Thu, Jan 29, 2026
Volume 34, Issue 4 (9-2024)
JHNM 2024, 34(4): 335-344 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Alizadeh Taghiabad B, Rassouli M, Jafaraghaee F, Abbasi Ranjbar Z, Maroufizadeh S, Doaee S et al . Assessing the Psychometric Properties of the Persian Version of the Integrative Health and Wellness Assessment Scale in Patients With Type 2 Diabetes. JHNM 2024; 34 (4) :335-344
URL: http://hnmj.gums.ac.ir/article-1-2236-en.html
URL: http://hnmj.gums.ac.ir/article-1-2236-en.html
Batoul Alizadeh Taghiabad1 

 , Maryam Rassouli2 , Fateme Jafaraghaee3 , Zahra Abbasi Ranjbar4 , Saman Maroufizadeh5 , Saeed Doaee6 , Zahra Taheri- Ezbarami *7
, Maryam Rassouli2 , Fateme Jafaraghaee3 , Zahra Abbasi Ranjbar4 , Saman Maroufizadeh5 , Saeed Doaee6 , Zahra Taheri- Ezbarami *7
, Maryam Rassouli2 , Fateme Jafaraghaee3 , Zahra Abbasi Ranjbar4 , Saman Maroufizadeh5 , Saeed Doaee6 , Zahra Taheri- Ezbarami *7
1- Assistant Professor of Nursing, Department of Nursing, Neyshabur University of Medical Sciences, Neyshabur, Iran.
2- Professor, Cancer Research Center, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
3- Associate Professor, Department of Medical Surgical Nursing, School of Nursing and Midwifery, Guilan University of Medical Sciences, Rasht, Iran.
4- Assistant Professor, Department of Internal Medicine, School of Medicine, RAZI Hospital, Guilan University of Medical Sciences, Rasht, Iran.
5- Assistant Professor, Department of Biostatistics, School of Health, Guilan University of Medical Sciences, Rasht, Iran.
6- Department of Community Nutrition, School of Nutrition and Food Sciences, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
7- Associate Professor, Department of Nursing, School of Nursing and Midwifery, Guilan University of Medical Sciences, Rasht, Iran. ,Zahra_ztt@yahoo.com
2- Professor, Cancer Research Center, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
3- Associate Professor, Department of Medical Surgical Nursing, School of Nursing and Midwifery, Guilan University of Medical Sciences, Rasht, Iran.
4- Assistant Professor, Department of Internal Medicine, School of Medicine, RAZI Hospital, Guilan University of Medical Sciences, Rasht, Iran.
5- Assistant Professor, Department of Biostatistics, School of Health, Guilan University of Medical Sciences, Rasht, Iran.
6- Department of Community Nutrition, School of Nutrition and Food Sciences, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
7- Associate Professor, Department of Nursing, School of Nursing and Midwifery, Guilan University of Medical Sciences, Rasht, Iran. ,
Full-Text [PDF 1136 kb]
(388 Downloads)
| Abstract (HTML) (936 Views)
Full-Text: (386 Views)
Introduction
Diabetes is a common chronic metabolic disorder and one of the most critical health, financial and social challenges in the world [1]. it is estimated that it will become the seventh leading cause of death in the world by 2030 [2]. About 50% of patients with diabetes have poor blood sugar control. Despite the high demand for patient-centered “self-care”, there are no care programs with serious follow-up [3]. The actions to prevent or control the major chronic diseases, including diabetes, should focus on lifestyle health and wellness interventions [4]. In the management of chronic diseases, one of the patient-centered approaches that has been used all over the world in recent decades, in which the patient makes decisions, is the new technique of health coaching [2]. Considering the important role of a healthy lifestyle in controlling diabetes [5, 6], American Nurses Association (ANA) and 19 other professional nursing organizations officially approved the role of nurse coach in 2013 [7]. One of the theories proposed to guide nurse coaching activities in the last decade is the theory of integrative nurse coaching (TINC) [8]. This theory is the basis for coaching interventions to support health promotion through healthy lifestyle changes [9]. Through the therapeutic relationships, the nurse helps the patient identify the first step on their path to wellness. As a coach, the nurse helps patients define their goals and determine where to begin in the change process by drawing on their strengths, inner wisdom, values, and past successes. The role of nurse coach encompasses nursing skills and coaching in all areas of nursing, including nursing care. In this role, integrated assessment is essential [10]. Nurse coaching is a unique role that aims to help patients establish health goals, modify lifestyle habits, manage health conditions, and incorporate integrative practices, when appropriate, to promote healthier lifestyles [11].
Considering that nurses can be effective in many health outcomes and their actions are aimed at improving the health and wellness of patients, and since nursing, especially holistic nursing, considers nurse coaching as a solution to the challenge of strengthening health and wellness, the tools derived from evidence-based holistic approaches such as the short form integrative health and wellness assessment (IHWA) are needed. With the IHWA scale, the basic scores before and after the lifestyle change can be compared and it can be used as a tool to measure the outcome [9]. This tool was developed based on the TINC [4, 9, 10] first by Keegan and Dossey in 2011 as a 132-item questionnaire according to the principles of holistic nursing for self-assessment and self-reflection on eight dimensions of TINC-based wellness. This version has never been published as an article [10]. With the development of TINC [8], the tool was developed in 2015 in a shorter form (36 items) to support the self-assessment and self-reflection needs of nurses, especially in the coaching activity with limited time. Although instruments such as HPLP II and 12-item short form survey (SF-12) are valid tools designed to measure health, they do not measure wellness as described by TINC. Instruments such as the IHWA short form provide data that support outcomes of nurse-patient engagement [9]. Also, as a self-assessment tool, it helps the nurse coach and patients to check their wellness status from eight different dimensions [10], including life balance and satisfaction, relationships, spiritual, mental, emotional, physical (nutrition, exercise, weight), environmental, and health responsibility [4, 9]. The IHWA short form is often used in initial coaching sessions to facilitate interaction and discussion between the patient and the nurse coach [11].
The assessment tools should be appropriate and in accordance with the culture and norms of the societies and countries where the tools are used. A tool designed for a particular society reflects the language and culture of that society and its use in other societies is associated with many challenges [12]. Considering that coaching interventions by nurses have led to blood sugar control and improved self-management of diabetes in patients, the use of TINC can be the best and most appropriate theoretical framework for research in this field [13]. Due to the lack of a valid and reliable questionnaire in Persian to evaluate the state of health and wellness and the effectiveness of nurse coaching interventions according to the TINC in Iranian patients with diabetes, the translation and validation of the Persian IHWA short form for the diabetic population of Iran can be helpful. Therefore, the purpose of the present study is to evaluate the psychometric properties of the Persian version of IHWA short form in patients with diabetes.
Materials and Methods
This is a quantitative methodological study, which was carried out in order to culturally adapt the IHWA short form, which was developed by Dossey et al. [8, 9] to Persian culture. Participants were patients with type 2 diabetes referred to the diabetes clinic of a teaching hospital in Rasht, Iran, in 2022-2023. After obtaining the necessary permits and obtaining informed consent from the patients, a demographic/clinical form, the Persian IHWA short form, and the Persian SF12 were completed by them. One of the authors was present in the clinic throughout the completion of the questionnaires and provided the necessary explanations to them in case of any difficulty.
The developers of the IHWA used PCA factor analysis with non-orthogonal rotation (Oblimin method) for the psychometrics of the tool. The factors found in this analysis accounted for 74.9% of the variance. Observing related items in each domain, factor loading, and item-total correlations, resulted in a revised 36-item short form of IHWA, which was confirmed in confirmatory factor analysis. The total score of the 36-question IHWA, using a 5-point Likert scale, ranges from 36 to 180. The internal consistency of the instrument using Cronbach’s α coefficient ranged from 0.45 for life balance/satisfaction to 0.88 for physical dimension, and the internal consistency of the overall scale was reported as 0.88 [9]. After correspondence with the developers of the IHWA and obtaining permission from them, the process of psychometric evaluation and cross-cultural adaptation was carried out based on the six-step model of Beaton et al [14].
First, using the forward-backward translation method, the original English version was translated into Persian by two people who are proficient in translating medical texts. The translated version was compared with the main version by two translators expert in English and the items were matched in terms of meaning and concept, and by choosing the best options, a Persian version of this tool was prepared. Then, to fully ensure the compatibility of the Persian version with the original version and the appropriateness of the sentences of the Persian version, it was translated back into English by another translator fluent in English who had not seen the original questionnaire before. Then, to get the final approval, the translated English draft was sent to the designer of the main version. In terms of compatibility, it was approved by the designer.
After the completion of the translation process, the validity (form, content, and construct) and reliability of the instrument were assessed. To determine the qualitative face validity, 16 patients with type 2 diabetes who were not the same in terms of gender, disease duration, education level and social status, were interviewed face to face. They were asked to comment on the appropriateness of the tool with the research objectives and the level of difficulty, clarity, simplicity and comprehensibility of the items. Modification of the items was done based on their comments. Both qualitative and quantitative approaches were used to determine content validity. In the qualitative approach, 14 experts (an expert in internal medicine, a diabetes clinic nurse, and nursing professors) were asked to give the necessary feedback after the quality review of the tool based on grammar, the use of appropriate words, the placement of phrases, and scoring. Modifications were done based on their comments. To determine content validity quantitatively, content validity ratio (CVR) and content validity index (CVI) were calculated, and the above-mentioned experts were asked to determine the necessity of each item of the tool. The numerical value of the CVR was calculated and interpreted using the Lawshe table. If the number is greater than the number in the Lawshe table, it means that the existence of that item in this tool is necessary and important [15]. In measuring the CVI, the relevance of each item (I-CVI) and all items (S-CVI) were examined using the opinions of experts. To obtain the S-CVI, the average of I-CVI for all items was calculated.
The construct validity of the instrument was determined by performing confirmatory factor analysis (CFA). Maximum likelihood algorithm was used to determine goodness-of-fit. Several fit indices are used in CFA, including χ2 (chi-square), df (degree of freedom), χ2/df, CFI (comparative fit index), SRMR (standardized root-mean square residual), and RMSEA (root mean square error of approximation). In general, at least 200 samples are recommended for performing CFA. This sample size is able to provide a high test power of 0.80 using RMSEM for a model with 100 degrees of freedom in a structural equation model [16]. In this study, the sample size was 202. Sampling was done by a convenience method. Inclusion criteria were a type 2 diabetes, age 18-65 years, not suffering from severe heart or kidney diseases and severe visual, hearing, cognitive, or mental disorders that cause disturbances in the measurement process, and willingness to participate in the study. The convergent validity of the tool was also determined. Considering that SF-12 is also a general measure of health status (physical and mental) [9], it was used for assessing convergent validity. Montazeri et al. investigated the validity and test re-test reliability of SF-12 in Iran. For the physical and mental domains, the reliability was reported as 0.73 and 0.72, respectively [17].
To determine the reliability of the questionnaire, the test re-test reliability and internal consistency were measured. For test re-test reliability, the questionnaire was presented to 15 patients in two stages with a 2-week interval, and then the Intra-class Correlation Coefficient (ICC) between the two rounds of assessments was calculated. The acceptable value for ICC is >0.6; the values closer to 1 indicate higher reliability [15]. Cronbach’s α coefficient was used to measure the internal consistency. The Mean±SD were used to describe the data, and Pearson’s correlation test was used to assess the relationship between the scores of IHWA and SF-12. Data analysis was done using AMOS software, version 26 and SPSS software, version 22.
Results
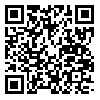
In this study, 202 patients with type 2 diabetes completed the Persian IHWA questionnaire. Their demographic and clinical information are reported in Table 1.
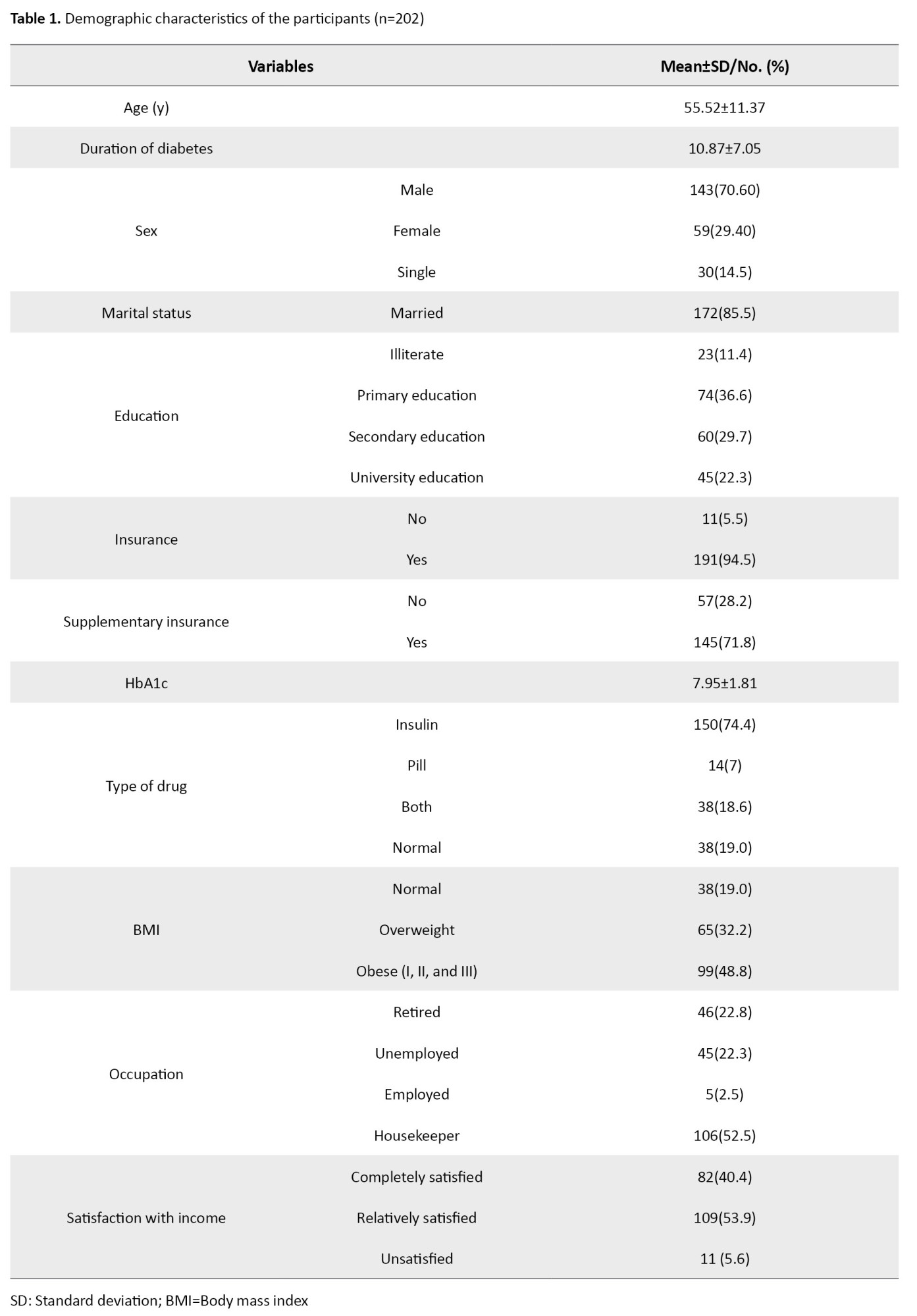
The descriptive scores of the IHWA domains are presented in Table 2.
The CVR was 0.96 for the whole scale. For the domains, the value was in the range of 0.57-1. The CVI of all items was higher than 0.83. For all subscales (S-CVI), this value was 0.97, which are acceptable.
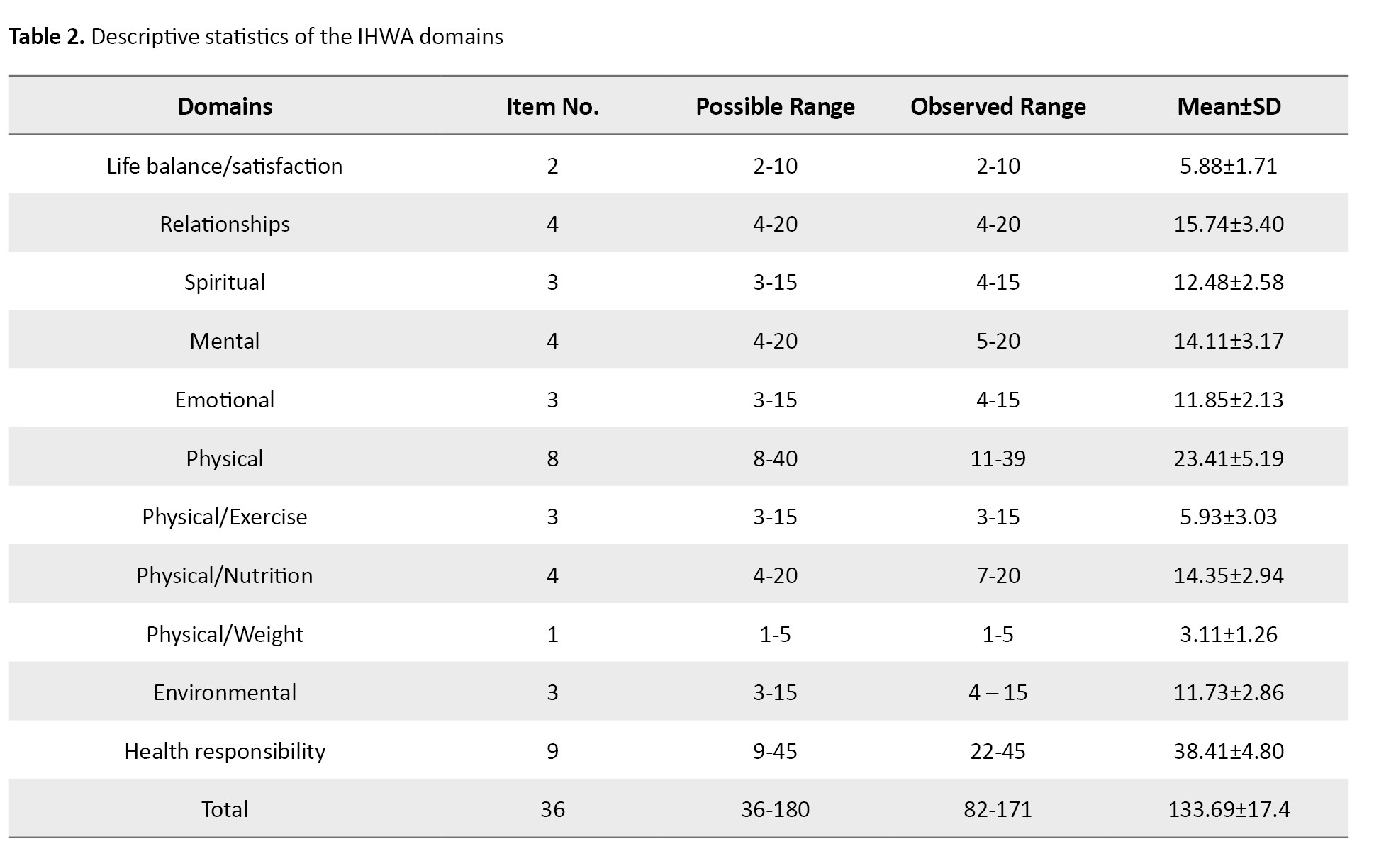
To examine the factor structure of the Persian IHWA, the CFA was performed (Figure 1).
 According to the goodness of fit indices, the eight-factor model of the second order of IHWA was not suitable (χ2/df=2.12; CFI=0.89; RMSEA=0.075, SRMR=0.100). The analysis of covariance was used to correct the indices between items 8 and 9, between items 17 and 18, and between items 25 and 26. After taking into account the covariance between the above items, a better fit was obtained (χ2/df=1.92, CFI=0.91; RMSEA=0.068, SRMR=0.081). In the CFA, all standardized factor loadings were significant and in the expected direction and ranged from 0.17 (item 28) to 0.83 (item 5). Therefore, the appropriateness of the Persian version to measure integrated health and wellness dimensions was confirmed.
According to the goodness of fit indices, the eight-factor model of the second order of IHWA was not suitable (χ2/df=2.12; CFI=0.89; RMSEA=0.075, SRMR=0.100). The analysis of covariance was used to correct the indices between items 8 and 9, between items 17 and 18, and between items 25 and 26. After taking into account the covariance between the above items, a better fit was obtained (χ2/df=1.92, CFI=0.91; RMSEA=0.068, SRMR=0.081). In the CFA, all standardized factor loadings were significant and in the expected direction and ranged from 0.17 (item 28) to 0.83 (item 5). Therefore, the appropriateness of the Persian version to measure integrated health and wellness dimensions was confirmed.
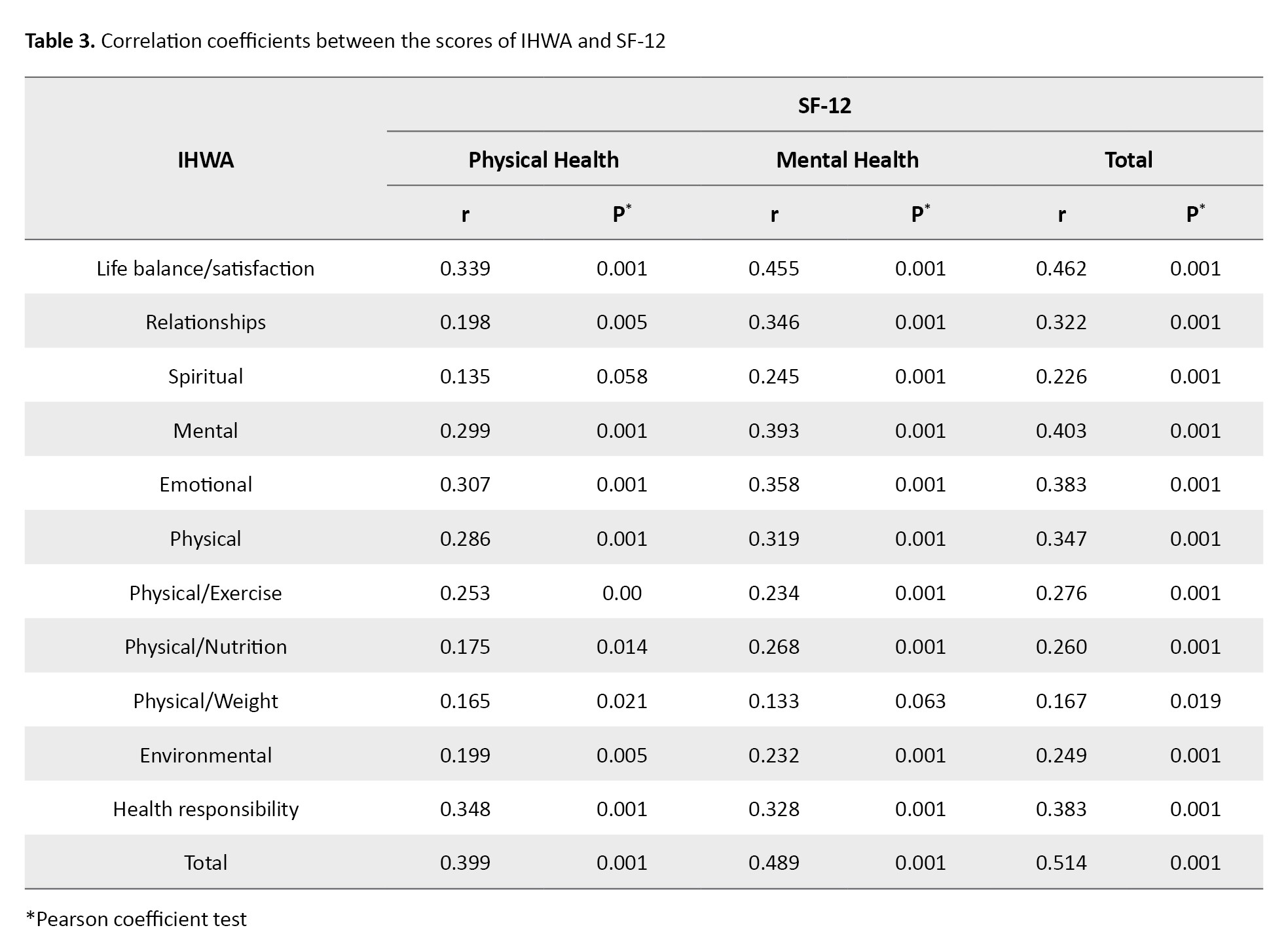
The results of the convergent validity test showed that the total score of the IHWA and each of its dimensions had a significant correlation with the total SF-12 score and its dimensions, with a small to large effect size and in the expected direction (Table 3).
These results confirm the convergent validity of the Persian version of the IHWA tool. Cronbach’s α value for the whole questionnaire was calculated as 0.889. Also, the test re-test reliability using the ICC was calculated as 0.833 (Table 4).
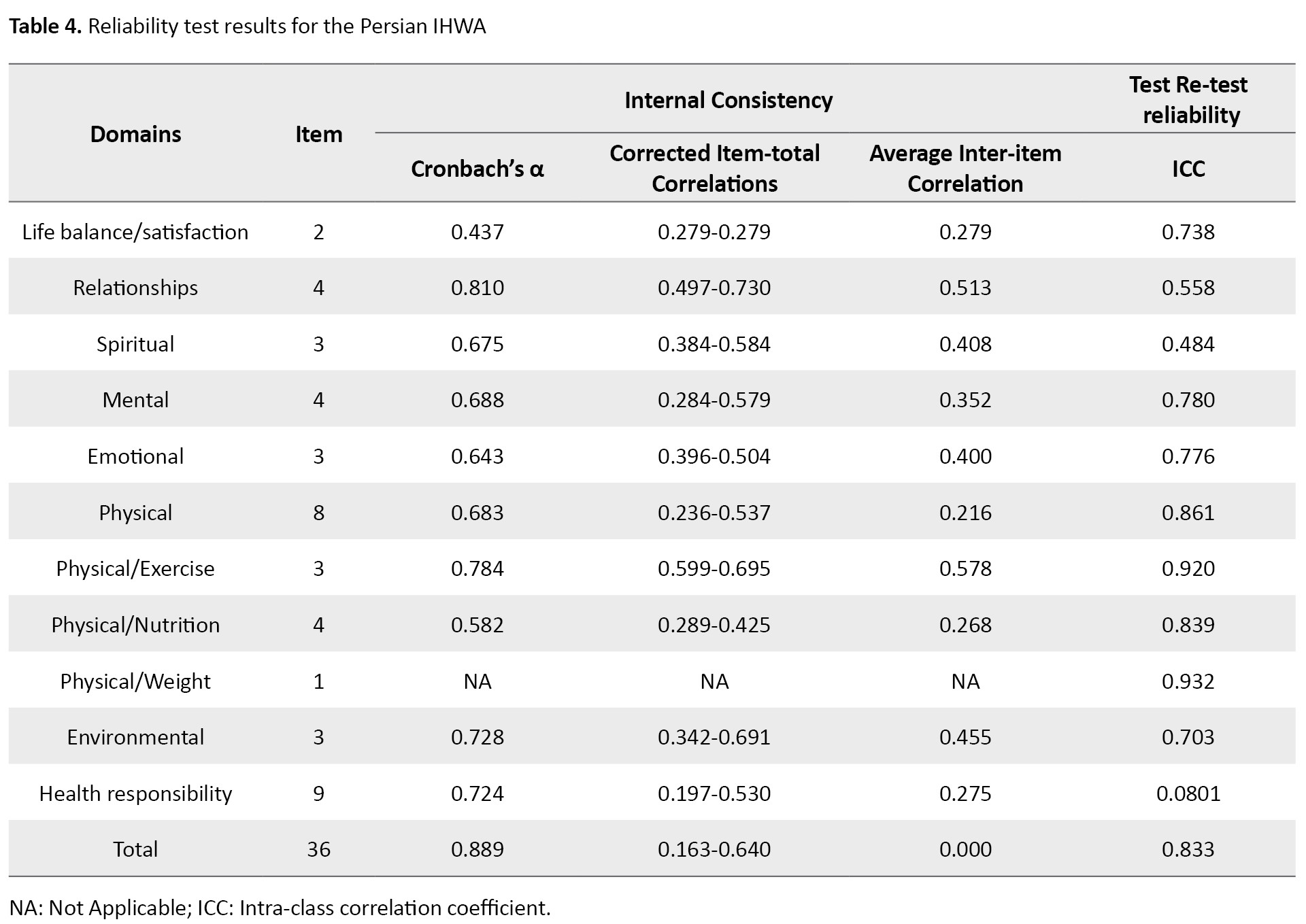
These results indicate the good reliability of the Persian IHWA.
Discussion
This study aimed to assess the psychometric properties of the Persian version of the IHWA questionnaire. In the present study, the face validity and content validity of the Persian instrument were confirmed. Similar to the present study, McElligott et al. also confirmed the content validity of the English IHWA tool, where they reported 100% inter-rater agreement [9]. In our study, the values of the fit indices in the CFA for construct validity were within the desired range, indicating that the model had a good fit to the data. The factor loadings in the relationship between domains and items and also the factor loadings between the total score and the domain scores were significant. This is consistent with McElligott et al.’s study for the original version. The Persian IHWA score had a significant positive relationship with the SF-12 score, confirming its convergent validity. The Cronbach’s α coefficients showed high internal consistency, similar to the original version. The appropriate Cronbach’s α in each domain indicates that the items constituting that domain are a suitable representation of the content of that domain [15, 18]. In McElligott et al.’s study, Cronbach’s α was 0.880 [10], which is close to our result. In the present study, the α value was lower in the dimension of life balance/satisfaction. Life satisfaction is a very important factor in the life of a patient with type 2 diabetes and leads to better treatment effects and improvement of the patient’s wellness. In these patients, low levels of life balance and satisfaction may negatively affect self-care behaviors and treatment outcomes. It seems that the reason for the low reliability of this dimension is due to the nature of satisfaction, which may vary from time to time depending on the physical, mental and psychological conditions of the person. It is also can be due to physical and mental conditions caused by the disease or mental and physical stress of nurses due to job conditions. In Iran, a study showed a positive and direct relationship between nutritional behaviors and life satisfaction in diabetic patients [19]. In a study conducted in two countries, Serbia and Poland, most nurses reported moderate life satisfaction. One of the factors predicting life satisfaction that are more prominent is job satisfaction and fatigue of nurses [20]. The highest reliability in the current study was observed in the dimension of relationships, while in McElligott et al.’s study, it was reported in the physical dimension [9]. The results for other dimensions were almost similar. Perhaps the reason for the discrepancy was the different culture, lifestyle, and the study population. In our study, participants were diabetic patients with high blood sugar and different physical conditions. In McElligott et al.’s study, nurses who had high knowledge about the side effects of inactivity, the importance of regular exercise and a healthy diet participated [9]. The increase in the prevalence of diabetes is related to lifestyle changes, including lack of a proper diet, physical activity, and obesity [19]. The IHWA short form has not been translated to other languages, so far, and the psychometric properties of other versions are not available to compare.
Considering the importance of patient- and community-centered evaluations in coaching sessions conducted by the nurse coach, the valid and reliable Persian version of IHWA can be used in all clinical settings in Iran to more accurately and reliably identify the lifestyle of people with type 2 diabetes. In addition, the Persian version of IHWA allows the Iranian nurse coach to conduct a more comprehensive assessment of these patients and evaluate the effects of coaching interventions on them. Since this tool was psychometrically evaluated for diabetic patients in this study and the TINC theory describes comprehensive nursing practice, it is suitable for use in many areas, such as lifestyle, chronic diseases, end-of-life care, etc. [4].
The present study, like other studies, had some disadvantages/limitations. The used instruments were self-report tools, and the study was conducted on diabetic patients in one of the hospitals in Rasht City. The results cannot be generalized to all people with type 2 diabetes in Iran. It is recommended that the validity and reliability of the Persian IHWA should be measured in other populations in Iran such as healthy people and or patients with other chronic patients who need to change their lifestyle for recovery. The Persian IHWA was validated in this study due to the lack of a specific tool to measure the effect of the nurse coach program in patients with type 2 diabetes in Iran. It is a valid and reliable tool that can be used in other studies to measure integrated health and wellness in these patients by nurses or other members of the treatment team. More studies are recommended in other countries to validate this tool for other cultures with different health systems
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of Guilan University of Medical Sciences (Code: IR.GUMS.REC.1399.617). All ethical principles, such as the informed consent from the participants, the confidentiality of their information, and their right to leave the study, were observed in this study.
Funding
This article was funded by the Deputy for Research and Technology of Guilan University of Medical Sciences.
Authors' contributions
Study design: Maryam Rassouli, Zahra Abbasi Ranjbar, Saman Maroufizadeh and Zahra Taheri-Ezbarami; Research: Zahra Taheri-Ezbarami; Data curation: Batoul Alizadeh Taghiabad, Fateme Jafaraghaee, Maryam Rassouli and Zahra Abbasi Ranjbar; Data collection: Batoul Alizadeh Taghiabad, and Fateme Jafaragha; Data analysis: Saman Maroufizadeh; Draft preparation: Batoul Alizadeh Taghiabad, Fateme Jafaraghaee, and Saman Maroufizadeh; Final approval: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors would like to thank the Deputy for Research and Technology of Guilan University of Medical Sciences for their financial support and to thank all patients participated in this study for their cooperation.
References
Diabetes is a common chronic metabolic disorder and one of the most critical health, financial and social challenges in the world [1]. it is estimated that it will become the seventh leading cause of death in the world by 2030 [2]. About 50% of patients with diabetes have poor blood sugar control. Despite the high demand for patient-centered “self-care”, there are no care programs with serious follow-up [3]. The actions to prevent or control the major chronic diseases, including diabetes, should focus on lifestyle health and wellness interventions [4]. In the management of chronic diseases, one of the patient-centered approaches that has been used all over the world in recent decades, in which the patient makes decisions, is the new technique of health coaching [2]. Considering the important role of a healthy lifestyle in controlling diabetes [5, 6], American Nurses Association (ANA) and 19 other professional nursing organizations officially approved the role of nurse coach in 2013 [7]. One of the theories proposed to guide nurse coaching activities in the last decade is the theory of integrative nurse coaching (TINC) [8]. This theory is the basis for coaching interventions to support health promotion through healthy lifestyle changes [9]. Through the therapeutic relationships, the nurse helps the patient identify the first step on their path to wellness. As a coach, the nurse helps patients define their goals and determine where to begin in the change process by drawing on their strengths, inner wisdom, values, and past successes. The role of nurse coach encompasses nursing skills and coaching in all areas of nursing, including nursing care. In this role, integrated assessment is essential [10]. Nurse coaching is a unique role that aims to help patients establish health goals, modify lifestyle habits, manage health conditions, and incorporate integrative practices, when appropriate, to promote healthier lifestyles [11].
Considering that nurses can be effective in many health outcomes and their actions are aimed at improving the health and wellness of patients, and since nursing, especially holistic nursing, considers nurse coaching as a solution to the challenge of strengthening health and wellness, the tools derived from evidence-based holistic approaches such as the short form integrative health and wellness assessment (IHWA) are needed. With the IHWA scale, the basic scores before and after the lifestyle change can be compared and it can be used as a tool to measure the outcome [9]. This tool was developed based on the TINC [4, 9, 10] first by Keegan and Dossey in 2011 as a 132-item questionnaire according to the principles of holistic nursing for self-assessment and self-reflection on eight dimensions of TINC-based wellness. This version has never been published as an article [10]. With the development of TINC [8], the tool was developed in 2015 in a shorter form (36 items) to support the self-assessment and self-reflection needs of nurses, especially in the coaching activity with limited time. Although instruments such as HPLP II and 12-item short form survey (SF-12) are valid tools designed to measure health, they do not measure wellness as described by TINC. Instruments such as the IHWA short form provide data that support outcomes of nurse-patient engagement [9]. Also, as a self-assessment tool, it helps the nurse coach and patients to check their wellness status from eight different dimensions [10], including life balance and satisfaction, relationships, spiritual, mental, emotional, physical (nutrition, exercise, weight), environmental, and health responsibility [4, 9]. The IHWA short form is often used in initial coaching sessions to facilitate interaction and discussion between the patient and the nurse coach [11].
The assessment tools should be appropriate and in accordance with the culture and norms of the societies and countries where the tools are used. A tool designed for a particular society reflects the language and culture of that society and its use in other societies is associated with many challenges [12]. Considering that coaching interventions by nurses have led to blood sugar control and improved self-management of diabetes in patients, the use of TINC can be the best and most appropriate theoretical framework for research in this field [13]. Due to the lack of a valid and reliable questionnaire in Persian to evaluate the state of health and wellness and the effectiveness of nurse coaching interventions according to the TINC in Iranian patients with diabetes, the translation and validation of the Persian IHWA short form for the diabetic population of Iran can be helpful. Therefore, the purpose of the present study is to evaluate the psychometric properties of the Persian version of IHWA short form in patients with diabetes.
Materials and Methods
This is a quantitative methodological study, which was carried out in order to culturally adapt the IHWA short form, which was developed by Dossey et al. [8, 9] to Persian culture. Participants were patients with type 2 diabetes referred to the diabetes clinic of a teaching hospital in Rasht, Iran, in 2022-2023. After obtaining the necessary permits and obtaining informed consent from the patients, a demographic/clinical form, the Persian IHWA short form, and the Persian SF12 were completed by them. One of the authors was present in the clinic throughout the completion of the questionnaires and provided the necessary explanations to them in case of any difficulty.
The developers of the IHWA used PCA factor analysis with non-orthogonal rotation (Oblimin method) for the psychometrics of the tool. The factors found in this analysis accounted for 74.9% of the variance. Observing related items in each domain, factor loading, and item-total correlations, resulted in a revised 36-item short form of IHWA, which was confirmed in confirmatory factor analysis. The total score of the 36-question IHWA, using a 5-point Likert scale, ranges from 36 to 180. The internal consistency of the instrument using Cronbach’s α coefficient ranged from 0.45 for life balance/satisfaction to 0.88 for physical dimension, and the internal consistency of the overall scale was reported as 0.88 [9]. After correspondence with the developers of the IHWA and obtaining permission from them, the process of psychometric evaluation and cross-cultural adaptation was carried out based on the six-step model of Beaton et al [14].
First, using the forward-backward translation method, the original English version was translated into Persian by two people who are proficient in translating medical texts. The translated version was compared with the main version by two translators expert in English and the items were matched in terms of meaning and concept, and by choosing the best options, a Persian version of this tool was prepared. Then, to fully ensure the compatibility of the Persian version with the original version and the appropriateness of the sentences of the Persian version, it was translated back into English by another translator fluent in English who had not seen the original questionnaire before. Then, to get the final approval, the translated English draft was sent to the designer of the main version. In terms of compatibility, it was approved by the designer.
After the completion of the translation process, the validity (form, content, and construct) and reliability of the instrument were assessed. To determine the qualitative face validity, 16 patients with type 2 diabetes who were not the same in terms of gender, disease duration, education level and social status, were interviewed face to face. They were asked to comment on the appropriateness of the tool with the research objectives and the level of difficulty, clarity, simplicity and comprehensibility of the items. Modification of the items was done based on their comments. Both qualitative and quantitative approaches were used to determine content validity. In the qualitative approach, 14 experts (an expert in internal medicine, a diabetes clinic nurse, and nursing professors) were asked to give the necessary feedback after the quality review of the tool based on grammar, the use of appropriate words, the placement of phrases, and scoring. Modifications were done based on their comments. To determine content validity quantitatively, content validity ratio (CVR) and content validity index (CVI) were calculated, and the above-mentioned experts were asked to determine the necessity of each item of the tool. The numerical value of the CVR was calculated and interpreted using the Lawshe table. If the number is greater than the number in the Lawshe table, it means that the existence of that item in this tool is necessary and important [15]. In measuring the CVI, the relevance of each item (I-CVI) and all items (S-CVI) were examined using the opinions of experts. To obtain the S-CVI, the average of I-CVI for all items was calculated.
The construct validity of the instrument was determined by performing confirmatory factor analysis (CFA). Maximum likelihood algorithm was used to determine goodness-of-fit. Several fit indices are used in CFA, including χ2 (chi-square), df (degree of freedom), χ2/df, CFI (comparative fit index), SRMR (standardized root-mean square residual), and RMSEA (root mean square error of approximation). In general, at least 200 samples are recommended for performing CFA. This sample size is able to provide a high test power of 0.80 using RMSEM for a model with 100 degrees of freedom in a structural equation model [16]. In this study, the sample size was 202. Sampling was done by a convenience method. Inclusion criteria were a type 2 diabetes, age 18-65 years, not suffering from severe heart or kidney diseases and severe visual, hearing, cognitive, or mental disorders that cause disturbances in the measurement process, and willingness to participate in the study. The convergent validity of the tool was also determined. Considering that SF-12 is also a general measure of health status (physical and mental) [9], it was used for assessing convergent validity. Montazeri et al. investigated the validity and test re-test reliability of SF-12 in Iran. For the physical and mental domains, the reliability was reported as 0.73 and 0.72, respectively [17].
To determine the reliability of the questionnaire, the test re-test reliability and internal consistency were measured. For test re-test reliability, the questionnaire was presented to 15 patients in two stages with a 2-week interval, and then the Intra-class Correlation Coefficient (ICC) between the two rounds of assessments was calculated. The acceptable value for ICC is >0.6; the values closer to 1 indicate higher reliability [15]. Cronbach’s α coefficient was used to measure the internal consistency. The Mean±SD were used to describe the data, and Pearson’s correlation test was used to assess the relationship between the scores of IHWA and SF-12. Data analysis was done using AMOS software, version 26 and SPSS software, version 22.
Results
In this study, 202 patients with type 2 diabetes completed the Persian IHWA questionnaire. Their demographic and clinical information are reported in Table 1.
The descriptive scores of the IHWA domains are presented in Table 2.
The CVR was 0.96 for the whole scale. For the domains, the value was in the range of 0.57-1. The CVI of all items was higher than 0.83. For all subscales (S-CVI), this value was 0.97, which are acceptable.
To examine the factor structure of the Persian IHWA, the CFA was performed (Figure 1).
The results of the convergent validity test showed that the total score of the IHWA and each of its dimensions had a significant correlation with the total SF-12 score and its dimensions, with a small to large effect size and in the expected direction (Table 3).
These results confirm the convergent validity of the Persian version of the IHWA tool. Cronbach’s α value for the whole questionnaire was calculated as 0.889. Also, the test re-test reliability using the ICC was calculated as 0.833 (Table 4).
These results indicate the good reliability of the Persian IHWA.
Discussion
This study aimed to assess the psychometric properties of the Persian version of the IHWA questionnaire. In the present study, the face validity and content validity of the Persian instrument were confirmed. Similar to the present study, McElligott et al. also confirmed the content validity of the English IHWA tool, where they reported 100% inter-rater agreement [9]. In our study, the values of the fit indices in the CFA for construct validity were within the desired range, indicating that the model had a good fit to the data. The factor loadings in the relationship between domains and items and also the factor loadings between the total score and the domain scores were significant. This is consistent with McElligott et al.’s study for the original version. The Persian IHWA score had a significant positive relationship with the SF-12 score, confirming its convergent validity. The Cronbach’s α coefficients showed high internal consistency, similar to the original version. The appropriate Cronbach’s α in each domain indicates that the items constituting that domain are a suitable representation of the content of that domain [15, 18]. In McElligott et al.’s study, Cronbach’s α was 0.880 [10], which is close to our result. In the present study, the α value was lower in the dimension of life balance/satisfaction. Life satisfaction is a very important factor in the life of a patient with type 2 diabetes and leads to better treatment effects and improvement of the patient’s wellness. In these patients, low levels of life balance and satisfaction may negatively affect self-care behaviors and treatment outcomes. It seems that the reason for the low reliability of this dimension is due to the nature of satisfaction, which may vary from time to time depending on the physical, mental and psychological conditions of the person. It is also can be due to physical and mental conditions caused by the disease or mental and physical stress of nurses due to job conditions. In Iran, a study showed a positive and direct relationship between nutritional behaviors and life satisfaction in diabetic patients [19]. In a study conducted in two countries, Serbia and Poland, most nurses reported moderate life satisfaction. One of the factors predicting life satisfaction that are more prominent is job satisfaction and fatigue of nurses [20]. The highest reliability in the current study was observed in the dimension of relationships, while in McElligott et al.’s study, it was reported in the physical dimension [9]. The results for other dimensions were almost similar. Perhaps the reason for the discrepancy was the different culture, lifestyle, and the study population. In our study, participants were diabetic patients with high blood sugar and different physical conditions. In McElligott et al.’s study, nurses who had high knowledge about the side effects of inactivity, the importance of regular exercise and a healthy diet participated [9]. The increase in the prevalence of diabetes is related to lifestyle changes, including lack of a proper diet, physical activity, and obesity [19]. The IHWA short form has not been translated to other languages, so far, and the psychometric properties of other versions are not available to compare.
Considering the importance of patient- and community-centered evaluations in coaching sessions conducted by the nurse coach, the valid and reliable Persian version of IHWA can be used in all clinical settings in Iran to more accurately and reliably identify the lifestyle of people with type 2 diabetes. In addition, the Persian version of IHWA allows the Iranian nurse coach to conduct a more comprehensive assessment of these patients and evaluate the effects of coaching interventions on them. Since this tool was psychometrically evaluated for diabetic patients in this study and the TINC theory describes comprehensive nursing practice, it is suitable for use in many areas, such as lifestyle, chronic diseases, end-of-life care, etc. [4].
The present study, like other studies, had some disadvantages/limitations. The used instruments were self-report tools, and the study was conducted on diabetic patients in one of the hospitals in Rasht City. The results cannot be generalized to all people with type 2 diabetes in Iran. It is recommended that the validity and reliability of the Persian IHWA should be measured in other populations in Iran such as healthy people and or patients with other chronic patients who need to change their lifestyle for recovery. The Persian IHWA was validated in this study due to the lack of a specific tool to measure the effect of the nurse coach program in patients with type 2 diabetes in Iran. It is a valid and reliable tool that can be used in other studies to measure integrated health and wellness in these patients by nurses or other members of the treatment team. More studies are recommended in other countries to validate this tool for other cultures with different health systems
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of Guilan University of Medical Sciences (Code: IR.GUMS.REC.1399.617). All ethical principles, such as the informed consent from the participants, the confidentiality of their information, and their right to leave the study, were observed in this study.
Funding
This article was funded by the Deputy for Research and Technology of Guilan University of Medical Sciences.
Authors' contributions
Study design: Maryam Rassouli, Zahra Abbasi Ranjbar, Saman Maroufizadeh and Zahra Taheri-Ezbarami; Research: Zahra Taheri-Ezbarami; Data curation: Batoul Alizadeh Taghiabad, Fateme Jafaraghaee, Maryam Rassouli and Zahra Abbasi Ranjbar; Data collection: Batoul Alizadeh Taghiabad, and Fateme Jafaragha; Data analysis: Saman Maroufizadeh; Draft preparation: Batoul Alizadeh Taghiabad, Fateme Jafaraghaee, and Saman Maroufizadeh; Final approval: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors would like to thank the Deputy for Research and Technology of Guilan University of Medical Sciences for their financial support and to thank all patients participated in this study for their cooperation.
References
- Dehvan F, Saeed DM, Dehkordi AH, Gheshlagh RG. Quality of life of Iranian patients with type 2 diabetes: A systematic review and meta-analysis. Nurs Pract Today. 2019; 6(4):167-75. [DOI:10.18502/npt.v6i4.1939]
- Chen RY, Huang LC, Su CT, Chang YT, Chu CL, Chang CL, et al. Effectiveness of short-term health coaching on diabetes control and self-management efficacy: A quasi-experimental trial. Front Public Health. 2019; 7:314. [DOI:10.3389/fpubh.2019.00314] [PMID]
- Noshad S, Afarideh M, Heidari B, Mechanick JI, Esteghamati A. Diabetes care in Iran: Where we stand and where we are headed. Ann Glob Health. 2015; 81(6):839-50. [DOI:10.1016/j.aogh.2015.10.003] [PMID]
- Moore AK, Avino K, McElligott D. Analysis of the theory of integrative nurse coaching. J Holist Nurs. 2022; 40(2):169-80. [DOI:10.1177/08980101211006599] [PMID]
- García-Molina L, Lewis-Mikhael AM, Riquelme-Gallego B, Cano-Ibáñez N, Oliveras-López MJ, Bueno-Cavanillas A. Improving type 2 diabetes mellitus glycaemic control through lifestyle modification implementing diet intervention: A systematic review and meta-analysis. Eur J Nutr. 2020; 59(4):1313-28. [DOI:10.1007/s00394-019-02147-6] [PMID]
- ElSayed NA, Aleppo G, Aroda VR, Bannuru RR, Brown FM, Bruemmer D, et al. 8. Obesity and weight management for the prevention and treatment of type 2 diabetes: Standards of care in diabetes-2023. Diabetes Care. 2023; 46(Suppl 1):S128-39. [DOI:10.2337/dc23-S008] [PMID]
- Dossey B, Luck S. Nurse coaching through a nursing lens: The theory of integrative nurse coaching. Beginnings. 2015; 35(4):10-3, 25. [PMID]
- Dossey BM, Luck S, Schaub BG. Nurse coaching: Integrative approaches for health and wellbeing. Miami: International Nurse Coach Association; 2015. [Link]
- McElligott D, Eckardt S, Montgomery Dossey B, Luck S, Eckardt P. Instrument development of integrative health and wellness assessment™. J Holist Nurs. 2018; 36(4):374-84. [DOI:10.1177/0898010117747752] [PMID]
- McElligott D, Turnier J. Integrative health and wellness assessment tool. Crit Care Nurs Clin North Am. 2020; 32(3):439-50. [DOI:10.1016/j.cnc.2020.05.006] [PMID]
- Dermody E. Nurse coaching: Providing holistic care to patients with cancer. Clin J Oncol Nurs. 2021; 25(3):237-9. [DOI:10.1188/21.CJON.237-239] [PMID]
- Farahani AS, Bussing A, Akbari ME, Ashrafizadeh H, Heidarzadeh M, Hatamipour K, et al. The translation and psychometric evaluation of the Persian version of brief multidimensional life satisfaction scale for Iranian patients with cancer. Int J Cancer Manage. 2021; 14(7):e113588. [DOI:10.5812/ijcm.113588]
- Jackson K, D'Avolio D, Gropper S. Choosing coaching frameworks for promoting diet modifications. Br J Nurs. 2019; 28(22):1456-60. [DOI:10.12968/bjon.2019.28.22.1456] [PMID]
- Beaton DE, Bombardier C, Guillemin F, Ferraz MB. Guidelines for the process of cross-cultural adaptation of self-report measures. Spine. 2000; 25(24):3186-91. [DOI:10.1097/00007632-200012150-00014] [PMID]
- Ebadi A, Sharif Nia H, Zareiyan A, Zarshenas L. [Instrument development in health sciences (Persian)]. Tehran: Jame-e-Negar. 2019. [Link]
- Brown T. CFA with equality constraints, multiple groups, and mean structures. Confirmatory Factor Anal Appl Res. 2006; 1(1):236-319. [Link]
- Montazeri A, Vahdaninia M, Mousavi SJ, Omidvari S. The Iranian version of 12-item short form health survey (SF-12): Factor structure, internal consistency and construct validity. BMC Public Health. 2009; 9:341.[DOI:10.1186/1471-2458-9-341] [PMID]
- Ebadi A, Ausili D, Albatineh AN, Salarvand S, Ghanei Ghashlagh R. Psychometric evaluation of the farsi version of the self-care of diabetes inventory in Iranian patients with diabetes. Diabetes Metab Syndr Obes. 2019; 12:2775-84. [DOI:10.2147/DMSO.S235436] [PMID]
- Rouzbeh P, Pourmovahed Z, Akbarpoor A, Zendedel MH. [The relationship between nutritional behaviors and life satisfaction among individuals with type II diabetes (Persian)]. J Diabetes Nurs 2023; 11(3):2203-14. [Link]
- Milutinović D, Marcinowicz L, Jovanović NB, Dragnić N. Impact of compassion satisfaction and compassion fatigue on satisfaction with life in Serbian and Polish nurses: A cross-sectional study. Int Nurs Rev. 2023; 70(2):194-203. [DOI:10.1111/inr.12793] [PMID]
Article Type : Research |
Subject:
Special
Received: 2023/11/5 | Accepted: 2024/09/13 | Published: 2024/10/1
Received: 2023/11/5 | Accepted: 2024/09/13 | Published: 2024/10/1
Send email to the article author
| Rights and permissions | |
 | This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
