A, Gourounti K. The association of cognitive representations with psychological adjustment in experience of infertility and fertility treatment: A systematic review. Eur J Midwifery. 2021; 5:33. [DOI:10.18332/ejm/138598] [PMID]
- Kim M, Yi SJ, Hong JE. Experiences of women with male factor infertility under in vitro fertilization. Int J Environ Res Public Health. 2020; 17(21):7809. [DOI:10.3390/ijerph17217809] [PMID]
- Taghipour A, Karimi FZ, Latifnejad Roudsari R, Mazlom SR. Coping strategies of women following the diagnosis of infertility in their spouses: A qualitative study. Evid Based. 2020; 10(1):15-24. [DOI:10.22038/EBCJ.2020.42136.2120]
- Turner KA, Rambhatla A, Schon S, Agarwal A, Krawetz SA, Dupree JM, et al. Male infertility is a women’s health issue-research and clinical evaluation of male infertility is needed. Cells. 2020; 9(4):990. [DOI:10.3390/cells9040990] [PMID]
- Ebrahimi M, Mohsenzade F, Zahrakar K. [Marital challenges of infertile couples: A phenomenological study (Persian)]. Appl Fam Ther J. 2022; 3(2):67-84. [DOI:10.61838/kman.aftj.3.2.4]
- Nazari A, Zarghami S [Existential psychotherapy (Persian)]. Tehran: Pazineh; 2009.
- Tantam D, van Deurzen E. Existential group therapy: Method and practice. In: van Deurzen E, Craig E, Längle A, Schneider KJ, Tantam D, Plock S, editors. The Wiley world handbook of existential therapy. New Jersey: John Wiley & Sons Ltd; 2019. [DOI:10.1002/9781119167198.ch27]
- Du Plessis G. An existential perspective on addiction treatment: A logic-based therapy case study. Int J Philos Pract. 2019; 5(1):1-32. [DOI:10.5840/ijpp2019511]
- Taghipor B, Barzegan R. [The effectiveness of group therapy on self-development and resilience of mothers of children with intellectual disability (Persian)]. Knowl Res in Appl Psychol. 2019; 20(2):100-9. [Link]
- Rezaei Z, Jalili Nikoo S, Nejati Nezhad N, Ghasemi Jobaneh R, Nooryan K. [The effectiveness of existing psychotherapy on increasing resilience in infertile women (Persian)]. Armaghan Danesh. 2015; 20 (5):453-9. [Link]
- Friedman R. Individual or group therapy? Indications for optimal therapy. Group Anal 2013; 46(2):164-70. [DOI:10.1177/0533316413483691]
- Vanhooren S. Existential empathy: The challenge of ‘being’in therapy and counseling. Religions. 2022; 13(8):752. [DOI:10.3390/rel13080752]
- Zadafshar B, Sharifi T, Ahmadi R, Chorami M. Effectiveness of emotion-focused and existential group therapy on depression, anxiety, and stress in victims of child sexual harassment. J Client Cent Nurs Care. 2021; 7(3):227-36. [DOI:10.32598/JCCNC.7.3.379.1]
- Lybbert R, Ryland S, Bean R. Existential interventions for adolescent suicidality: Practical interventions to target the root causes of adolescent distress. Children Youth Serv Rev. 2019; 100:98-104. [DOI:10.1016/j.childyouth.2019.02.028]
- Faghani S, Ghaffari F. Effects of sexual rehabilitation using the plissit model on quality of sexual life and sexual functioning in post-mastectomy breast cancer survivors. Asian Pac J Cancer Prev. 2016; 17(11):4845-51. [PMID]
- Newton CR, Sherrard W, Glavac I. The fertility problem inventory: Measuring perceived infertility-related stress. Fertil Steril. 1999; 72(1):54-62. [DOI:10.1016/S0015-0282(99)00164-8] [PMID]
- Samani RO, Almasi-Hashiani A, Shokri F, Maroufizadeh S, Vesali S, Sepidarkish M. Validation study of the fertility problem inventory in iranian infertile patients. Middle East Fertil Soc J. 2017; 22(1):48-53. [DOI:10.1016/j.mefs.2016.07.002]
- Khodadadi Sangdeh J, Ghomi M. [The effectiveness of existential group psychotherapy on increasing psychological well-being mothers of children with cancer (Persian)]. Psychol stud. 2018; 13(4):125-40. [Link]
- Mokhtari Sorkhani T, Ahmadi A, Mirzaee M, Habibzadeh V, Alidousti Shahraki K. Effectiveness of integrated psychological counseling with couple therapy approach on quality of life of infertile women. J Holistic Nurs Midwifery. 2022; 32(2).144-51. [DOI:10.32598/jhnm.32.2.2191]
- Kissane DW, Love A, Hatton A, Bloch S, Smith G, Clarke DM, et al. Effect of cognitive-existential group therapy on survival in early-stage breast cancer. J Clin Oncol. 2004; 22(21):4255-60. [DOI:10.1200/JCO.2004.12.129] [PMID]
Article Type : Research |
Subject:
General
Received: 2024/02/24 | Accepted: 2024/02/21 | Published: 2024/02/21
Received: 2024/02/24 | Accepted: 2024/02/21 | Published: 2024/02/21
Send email to the article author
| Rights and permissions | |
 | This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Articles Copyright © The Author(s).
Owned by Guilan University of Medical Sciences.
Co-published by Negah Institute for Scientific Communication.
Contact Information
JHNM Office, Guilan University of Medical Sciences P.O.Box 41635-1873, Rasht, Iran
Journal Tel: +9813 33553202
Publisher Tel: +9821 453 55 555; +9821 453 55 000
Email: holisticnmj@gmail.com, nursjournal@gums.ac.ir
