Fri, Jan 30, 2026
Volume 35, Issue 1 (1-2025)
JHNM 2025, 35(1): 71-80 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Amrolahi-Mishavan F, Emami-Sigaroudi A, Jafaraghaee F, Shahsavari H, Maroufizadeh S, Babaeipour-Divshali M. Determinants of Missed Nursing Care for Cardiac Patients in Iran: A Mixed-method Study. JHNM 2025; 35 (1) :71-80
URL: http://hnmj.gums.ac.ir/article-1-2234-en.html
URL: http://hnmj.gums.ac.ir/article-1-2234-en.html
Fatemeh Amrolahi-Mishavan1 

 , Abdolhossein Emami-Sigaroudi *2 , Fatemeh Jafaraghaee3 , Hooman Shahsavari4 , Saman Maroufizadeh5 , Mohammad Babaeipour-Divshali6
, Abdolhossein Emami-Sigaroudi *2 , Fatemeh Jafaraghaee3 , Hooman Shahsavari4 , Saman Maroufizadeh5 , Mohammad Babaeipour-Divshali6
, Abdolhossein Emami-Sigaroudi *2 , Fatemeh Jafaraghaee3 , Hooman Shahsavari4 , Saman Maroufizadeh5 , Mohammad Babaeipour-Divshali6
1- Assistant Professor, Department of Nursing, Zeynab (P.B.U.H) School of Nursing and Midwifery, Guilan University of Medical Sciences, Rasht, Iran.
2- Professor, Department of Cardiology, Cardiovascular Diseases Research Center, School of Medicine, Heshmat Hospital, Guilan University of Medical Sciences, Rasht, Iran. ,emamisig@gmail.com
3- Associated Professor, Department of Medical-Surgical Nursing, School of Nursing and Midwifery, Guilan University of Medical Sciences, Rasht, Iran.
4- Associated Professor, Department of Medical-Surgical Nursing, School of Nursing and Midwifery, Tehran University of Medical Sciences, Tehran, Iran.
5- Assistant Professor, Department of Biostatistics, School of Health, Guilan University of Medical Sciences, Rasht, Iran.
6- Master of Nursing, Guilan University of Medical Sciences, Rasht, Iran.
2- Professor, Department of Cardiology, Cardiovascular Diseases Research Center, School of Medicine, Heshmat Hospital, Guilan University of Medical Sciences, Rasht, Iran. ,
3- Associated Professor, Department of Medical-Surgical Nursing, School of Nursing and Midwifery, Guilan University of Medical Sciences, Rasht, Iran.
4- Associated Professor, Department of Medical-Surgical Nursing, School of Nursing and Midwifery, Tehran University of Medical Sciences, Tehran, Iran.
5- Assistant Professor, Department of Biostatistics, School of Health, Guilan University of Medical Sciences, Rasht, Iran.
6- Master of Nursing, Guilan University of Medical Sciences, Rasht, Iran.
Full-Text [PDF 556 kb]
(466 Downloads)
| Abstract (HTML) (740 Views)
Full-Text: (444 Views)
Introduction
Nursing care has a significant impact on patient outcomes [1-3]. Evidence shows a strong correlation between nursing care and patient recovery [4]. In some situations, nursing care may be missed due to factors such as staff shortages [5]. Missed nursing care refers to delayed or unfinished care [6, 7]. In a study by Hessels et al., the rate of missed nursing care was 10-27% [8], while in Blackman et al.’s study it was 34% [9]. Jones revealed that missed nursing care, as a major issue in hospitals, affects nurses’ care prioritization and results in unmet educational, emotional, and psychological needs, thereby increasing patient vulnerability [10]. Missed nursing care is linked to various negative outcomes, including prolonged hospital stays, decreased patient satisfaction [11], reduced sense of safety in the patient, decline in hospital reputation [12], skin problems, and medication errors [5]. Overall, missed nursing care is a key indicator in assessing the quality of nursing services. Therefore, understanding the factors contributing to missed nursing care and improving nursing practice are crucial [13], especially in cardiac care units (CCUs), where missed nursing care can be dangerous to patients. The factors associated with missed nursing care may vary depending on the study setting and the financial and human resources of the healthcare system [7]. There is scant research on missed nursing care, specifically in CCUs.
Mixed-method studies, which combine qualitative and quantitative approaches, can provide comprehensive and reliable results [14]. Given the importance of nursing care in CCUs and its impact on the recovery of cardiac patients, this study aims to design and evaluate a model of missed nursing care in CCUs. Previously, we conducted two separate studies, a scoping review [15] and a qualitative study [16], to identify factors contributing to missed nursing care. The scoping review highlighted factors such as nurses’ personal and job-related characteristics, workload, job satisfaction, available resources, professional communication, teamwork, work environment, management performance, and the use of technology in patient care delivery. The qualitative study identified factors such as the nurse’s job profile, work-life conflict, clinical competence, cardiac room climate, and organizational management as key determinants of missed nursing care in CCUs. The findings from these two studies are used in the present study.
Materials and Methods
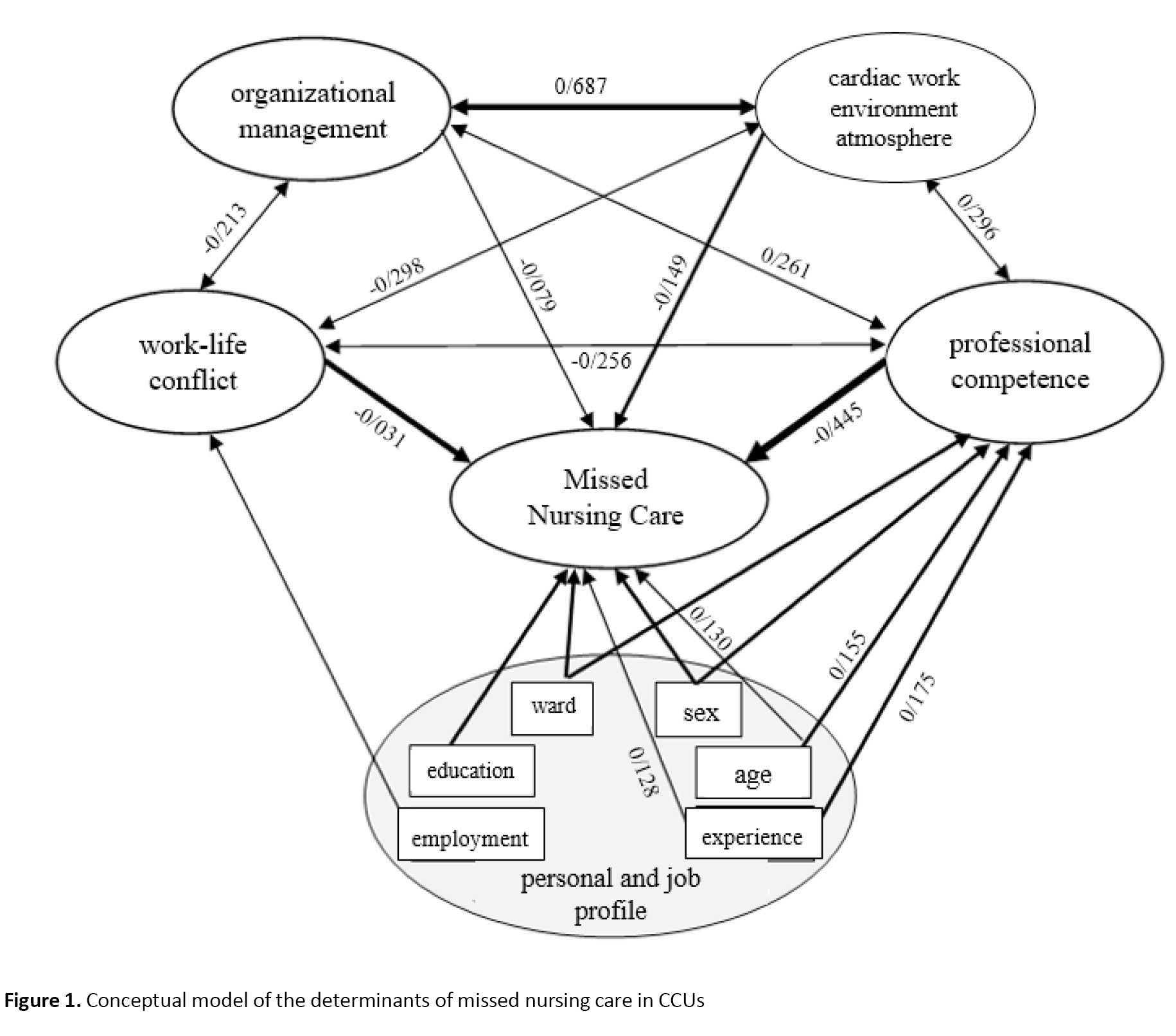
This is a mixed-method study, conducted in two consecutive stages in 2023. In the first stage, results from the scoping review and qualitative studies [15, 16] were integrated using the side-by-side joint display approach. The integration was done by preserving the classifications and findings from the qualitative study, as primary data, while incorporating and consolidating the initial codes from the scoping review. Notably, no data from the scoping review exceeded the data from the qualitative study; all review data were integrated into the qualitative data, resulting in the identification of main themes. These themes were introduced as variables influencing missed nursing care in CCUs, forming the initial model of the determinants of missed nursing care. Figure 1 shows the conceptual model of the study.
 The second stage had an analytical cross-sectional design, conducted from April to June 2023 with the participation of 225 nurses working in the CCUs (two cardiology units, two cardiac surgery units, two intensive care units, two emergency units, post-angiography and electrophysiology units, and pacemaking and Holter monitoring units) of a specialized teaching hospital affiliated with Guilan University of Medical Sciences in Rasht, Iran. Inclusion criteria were having a nursing degree (bachelor’s or higher) and currently working in a CCU. In this stage, based on the developed model, the quantitative data were collected for each variable, and the fit of the proposed model was evaluated, revised, and finalized. Ultimately, the main determinants of missed nursing care in CCUs and the relationships between them were identified.
The second stage had an analytical cross-sectional design, conducted from April to June 2023 with the participation of 225 nurses working in the CCUs (two cardiology units, two cardiac surgery units, two intensive care units, two emergency units, post-angiography and electrophysiology units, and pacemaking and Holter monitoring units) of a specialized teaching hospital affiliated with Guilan University of Medical Sciences in Rasht, Iran. Inclusion criteria were having a nursing degree (bachelor’s or higher) and currently working in a CCU. In this stage, based on the developed model, the quantitative data were collected for each variable, and the fit of the proposed model was evaluated, revised, and finalized. Ultimately, the main determinants of missed nursing care in CCUs and the relationships between them were identified.
The main variable in this study was “missed nursing care”, and five independent variables derived from the integration of the scoping review and qualitative study were nurse’s job profile, work-life conflict, nurse’s clinical competence, cardiac room climate, and organizational management. To assess these variables, the MISSCARE survey (for missed nursing care), the work-family conflict scale (WFCS), and the competency inventory for registered nurse (CIRN) were used. For the three variables of cardiac room climate, organizational management, and nurse’s job profile (personal and job-related), researcher-developed questionnaires were employed due to the lack of related assessment tools.
The MISSCARE survey consists of 24 items that assess missed nursing care by a self-report method using a five-point Likert scale from 1 (never missed) to 5 (always missed). The Persian version of this questionnaire has been previously validated by Chegini et al. [17]. The internal consistency of this instrument in this study using Cronbach’s α was determined as 0.91. The WFCS is an 18-item, 6-factor questionnaire measuring three aspects (time-based, strain-based, and behavior-based) of work-family conflict based on a five-point Likert scale from 1 (strongly disagree) to 5 (strongly agree). The Persian version of this scale was validated by Rajabi et al. [18], and its internal consistency was confirmed with a Cronbach’s α of 0.96. The CIRN is a self-assessment tool with seven subscales and 55 items, measuring the frequency of using each skill on a five-point Likert scale from 0 (never) to 4 (always). This scale was translated and psychometrically evaluated in Iran by Ghasemi et al., who tested it on nursing faculty members and reported its acceptable face validity and content validity (content validity ratio [CVI]=0.94) [19]. In this study, the internal consistency of this tool was determined with a Cronbach’s α of 0.94.
The researcher-made cardiac room climate scale had 15 items and three subscales (management climate, care climate, and professional communication), and the researcher-made organizational management scale had 17 items and four subscales (staff management, resource management, education, and satisfaction). Responses were based on a five-point Likert scale from 1 (strongly disagree) to 5 (strongly agree). To determine their content and face validity, they were examined by 10 nursing faculty members, and their CVR and content validity index (CVI) were calculated. The overall CVI for the cardiac room climate scale was 0.98, with a CVR of 0.95, while the organizational management scale had a CVI of 0.97 and a CVR of 0.95. Test re-test reliability was assessed by administering the questionnaires to 15 CCU nurses twice at a 10-day interval. The results reported interclass correlation coefficients of 0.98 for the cardiac room climate scale and 0.99 for the organizational management scale.
Descriptive and inferential statistics were used to analyze the collected data. The relationship between the main variables was assessed using Pearson’s correlation test. The relationship between missed nursing care scores and nurse’s job profile variables was examined using independent t-tests, one-way ANOVA, and Pearson’s correlation test. Hierarchical multiple linear regression was used to determine factors predicting the missed nursing care. In this regard, the relationship between nurse’s job profile variables and missed nursing care was first evaluated (model 1). Other variables were then added to model 2 to assess the prediction power of the model. Data analysis was conducted in SPSS software, version 16, and the significance level was set at 0.05.
Results
In this study, 202 questionnaires were returned, yielding a response rate of 90%. The demographic and job-related characteristics of the nurses are presented in Table 1.
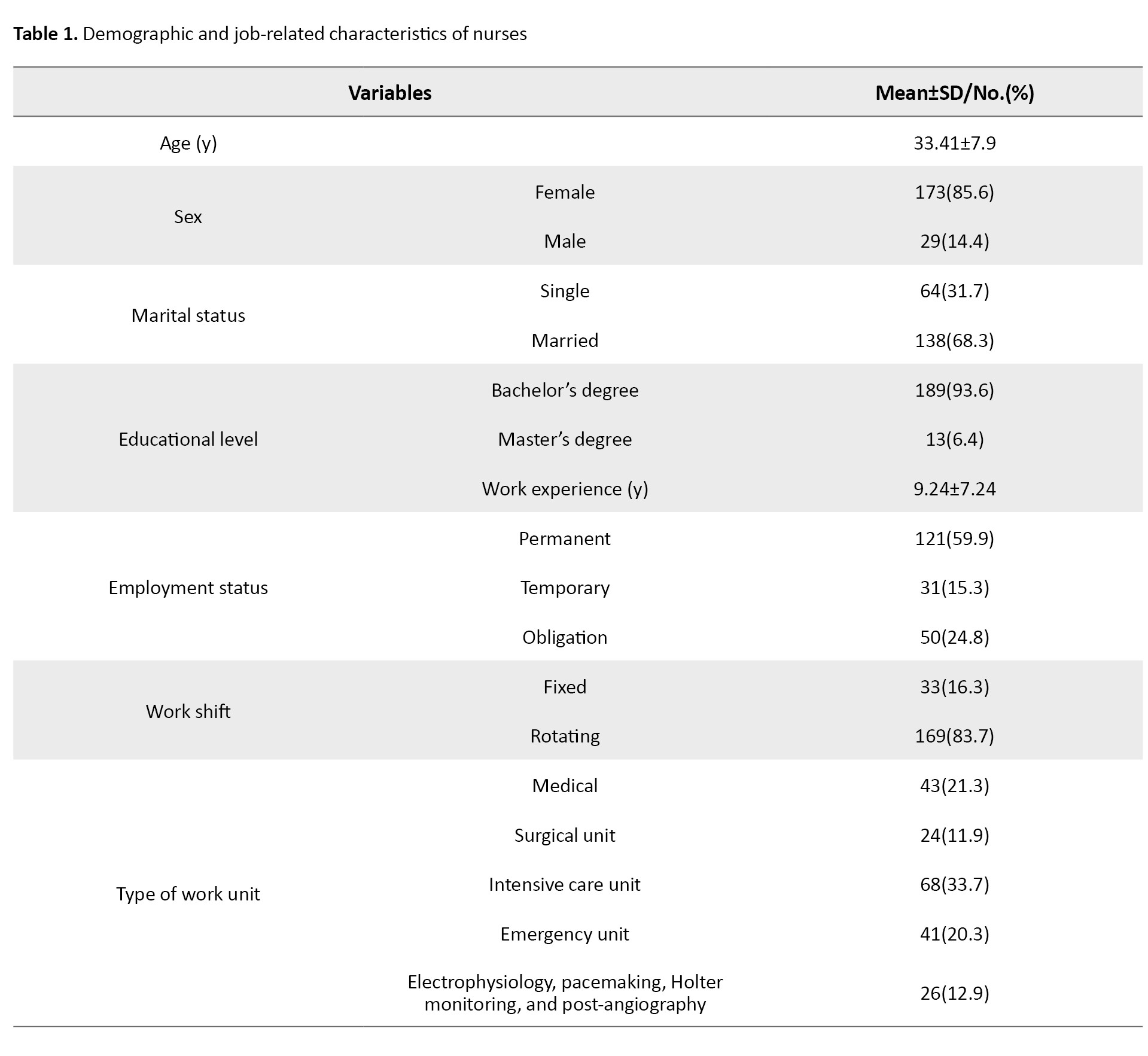
The mean age of the nurses was 33.41±7.9 years, and their mean work experience was 9.24±7.24 years. Among 202 nurses, 29(14.4%) were male, 138(68.3%) were married, and 13(6.4%) had a master’s degree.
The results related to the correlations between the main variables are presented in Table 2.
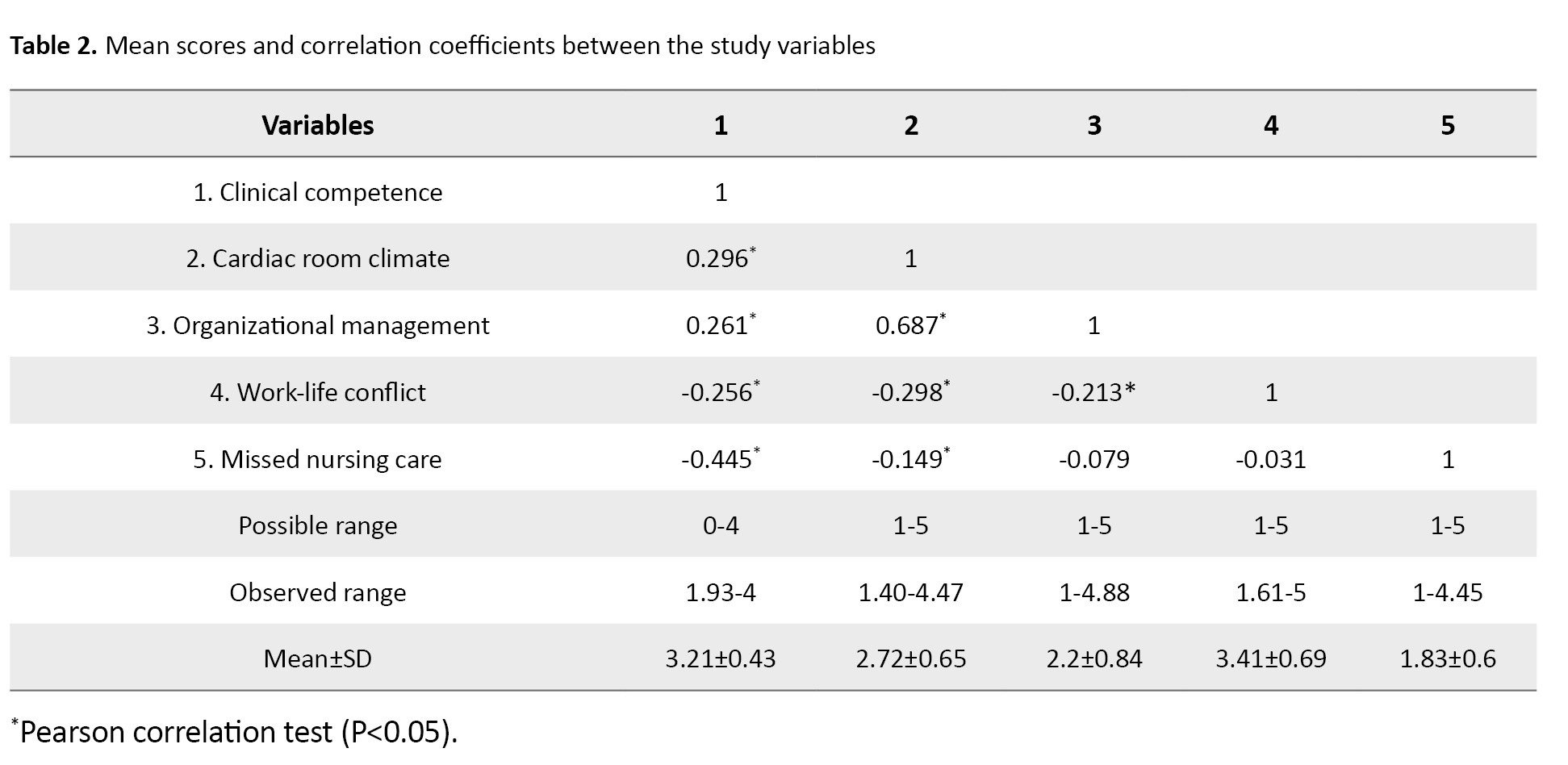
The results showed a significant negative correlation (moderate) between clinical competence and missed nursing care (r=-0.445, P=0.001). The cardiac room climate had a weak but significant negative correlation with missed nursing care (r=-0.149, P=0.035) and work-family conflict (r=-0.298, P=0.001), and a strong significant positive correlation with organizational management (r=0.687, P=0.001).
Table 3 shows the results related to the relationship of demographic and job-related characteristics with missed nursing care scores.
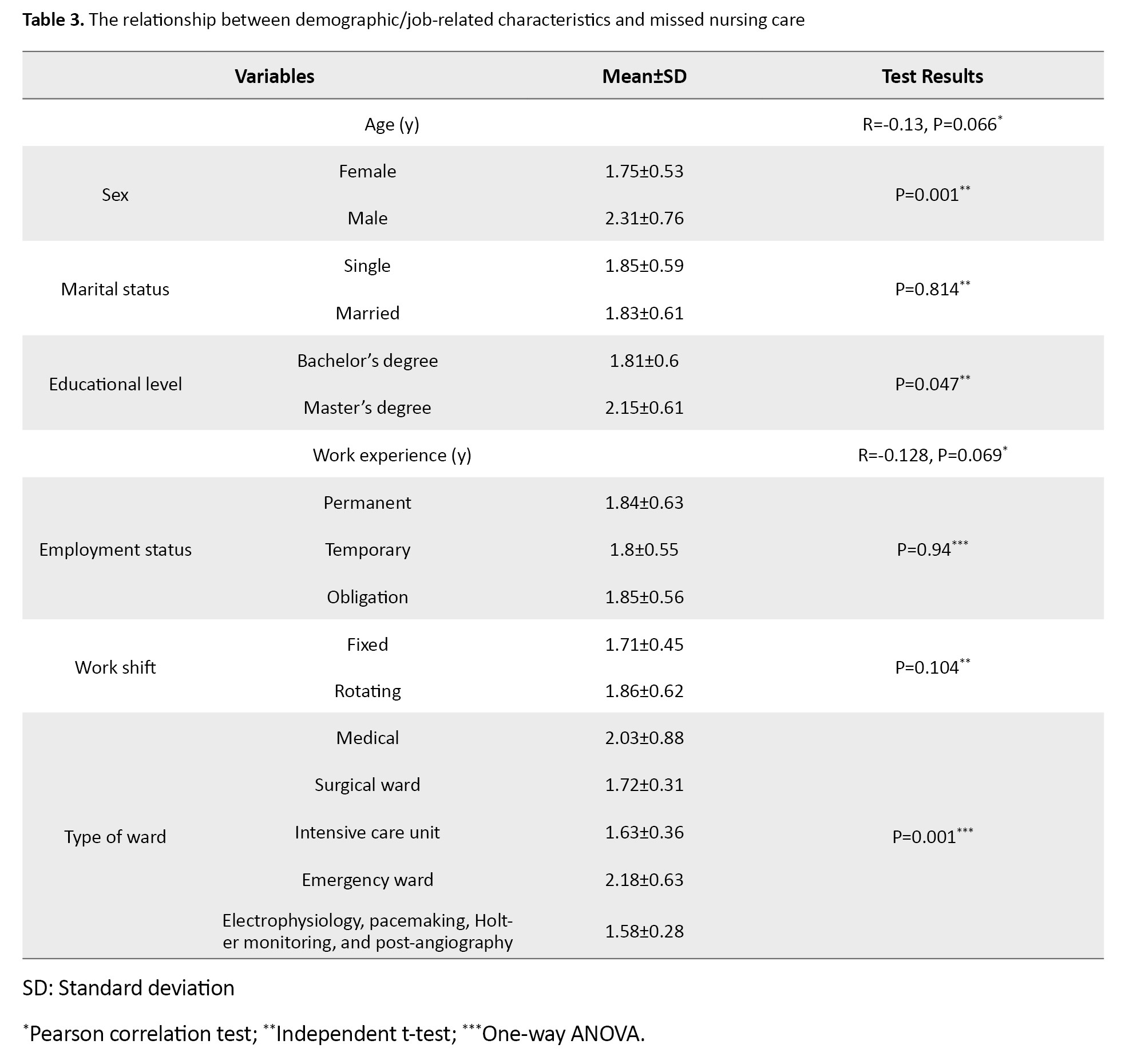
As can be seen, male nurses had significantly higher missed nursing care scores than female nurses (P=0.001). Nurses with a master’s degree had significantly higher missed care scores than those with a bachelor’s degree (P=0.047). Furthermore, a significant difference in missed nursing care scores was observed based on the type of unit where the nurses worked (P=0.001).
Table 4 presents the factors in the linear regression model.
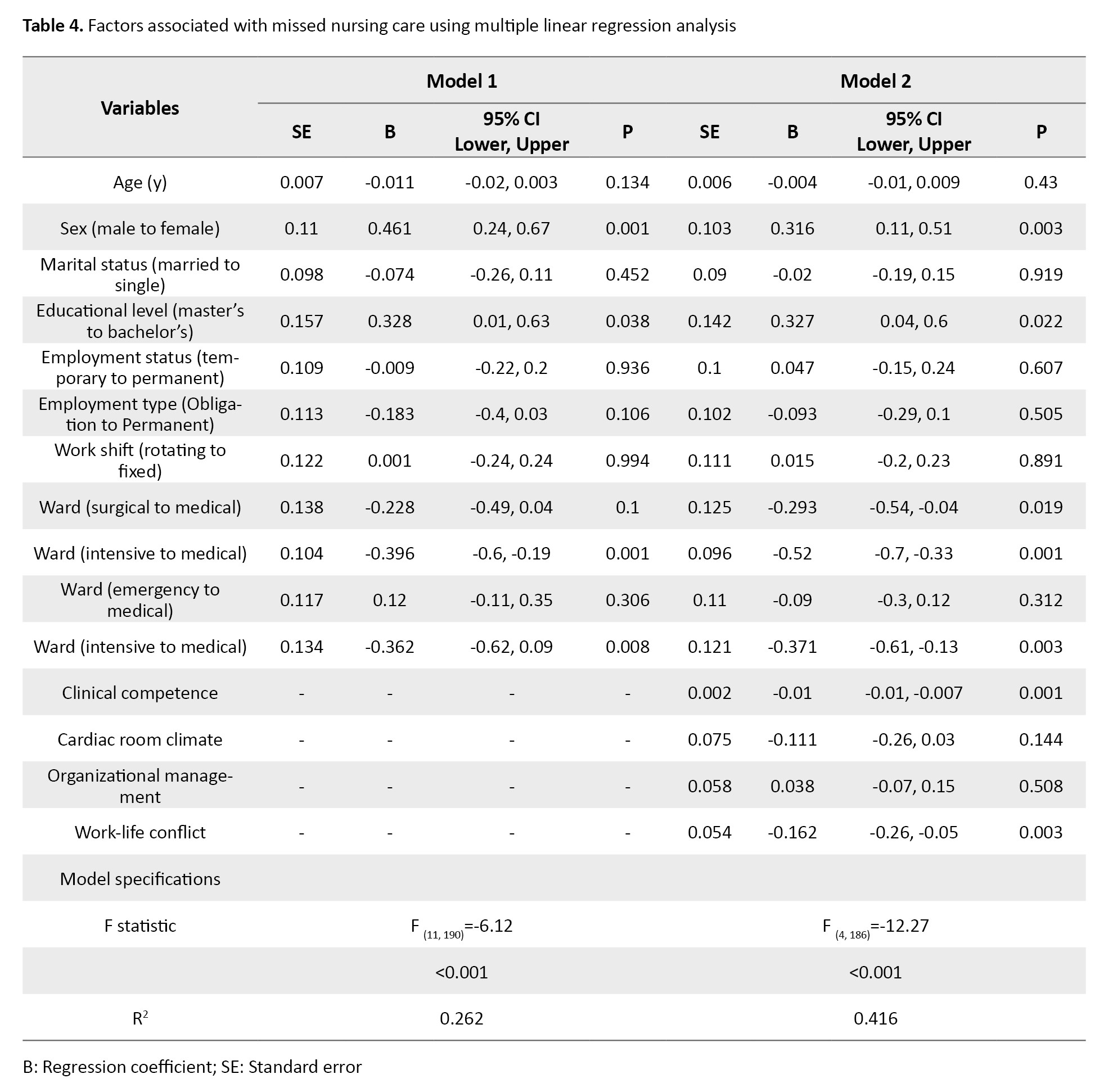
Based on the findings for model 1, missed nursing care was more likely in male nurses than in female nurses by 0.461 units (β=0.461, 95%CI; 0.243%, 0.679%, P=0.001). Nurses with a master’s degree were more likely to report missed nursing care than those with a bachelor’s degree by 0.328 units (β=0.328, 95%CI; 0.019%, 0.637%, P=0.038). Compared to nurses working in internal medicine wards, those in intensive care units (β=-0.396, 95%CI; -0.601%, -0.190%, P<0.001) and invasive units (β=-0.362, 95%CI; -0.627%, -0.096%, P=0.008) were less likely to report missed nursing care. The coefficient of determination (R²) for the model included demographic and job-related characteristics was 0.262, indicating that these variables can explain 26.2% of the variance in missed nursing care.
In model 2, the results showed that clinical competence was significantly associated with missed nursing care. For each one-unit increase in clinical competence, the overall missed nursing care score decreased by 0.01 units (β=-0.010, 95%CI; -0.014%, -0.007%, P<0.001). An increase in work-family conflict was also significantly associated with reduced missed nursing care (β=-0.162, 95%CI; -0.269%, -0.055%, P=0.003). When the variables of clinical competence, work-family conflict, organizational management, and cardiac room climate were added to the regression model, there was a significant increase of 15.4% in the R2 value. In model 2, the variables explained 41.6% of the variance in missed nursing care.
Discussion
The purpose of this study was to identify the determinants of missed nursing care in the CCUs of hospitals in Iran using a mixed-method approach. Based on our previous studies, factors such as nurse demographic/job-related characteristics, work-life conflict, clinical competence, cardiac room climate, and organizational management were considered as the components of the model of the determinants of missed nursing care.
The results indicated a significant relationship between some demographic/job-related characteristics of nurses (such as sex, educational level, and type of unit where they worked) and missed nursing care. It was found that male nurses had a higher rate of missed nursing care than female nurses. This finding is consistent with the results of Vatankhah et al., who also reported higher missed nursing care among male nurses. They suggested that fatigue (due to long work hours and shiftwork) and financial concerns may contribute to the higher missed nursing care in male nurses [20]. In our study, nurses with master’s degrees had higher rates of missed nursing care than those with bachelor’s degrees, consistent with the results of Ebadi et al. [21]. This may be explained by the higher career expectations of nurses having higher degrees; when these expectations are not met, it can reduce their motivation. Furthermore, due to their involvement in research and educational activities, they may have a lower clinical focus, affecting their bedside performance. We also found that nurses in internal medicine units had lower rates of missed nursing care than those in other units, which is consistent with previous studies that reported different missed nursing care rates across different units [1, 22, 23]. The workload may contribute to more missed nursing care in these highly stressful units. Our results also showed that missed nursing care decreased with the increase of age and years of work experience, but this correlation was not statistically significant. Srulovici and Drach-Zahavy found no significant relationship between missed nursing care and age and work experience, either [24].
Multivariate regression analysis revealed that higher work-life conflict was significantly associated with lower missed nursing care. This suggests that nurses often prioritize their job duties over their family roles, which may lead to less missed nursing care but greater work-life conflict. This is consistent with previous studies, which indicated that work has a greater impact on family responsibilities compared to the effect of family responsibilities on work [25-28]. In the Iranian culture, the supportive role of family, such as care and emotional supports, may help reduce work-life conflict, allowing nurses to focus more on their work tasks. The regression model also showed that increased clinical competence was significantly associated with reduced missed nursing care. In a similar study, Chang and Manojlovich found that higher nursing competency was linked to lower rates of missed nursing care [29]. Nobahar also reported the negative impact of inadequate nursing competency, particularly in areas such as recognizing patient deterioration and handling equipment, on the quality of cardiac care [30]. Given that the strongest predictor of missed nursing care in our study was clinical competence, it can be a key determinant of missed nursing care in cardiac patients.
The results also indicated that the cardiac room climate significantly affected nurse performance and missed nursing care. Due to the nature of cardiac diseases, the patient care needs, and the stressful environment of CCUs, nurses may prioritize specific tasks which can lead to missing some of them. Although the univariate data analysis results showed a weak negative correlation between cardiac room climate and missed nursing care, this relationship was not significant in multivariate data analysis, possibly due to the small sample size. Similar findings were reported by Ibrahim and Abohabieb [31], but Lake et al.’s study suggested a correlation between improved work environment and reduced missed nursing care [32]. Several other studies have reported similar findings [33-35], confirming that the work environment is still essential in determining missed nursing care.
Finally, we identified a weak negative correlation between organizational management and missed nursing care, but it was not statistically significant in either univariate or multivariate data analyses, potentially due to the small sample size or nurses’ fatigue. Proper management and leadership are critical in ensuring optimal nursing care. Kim et al. identified effective nursing leadership and support as factors affecting missed nursing care [34]. Therefore, despite a non-significant correlation, organizational management remains crucial in determining missed nursing care.
The missed nursing care in CCUs of hospitals in Iran is associated with nurses’ sex, educational level, and the type of work unit. Additionally, increased work-life conflict and clinical competence can predict decreased missed nursing care. The mentioned demographic/job-related variables explained 26.2% of the variance in missed nursing care. By considering work-life conflict and clinical competence, the variance in missed nursing care was explained by 41.6%. This suggests that there may be other factors that have a role in missed nursing care for cardiac patients in Iran. Healthcare managers in Iran should pay attention to the demographic and job-related characteristics of nurses working in CCUs and develop strategies to reduce their work-life conflict and improve their clinical competence for controlling the incidence of missed nursing care in CCUs.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of Guilan University of Medical Sciences Rasht, Iran (Code: IR.GUMS.REC.1400.005). Participation in the study was voluntary, and informed consent to participate in the research was obtained from all participants.
Funding
This study was extracted from a PhD dissertation, that received approval and funding from Guilan University of Medical Sciences, Rasht, Iran.
Authors' contributions
Conceptualization and study design: Abdolhossein Emami-Sigaroudi, Fatemeh Amrolahi-Mishavan, Fatemeh Jafaraghaee, Hooman Shahsavari, Saman Maroufizadeh; Data acquisition, analysis, and interpretation: Fatemeh Amrolahi-Mishavan, Abdolhossein Emami-Sigaroudi, Fatemeh Jafaraghaee, Hooman Shahsavari, Mohammad Babaeipour-Divshali; Writing the original draft: Fatemeh Amrolahi-Mishavan and Mohammad Babaeipour-Divshali; Supervision, administrative, technical, or material support, review and editing: Abdolhossein Emami-Sigaroudi, Fatemeh Jafaraghaee, Hooman Shahsavari, and Saman Maroufizadeh.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors would like to thank all the nurses who participated in this study for their cooperation and the Vice-Chancellor for Research and Technology of Guilan University of Medical Sciences, Rasht Iran, for their financial support.
References
Nursing care has a significant impact on patient outcomes [1-3]. Evidence shows a strong correlation between nursing care and patient recovery [4]. In some situations, nursing care may be missed due to factors such as staff shortages [5]. Missed nursing care refers to delayed or unfinished care [6, 7]. In a study by Hessels et al., the rate of missed nursing care was 10-27% [8], while in Blackman et al.’s study it was 34% [9]. Jones revealed that missed nursing care, as a major issue in hospitals, affects nurses’ care prioritization and results in unmet educational, emotional, and psychological needs, thereby increasing patient vulnerability [10]. Missed nursing care is linked to various negative outcomes, including prolonged hospital stays, decreased patient satisfaction [11], reduced sense of safety in the patient, decline in hospital reputation [12], skin problems, and medication errors [5]. Overall, missed nursing care is a key indicator in assessing the quality of nursing services. Therefore, understanding the factors contributing to missed nursing care and improving nursing practice are crucial [13], especially in cardiac care units (CCUs), where missed nursing care can be dangerous to patients. The factors associated with missed nursing care may vary depending on the study setting and the financial and human resources of the healthcare system [7]. There is scant research on missed nursing care, specifically in CCUs.
Mixed-method studies, which combine qualitative and quantitative approaches, can provide comprehensive and reliable results [14]. Given the importance of nursing care in CCUs and its impact on the recovery of cardiac patients, this study aims to design and evaluate a model of missed nursing care in CCUs. Previously, we conducted two separate studies, a scoping review [15] and a qualitative study [16], to identify factors contributing to missed nursing care. The scoping review highlighted factors such as nurses’ personal and job-related characteristics, workload, job satisfaction, available resources, professional communication, teamwork, work environment, management performance, and the use of technology in patient care delivery. The qualitative study identified factors such as the nurse’s job profile, work-life conflict, clinical competence, cardiac room climate, and organizational management as key determinants of missed nursing care in CCUs. The findings from these two studies are used in the present study.
Materials and Methods
This is a mixed-method study, conducted in two consecutive stages in 2023. In the first stage, results from the scoping review and qualitative studies [15, 16] were integrated using the side-by-side joint display approach. The integration was done by preserving the classifications and findings from the qualitative study, as primary data, while incorporating and consolidating the initial codes from the scoping review. Notably, no data from the scoping review exceeded the data from the qualitative study; all review data were integrated into the qualitative data, resulting in the identification of main themes. These themes were introduced as variables influencing missed nursing care in CCUs, forming the initial model of the determinants of missed nursing care. Figure 1 shows the conceptual model of the study.
The main variable in this study was “missed nursing care”, and five independent variables derived from the integration of the scoping review and qualitative study were nurse’s job profile, work-life conflict, nurse’s clinical competence, cardiac room climate, and organizational management. To assess these variables, the MISSCARE survey (for missed nursing care), the work-family conflict scale (WFCS), and the competency inventory for registered nurse (CIRN) were used. For the three variables of cardiac room climate, organizational management, and nurse’s job profile (personal and job-related), researcher-developed questionnaires were employed due to the lack of related assessment tools.
The MISSCARE survey consists of 24 items that assess missed nursing care by a self-report method using a five-point Likert scale from 1 (never missed) to 5 (always missed). The Persian version of this questionnaire has been previously validated by Chegini et al. [17]. The internal consistency of this instrument in this study using Cronbach’s α was determined as 0.91. The WFCS is an 18-item, 6-factor questionnaire measuring three aspects (time-based, strain-based, and behavior-based) of work-family conflict based on a five-point Likert scale from 1 (strongly disagree) to 5 (strongly agree). The Persian version of this scale was validated by Rajabi et al. [18], and its internal consistency was confirmed with a Cronbach’s α of 0.96. The CIRN is a self-assessment tool with seven subscales and 55 items, measuring the frequency of using each skill on a five-point Likert scale from 0 (never) to 4 (always). This scale was translated and psychometrically evaluated in Iran by Ghasemi et al., who tested it on nursing faculty members and reported its acceptable face validity and content validity (content validity ratio [CVI]=0.94) [19]. In this study, the internal consistency of this tool was determined with a Cronbach’s α of 0.94.
The researcher-made cardiac room climate scale had 15 items and three subscales (management climate, care climate, and professional communication), and the researcher-made organizational management scale had 17 items and four subscales (staff management, resource management, education, and satisfaction). Responses were based on a five-point Likert scale from 1 (strongly disagree) to 5 (strongly agree). To determine their content and face validity, they were examined by 10 nursing faculty members, and their CVR and content validity index (CVI) were calculated. The overall CVI for the cardiac room climate scale was 0.98, with a CVR of 0.95, while the organizational management scale had a CVI of 0.97 and a CVR of 0.95. Test re-test reliability was assessed by administering the questionnaires to 15 CCU nurses twice at a 10-day interval. The results reported interclass correlation coefficients of 0.98 for the cardiac room climate scale and 0.99 for the organizational management scale.
Descriptive and inferential statistics were used to analyze the collected data. The relationship between the main variables was assessed using Pearson’s correlation test. The relationship between missed nursing care scores and nurse’s job profile variables was examined using independent t-tests, one-way ANOVA, and Pearson’s correlation test. Hierarchical multiple linear regression was used to determine factors predicting the missed nursing care. In this regard, the relationship between nurse’s job profile variables and missed nursing care was first evaluated (model 1). Other variables were then added to model 2 to assess the prediction power of the model. Data analysis was conducted in SPSS software, version 16, and the significance level was set at 0.05.
Results
In this study, 202 questionnaires were returned, yielding a response rate of 90%. The demographic and job-related characteristics of the nurses are presented in Table 1.
The mean age of the nurses was 33.41±7.9 years, and their mean work experience was 9.24±7.24 years. Among 202 nurses, 29(14.4%) were male, 138(68.3%) were married, and 13(6.4%) had a master’s degree.
The results related to the correlations between the main variables are presented in Table 2.
The results showed a significant negative correlation (moderate) between clinical competence and missed nursing care (r=-0.445, P=0.001). The cardiac room climate had a weak but significant negative correlation with missed nursing care (r=-0.149, P=0.035) and work-family conflict (r=-0.298, P=0.001), and a strong significant positive correlation with organizational management (r=0.687, P=0.001).
Table 3 shows the results related to the relationship of demographic and job-related characteristics with missed nursing care scores.
As can be seen, male nurses had significantly higher missed nursing care scores than female nurses (P=0.001). Nurses with a master’s degree had significantly higher missed care scores than those with a bachelor’s degree (P=0.047). Furthermore, a significant difference in missed nursing care scores was observed based on the type of unit where the nurses worked (P=0.001).
Table 4 presents the factors in the linear regression model.
Based on the findings for model 1, missed nursing care was more likely in male nurses than in female nurses by 0.461 units (β=0.461, 95%CI; 0.243%, 0.679%, P=0.001). Nurses with a master’s degree were more likely to report missed nursing care than those with a bachelor’s degree by 0.328 units (β=0.328, 95%CI; 0.019%, 0.637%, P=0.038). Compared to nurses working in internal medicine wards, those in intensive care units (β=-0.396, 95%CI; -0.601%, -0.190%, P<0.001) and invasive units (β=-0.362, 95%CI; -0.627%, -0.096%, P=0.008) were less likely to report missed nursing care. The coefficient of determination (R²) for the model included demographic and job-related characteristics was 0.262, indicating that these variables can explain 26.2% of the variance in missed nursing care.
In model 2, the results showed that clinical competence was significantly associated with missed nursing care. For each one-unit increase in clinical competence, the overall missed nursing care score decreased by 0.01 units (β=-0.010, 95%CI; -0.014%, -0.007%, P<0.001). An increase in work-family conflict was also significantly associated with reduced missed nursing care (β=-0.162, 95%CI; -0.269%, -0.055%, P=0.003). When the variables of clinical competence, work-family conflict, organizational management, and cardiac room climate were added to the regression model, there was a significant increase of 15.4% in the R2 value. In model 2, the variables explained 41.6% of the variance in missed nursing care.
Discussion
The purpose of this study was to identify the determinants of missed nursing care in the CCUs of hospitals in Iran using a mixed-method approach. Based on our previous studies, factors such as nurse demographic/job-related characteristics, work-life conflict, clinical competence, cardiac room climate, and organizational management were considered as the components of the model of the determinants of missed nursing care.
The results indicated a significant relationship between some demographic/job-related characteristics of nurses (such as sex, educational level, and type of unit where they worked) and missed nursing care. It was found that male nurses had a higher rate of missed nursing care than female nurses. This finding is consistent with the results of Vatankhah et al., who also reported higher missed nursing care among male nurses. They suggested that fatigue (due to long work hours and shiftwork) and financial concerns may contribute to the higher missed nursing care in male nurses [20]. In our study, nurses with master’s degrees had higher rates of missed nursing care than those with bachelor’s degrees, consistent with the results of Ebadi et al. [21]. This may be explained by the higher career expectations of nurses having higher degrees; when these expectations are not met, it can reduce their motivation. Furthermore, due to their involvement in research and educational activities, they may have a lower clinical focus, affecting their bedside performance. We also found that nurses in internal medicine units had lower rates of missed nursing care than those in other units, which is consistent with previous studies that reported different missed nursing care rates across different units [1, 22, 23]. The workload may contribute to more missed nursing care in these highly stressful units. Our results also showed that missed nursing care decreased with the increase of age and years of work experience, but this correlation was not statistically significant. Srulovici and Drach-Zahavy found no significant relationship between missed nursing care and age and work experience, either [24].
Multivariate regression analysis revealed that higher work-life conflict was significantly associated with lower missed nursing care. This suggests that nurses often prioritize their job duties over their family roles, which may lead to less missed nursing care but greater work-life conflict. This is consistent with previous studies, which indicated that work has a greater impact on family responsibilities compared to the effect of family responsibilities on work [25-28]. In the Iranian culture, the supportive role of family, such as care and emotional supports, may help reduce work-life conflict, allowing nurses to focus more on their work tasks. The regression model also showed that increased clinical competence was significantly associated with reduced missed nursing care. In a similar study, Chang and Manojlovich found that higher nursing competency was linked to lower rates of missed nursing care [29]. Nobahar also reported the negative impact of inadequate nursing competency, particularly in areas such as recognizing patient deterioration and handling equipment, on the quality of cardiac care [30]. Given that the strongest predictor of missed nursing care in our study was clinical competence, it can be a key determinant of missed nursing care in cardiac patients.
The results also indicated that the cardiac room climate significantly affected nurse performance and missed nursing care. Due to the nature of cardiac diseases, the patient care needs, and the stressful environment of CCUs, nurses may prioritize specific tasks which can lead to missing some of them. Although the univariate data analysis results showed a weak negative correlation between cardiac room climate and missed nursing care, this relationship was not significant in multivariate data analysis, possibly due to the small sample size. Similar findings were reported by Ibrahim and Abohabieb [31], but Lake et al.’s study suggested a correlation between improved work environment and reduced missed nursing care [32]. Several other studies have reported similar findings [33-35], confirming that the work environment is still essential in determining missed nursing care.
Finally, we identified a weak negative correlation between organizational management and missed nursing care, but it was not statistically significant in either univariate or multivariate data analyses, potentially due to the small sample size or nurses’ fatigue. Proper management and leadership are critical in ensuring optimal nursing care. Kim et al. identified effective nursing leadership and support as factors affecting missed nursing care [34]. Therefore, despite a non-significant correlation, organizational management remains crucial in determining missed nursing care.
The missed nursing care in CCUs of hospitals in Iran is associated with nurses’ sex, educational level, and the type of work unit. Additionally, increased work-life conflict and clinical competence can predict decreased missed nursing care. The mentioned demographic/job-related variables explained 26.2% of the variance in missed nursing care. By considering work-life conflict and clinical competence, the variance in missed nursing care was explained by 41.6%. This suggests that there may be other factors that have a role in missed nursing care for cardiac patients in Iran. Healthcare managers in Iran should pay attention to the demographic and job-related characteristics of nurses working in CCUs and develop strategies to reduce their work-life conflict and improve their clinical competence for controlling the incidence of missed nursing care in CCUs.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of Guilan University of Medical Sciences Rasht, Iran (Code: IR.GUMS.REC.1400.005). Participation in the study was voluntary, and informed consent to participate in the research was obtained from all participants.
Funding
This study was extracted from a PhD dissertation, that received approval and funding from Guilan University of Medical Sciences, Rasht, Iran.
Authors' contributions
Conceptualization and study design: Abdolhossein Emami-Sigaroudi, Fatemeh Amrolahi-Mishavan, Fatemeh Jafaraghaee, Hooman Shahsavari, Saman Maroufizadeh; Data acquisition, analysis, and interpretation: Fatemeh Amrolahi-Mishavan, Abdolhossein Emami-Sigaroudi, Fatemeh Jafaraghaee, Hooman Shahsavari, Mohammad Babaeipour-Divshali; Writing the original draft: Fatemeh Amrolahi-Mishavan and Mohammad Babaeipour-Divshali; Supervision, administrative, technical, or material support, review and editing: Abdolhossein Emami-Sigaroudi, Fatemeh Jafaraghaee, Hooman Shahsavari, and Saman Maroufizadeh.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors would like to thank all the nurses who participated in this study for their cooperation and the Vice-Chancellor for Research and Technology of Guilan University of Medical Sciences, Rasht Iran, for their financial support.
References
- Ball JE, Murrells T, Rafferty AM, Morrow E, Griffiths P. ‘Care left undone’during nursing shifts: Associations with workload and perceived quality of care. BMJ Qual Saf. 2014; 23(2):116-25. [DOI:10.1136/bmjqs-2012-001767] [PMID]
- Cho SH, Yun SC. Bed-to-nurse ratios, provision of basic nursing care, and in-hospital and 30-day mortality among acute stroke patients admitted to an intensive care unit: Cross-sectional analysis of survey and administrative data. Int J Nurs Stud. 2009; 46(8):1092-101. [DOI:10.1016/j.ijnurstu.2009.02.001] [PMID]
- Kalisch BJ, Lee KH. Missed nursing care: Magnet versus non-Magnet hospitals. Nurs Outlook. 2012 ;60(5):e32-9. [DOI:10.1016/j.outlook.2012.04.006] [PMID]
- Duffy JR. Implementing the Quality-Caring Model in acute care. J Nurs Adm. 2005; 35(1):4-6. [DOI:10.1097/00005110-200501000-00002] [PMID]
- John ME, Mgbekem MA, Nsemo AD, Maxwell GI. Missed nursing care, patient outcomes and care outcomes in selected hospitals in Southern Nigeria. J Nurs Healthc. 2016; 1(2):1-5. [DOI:10.33140/JNH]
- Kalisch BJ, Landstrom GL, Hinshaw AS. Missed nursing care: A concept analysis. J Adv Nurs. 2009; 65(7):1509-17. [DOI:10.1111/j.1365-2648.2009.05027.x] [PMID]
- Khajooee R, Bagherian B, Dehghan M, Azizzadeh Forouzi M. [Missed nursing care and its related factors from the points of view of nurses affiliated to Kerman University of Medical Sciences in 2017 (Persian)]. J Hayat. 2019; 25(1):11-24. [Link]
- Hessels AJ, Flynn L, Cimiotti JP, Cadmus E, Gershon RR. The impact of the nursing practice environment on missed nursing care. Clin Nurs Stud. 2015; 3(4):60-5. [DOI:10.5430%2Fcns.v3n4p60] [PMID]
- Blackman I, Henderson J, Willis E, Hamilton P, Toffoli L, Verrall C, et al. Factors influencing why nursing care is missed. J Clin Nurs. 2015; 24(1-2):47-56. [DOI:10.1111/jocn.12688] [PMID]
- Jones TL, Hamilton P, Murry N. Unfinished nursing care, missed care, and implicitly rationed care: State of the science review. Int J Nurs Stud. 2015; 52(6):1121-37. [DOI:10.1016/j.ijnurstu.2015.02.012] [PMID]
- Lake ET, Germack HD, Viscardi MK. Missed nursing care is linked to patient satisfaction: A cross-sectional study of US hospitals. BMJ Qual Saf. 2016; 25(7):535-43. [DOI:10.1136/bmjqs-2015-003961] [PMID]
- Ball J, Griffiths P. Missed nursing care: A key measure for patient safety. Maryland: Agency for Healthcare Research and Quality, PSNet; 2018. [Link]
- Yaghoubi M, Ebrahimi-Torki M, Salesi M, EhsaniChimeh E, Bahadori M. [The relationship between teamwork and missed nursing Care: Case study in a military hospital in Tehran (Persian)]. J Mil Med. 2019; 21(1):63-72. [Link]
- Sajjadi M, Rassouli M, Abbaszadeا A, Alavi Majd H. [Mixed methods research: Typology (Persian)]. Middle East J Disabil Stud. 2013; 3(2):54-66. [Link]
- Amrolahi-Mishavan F, Emami-Sigaroudi A, Jafaraghaee F, Shahsavari H, Maroufizadeh S. Factors affecting missed nursing care in hospitals: A scoping review. Health Sci Rev. 2022; 4:100053. [DOI:10.1016/j.hsr.2022.100053]
- Amrolahi-Mishavan F, Emami-Sigaroudi A, Jafaraghaee F, Shahsavari H, Maroufizadeh S, Babaeipour-Divshali M. Exploring factors affecting missed nursing care in cardiovascular care units: A qualitative study. Iran J Nurs Midwifery Res. 2024; 29(1):133-9. [DOI:10.4103/ijnmr.ijnmr_133_23] [PMID]
- Chegini Z, Jafari-Koshki T, Kheiri M, Behforoz A, Aliari S, Mitra U, et al. Missed nursing care and related factors in Iranian Hospitals: A cross sectional survey. J Nurs Manag. 2020; 28(8):2205-15.[DOI:10.1111/jonm.13055] [PMID]
- Rajabi G, Makki E, Aslani K. [Reliability and validity of the Persian version of Work-Family Conflict Scale (Persian)]. Payesh. 2020; 19(4):435-44. [DOI:10.29252/payesh.19.4.435]
- Ghasemi E, Janani L, Dehghan Nayeri N, Negarandeh R. [Psychometric properties of Persian version of the Competency Inventory for Registered Nurse (CIRN) (Persian)]. Iran J Nurs. 2014; 27(87):1-13. [DOI:10.29252/ijn.27.87.1]
- Vatankhah I, Rezaei M, Baljani E. [The correlation of missed nursing care and perceived supervisory support in nurses (Persian)]. Iran J Nurs. 2020; 33(126):103-16. [DOI:10.52547/ijn.33.126.103]
- Ebadi J, Najafi E, Aghamohammadi V, Saeeidi S, Nasiri K. [Missed nursing care and its related factors in Ardabil and Khalkhal Educational and Medical Centers in 2020 (Persian)]. J Health Care. 2021; 23(1):78-87. [DOI:10.52547/jhc.23.1.78]
- Bragadóttir H, Kalisch BJ, Tryggvadóttir GB. Correlates and predictors of missed nursing care in hospitals. J Clin Nurs. 2017; 26(11-12):1524-34. [DOI:10.1111/jocn.13449] [PMID]
- Kalisch BJ, Lee KH. The impact of teamwork on missed nursing care. Nurs Outlook. 2010; 58(5):233-41. [DOI:10.1016/j.outlook.2010.06.004] [PMID]
- Srulovici E, Drach-Zahavy A. Nurses’ personal and ward accountability and missed nursing care: A cross-sectional study. Int J Nurs Stud. 2017; 75:163-71. [DOI:10.1016/j.ijnurstu.2017.08.003] [PMID]
- Mousavinia S, Naami A, Arshadi N, Beshlideh K. [The role of work-self facilitation and work-family conflict self-efficacy in decreasing effect of work-family conflicton family satisfaction, couple relationship quality and parenting quality in nurses (Persian)]. Iran J Nurs Res. 2021; 15(6):105-20. [Link]
- Bolandian Bafghi S, Sharifi K. [Work-family conflict in Iranian Nurses: A systematic review (Persian)]. Iran J Nurs Res. 2020; 14(6):53-60. [Link]
- Majomi P, Brown B, Crawford P. Sacrificing the personal to the professional: Community mental health nurses. J Adv Nurs. 2003; 42(5):527-38. [DOI:10.1046/j.1365-2648.2003.02652.x] [PMID]
- Tavangar H, Alhani F, Vanaki Z. [Decline of self-efficacy: The consequence of nursing work-family conflict (Persian)]. Journal of Qualitative Research in Health Sciences. 2012; 1(2):135-47. [Link]
- Chang HE, Manojlovich M. Clinical nurses’ patient safety competency, systems thinking and missed nursing care: A cross-sectional survey. Int J Nurs Pract. 2023; 29(2):e13130. [DOI:10.1111/ijn.13130] [PMID]
- Nobahar M. [Care quality in critical cardiac units from nurses perspective: A content analysis (Persian)]. J Qual Res Health Sci. 2014; 3(2):149-61. [Link]
- Ibrahim IA, Abohabieb EE. Associations between nursing work environment, patient safety culture, and missed nursing care among staff nurses. Port Said Sci JNurs. 2020; 7(3):265-84. [DOI:10.21608/pssjn.2021.50276.1065]
- Lake ET, Riman KA, Sloane DM. Improved work environments and staffing lead to less missed nursing care: A panel study. J Nurs Manag. 2020; 28(8):2157-65. [DOI:10.1111/jonm.12970] [PMID]
- Ball JE, Griffiths P, Rafferty AM, Lindqvist R, Murrells T, Tishelman C. A cross-sectional study of ‘care left undone’on nursing shifts in hospitals. J Adv Nurs. 2016; 72(9):2086-97. [DOI:10.1111/jan.12976] [PMID]
- Kim KJ, Yoo MS, Seo EJ. Exploring the influence of nursing work environment and patient safety culture on missed nursing care in Korea. Asian Nurs Res (Korean Soc Nurs Sci). 2018; S1976-1317(17)30683-7. [DOI:10.1016/j.anr.2018.04.003] [PMID]
- Zelenikova R, Jarosova D, Plevova I, Janikova E. Nurses’ perceptions of professional practice environment and its relation to missed nursing care and nurse satisfaction. Int J Environ Res Public Health. 2020; 17(11):3805. [DOI:10.3390/ijerph17113805] [PMID]
Article Type : Research |
Subject:
Special
Received: 2023/10/24 | Accepted: 2023/11/19 | Published: 2025/01/12
Received: 2023/10/24 | Accepted: 2023/11/19 | Published: 2025/01/12
Send email to the article author
| Rights and permissions | |
 | This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
