Mon, Jul 22, 2024
Volume 33, Issue 4 (9-2023)
JHNM 2023, 33(4): 259-267 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Farokhzadian J, Sohrabzadeh N, Jahani Y, Nouhi E. The Effect of Acceptance and Commitment Therapy on High-risk Behaviors of Delinquent Adolescents in a Juvenile Detention Center. JHNM 2023; 33 (4) :259-267
URL: http://hnmj.gums.ac.ir/article-1-2226-en.html
URL: http://hnmj.gums.ac.ir/article-1-2226-en.html



1- Associate Professor, Nursing Research Center, Kerman University of Medical Sciences, Kerman, Iran.
2- Nursing (MSN), Student Research Committee, Razi Faculty of Nursing and Midwifery, Kerman University of Medical Sciences, Kerman, Iran.
3- Associate Professor, Department of Biostatistics and Epidemiology, School of Public Health, Kerman University of Medical Sciences, Kerman, Iran.
4- Professor, Department of Medical Surgical Nursing, Razi Faculty of Nursing and Midwifery, Kerman University of Medical Sciences, Kerman, Iran. ,e-nuhi@kmu.ac.ir
2- Nursing (MSN), Student Research Committee, Razi Faculty of Nursing and Midwifery, Kerman University of Medical Sciences, Kerman, Iran.
3- Associate Professor, Department of Biostatistics and Epidemiology, School of Public Health, Kerman University of Medical Sciences, Kerman, Iran.
4- Professor, Department of Medical Surgical Nursing, Razi Faculty of Nursing and Midwifery, Kerman University of Medical Sciences, Kerman, Iran. ,
Full-Text [PDF 568 kb]
(273 Downloads)
| Abstract (HTML) (461 Views)
Full-Text: (168 Views)
Introduction
Adolescence is the most important and valuable stage of every person’s life. Adolescents are more exposed to high-risk behaviors due to physical, psychological, and social changes in transitioning from childhood to adulthood [1]. High-risk behaviors endanger individuals’ and society’s physical, psychological, social health and wellbeing [2]. Hookah smoking, cigarette smoking, sexual intercourse, beating outside the home, and experience of alcohol consumption were reported as the most common high-risk behaviors among Iranian adolescents, with the average high-risk behaviors being higher among boys than girls [3].
Keeping adolescents who have committed high-risk behaviors in juvenile detention centers is one of the interventions needed to promote the health of people in any community [4]. This objective requires adolescents’ control by the criminal justice system for a short time. They should receive education and support in these centers to distance themselves from the risk factors around them [5]. However, instead of prisons, these centers can be called delinquency prevention schools, where some measures are taken to socialize children.
One of the most effective treatments for adolescents introduced in recent years is acceptance and commitment therapy (ACT) [6]. In the ACT, the main goal is to create psychological flexibility to enable a person to make more practical choices among various available options. The therapy emphasizes that psychological distress in people is the product of trying to control or avoid negative thoughts and behaviors. Instead of changing cognitions, this treatment technique establishes a psychological connection between the person and their thoughts and feelings. In other words, in ACT, individuals are advised to accept what is beyond their control and to pay attention to actions, behaviors, and activities that lead to a better life without prejudice [6, 7].
A literature review shows that several studies examined the effect of ACT on different vulnerable groups. For instance, Takahashi et al. found that the school-based group ACT could reduce adolescent avoidance and hyperactivity-inattention, but ACT did not reduce symptoms in sub-clinical samples [8]. In other studies, ACT was effective in improving stress and psychotic symptoms, obsessive-compulsive disorder, anxiety, substance abuse in adolescent groups [9], psychological capital and school engagement in adolescents with anxiety [10], and the mental health of women imprisoned for substance abuse [11]. In a meta-analysis study, ACT was reported to have a positive effect on anxiety disorders, depression, addiction, and physical problems of vulnerable groups [12].
A juvenile detention center is one of the places for community-oriented nurses’ activities. However, community health nurses and social workers usually neglect the problems of delinquent adolescents in a juvenile detention center. They can render professional services to delinquent adolescents by assessing high-risk behaviors, designing educational and interventional programs such as ACT for changing attitudes and behavior, and ultimately promoting their mental health. However, limited studies have addressed ACT’s effectiveness on high-risk behaviors in male adolescents in juvenile detention centers in Iran. Therefore, this study aimed to investigate the effect of ACT on the risk-taking behaviors of delinquents in a juvenile detention center.
Materials and Methods
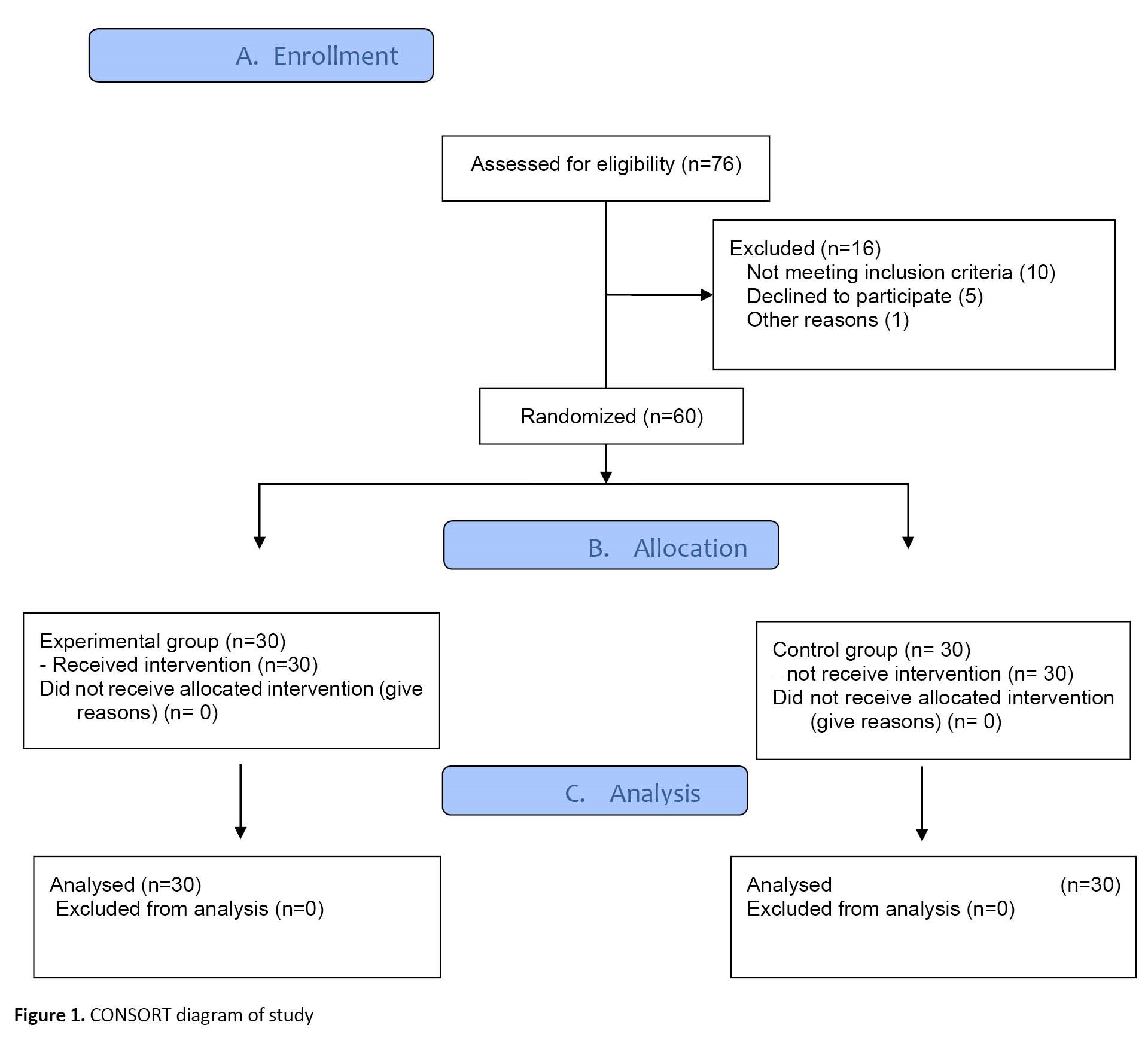
This quasi-experimental study used a pre-test and post-test design with control and intervention groups. The research setting was a juvenile detention center in Kerman City, Iran, the largest province in southeastern Iran. The center is one of the best places for correcting and educating delinquent adolescents. It also provides employment and support for its clients after release. The research population included all male delinquent adolescents (n=76) who were kept in the juvenile detention center during the data collection period from April to July 2020. Given the limited number of adolescents, all were recruited by the census method. According to the inclusion criteria, 60 adolescents were assigned to the intervention and control groups using simple random sampling (30 persons in each group). The inclusion criteria were receiving voluntary and informed consent from the participants and their legal guardians and having no self-reported mental or physical disorders. Besides, absence for more than 2 intervention sessions and participants’ unwillingness to continue attending the sessions were considered exclusion criteria. None of the samples were excluded until the end of the study (Figure 1).
Adolescence is the most important and valuable stage of every person’s life. Adolescents are more exposed to high-risk behaviors due to physical, psychological, and social changes in transitioning from childhood to adulthood [1]. High-risk behaviors endanger individuals’ and society’s physical, psychological, social health and wellbeing [2]. Hookah smoking, cigarette smoking, sexual intercourse, beating outside the home, and experience of alcohol consumption were reported as the most common high-risk behaviors among Iranian adolescents, with the average high-risk behaviors being higher among boys than girls [3].
Keeping adolescents who have committed high-risk behaviors in juvenile detention centers is one of the interventions needed to promote the health of people in any community [4]. This objective requires adolescents’ control by the criminal justice system for a short time. They should receive education and support in these centers to distance themselves from the risk factors around them [5]. However, instead of prisons, these centers can be called delinquency prevention schools, where some measures are taken to socialize children.
One of the most effective treatments for adolescents introduced in recent years is acceptance and commitment therapy (ACT) [6]. In the ACT, the main goal is to create psychological flexibility to enable a person to make more practical choices among various available options. The therapy emphasizes that psychological distress in people is the product of trying to control or avoid negative thoughts and behaviors. Instead of changing cognitions, this treatment technique establishes a psychological connection between the person and their thoughts and feelings. In other words, in ACT, individuals are advised to accept what is beyond their control and to pay attention to actions, behaviors, and activities that lead to a better life without prejudice [6, 7].
A literature review shows that several studies examined the effect of ACT on different vulnerable groups. For instance, Takahashi et al. found that the school-based group ACT could reduce adolescent avoidance and hyperactivity-inattention, but ACT did not reduce symptoms in sub-clinical samples [8]. In other studies, ACT was effective in improving stress and psychotic symptoms, obsessive-compulsive disorder, anxiety, substance abuse in adolescent groups [9], psychological capital and school engagement in adolescents with anxiety [10], and the mental health of women imprisoned for substance abuse [11]. In a meta-analysis study, ACT was reported to have a positive effect on anxiety disorders, depression, addiction, and physical problems of vulnerable groups [12].
A juvenile detention center is one of the places for community-oriented nurses’ activities. However, community health nurses and social workers usually neglect the problems of delinquent adolescents in a juvenile detention center. They can render professional services to delinquent adolescents by assessing high-risk behaviors, designing educational and interventional programs such as ACT for changing attitudes and behavior, and ultimately promoting their mental health. However, limited studies have addressed ACT’s effectiveness on high-risk behaviors in male adolescents in juvenile detention centers in Iran. Therefore, this study aimed to investigate the effect of ACT on the risk-taking behaviors of delinquents in a juvenile detention center.
Materials and Methods
This quasi-experimental study used a pre-test and post-test design with control and intervention groups. The research setting was a juvenile detention center in Kerman City, Iran, the largest province in southeastern Iran. The center is one of the best places for correcting and educating delinquent adolescents. It also provides employment and support for its clients after release. The research population included all male delinquent adolescents (n=76) who were kept in the juvenile detention center during the data collection period from April to July 2020. Given the limited number of adolescents, all were recruited by the census method. According to the inclusion criteria, 60 adolescents were assigned to the intervention and control groups using simple random sampling (30 persons in each group). The inclusion criteria were receiving voluntary and informed consent from the participants and their legal guardians and having no self-reported mental or physical disorders. Besides, absence for more than 2 intervention sessions and participants’ unwillingness to continue attending the sessions were considered exclusion criteria. None of the samples were excluded until the end of the study (Figure 1).
The study data were collected using a demographic information form that assessed the participants’ characteristics such as age, education, parental education, occupation, and monthly family income. The other tool was the Iranian adolescent risk scale (iARS), developed by Zadeh Mohammadi et al. [13] in Iran. The scale contains 38 items to assess the harms of adolescents in high-risk behaviors using 7 tendencies to these items: substance abuse (items 1 to 8), alcoholism (items 9 to 14), smoking tendency (items 15 to 19), violence (items 20), sexual behavior (items 25 to 28), communicate with the opposite sex (items 29 to 32), and careless driving (items 33 to 38). Respondents are asked to express their agreement or disagreement with these items on a 5-point scale ranging from 5 (strongly agree) to 1 (strongly disagree).
The content of the ACT intervention was prepared based on the research of Hayes et al. [14]. To implement the ACT, a brief description of the intervention sessions, the schedule of the ACT, and the research objectives were provided to the participants and the officials of the center by the first researcher. A clinical psychologist professional in ACT, who was not a research team member, conducted the ACT intervention package in eight 90-minute sessions for 2 months (4 face-to-face and 4 offline sessions). All sessions were held at a hall located within a juvenile detention center with sufficient training facilities. Online sessions were held through the presentation of recorded videos in the form of lectures, questions and answers, and PowerPoint slides in a hall. Participants were also encouraged to do practical exercises. Researchers closely monitored the study conditions to ensure the program was implemented according to the schedule and the participants completed assigned exercises. A detailed description of ACT sessions is shown in Table 1.

During the intervention program, the control group members did not undergo any intervention and only received the routine training provided by the juvenile detention center. One month after the intervention, the participants in the two groups completed the two questionnaires. Upon the data collection, an educational package containing all training materials was provided to the control group members. Therefore, the treatment was not shared between the intervention and control groups. Moreover, the researchers reminded the intervention group not to discuss the training contents with the control group until the end of the study.
Data were collected using an anonymous, self-reported, and structured questionnaire. The second researcher referred to the study setting, distributed the questionnaires among participants of the intervention and control groups in the pre-test (before ACT) and post-test stages (1 month after the ACT), and trained participants on how to fill out the questionnaires.
The data were entered into the SPSS software, version 21 and analyzed using descriptive (frequency, percentage, Mean±SD) and inferential statistics (independent samples t-test, paired samples t-test, chi-square test, and the analysis of covariance [ANCOVA]). The Kolmogorov-Smirnov test showed that the data followed a normal distribution. The significance level was considered at <0.05.
Results
In this study, all 60 male adolescents in the intervention group (n=30) and the control group (n=30) completed the study (100% response rate). Most adolescents in the intervention and control groups were in the age group of 16-20 years (96.7% and 93.3%, respectively), had a middle school degree (56.7% and 40%, respectively), and their fathers were illiterate or passed primary school (43% and 40% respectively). Their mothers in the intervention and control groups had a high school diploma (40% and 50%, respectively), their fathers were self-employed (80% and 76.7%, respectively), their mothers were housewives (76.7% and 86.7%, respectively), and their family income was $60 to $100 per month (73.3% and 86.7%, respectively). Besides, most of the participants in the intervention group were alive (63%), and most of the participants in the control group were divorced (53%). Moreover, the participants in both intervention and control groups had no significant differences in terms of all variables except the parents’ marital status (Table 2).

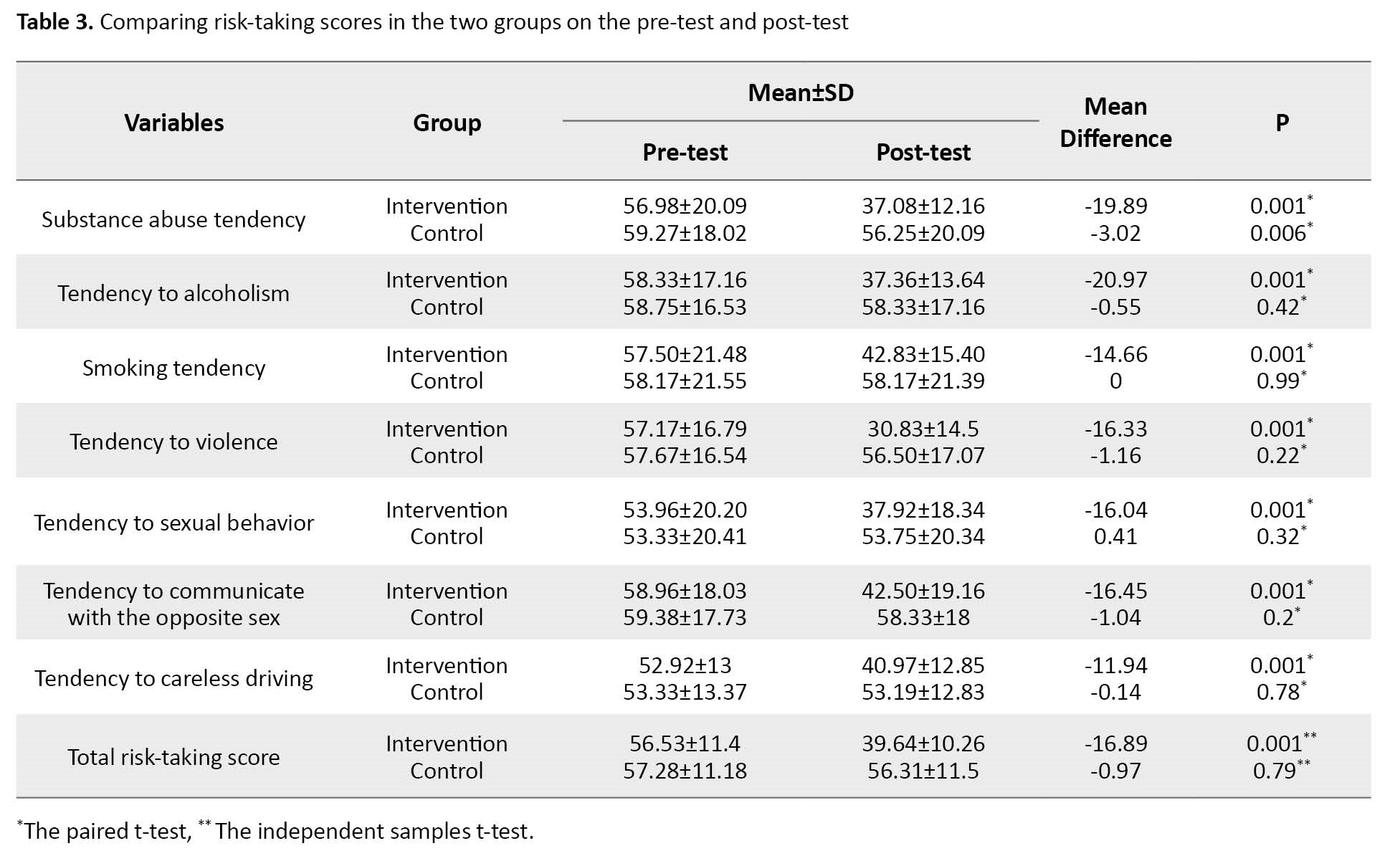
Results showed that the score of risk-taking for the participants in the intervention group in the post-test stage (39.64±10.26) significantly (P=0.001) decreased compared with the pre-test stage (56.53±11.4). Moreover, the post-test score of risk-taking for the control group (56.31±11.5) was significantly (P=0.005) lower than the pre-test score (57.28±11.18), with a mean difference of 0.97 (Table 3).
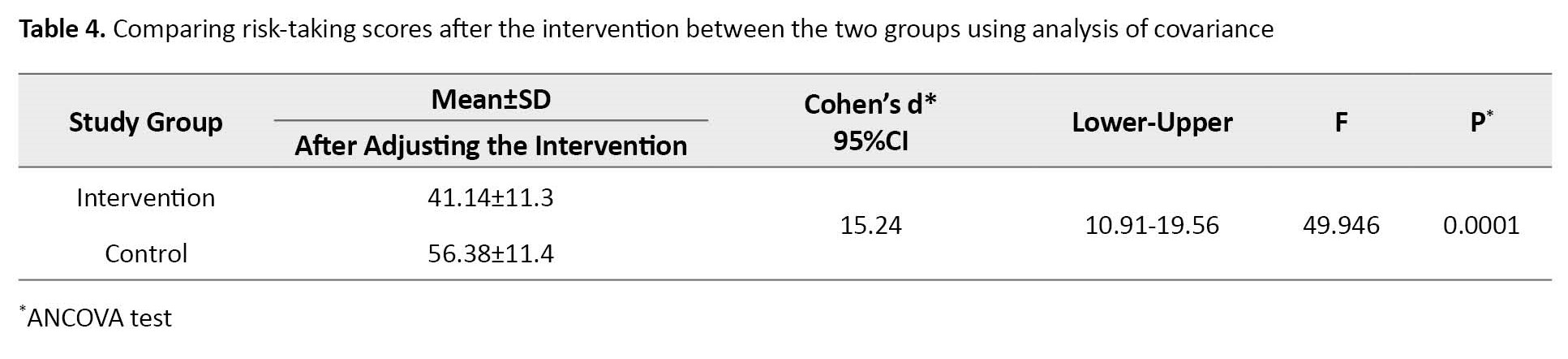
Using the analysis of covariance and controlling the demographic variables, after the intervention, the Mean±SD risk-taking parents’ marital status for the participants in the intervention group was higher than the control (56.38±11.4 vs 41.14±11.3), and these differences were statistically significant (Cohen’s d=15.24; 95% CI, 10.91%-19.56%). The information is presented in Table 4.
Discussion
The present study evaluated the effect of ACT on the high-risk behaviors of delinquent adolescents in a juvenile detention center. The findings indicated that the ACT decreased self-reported risk-taking of the intervention group significantly on the post-test. Accordingly, several studies have examined the effectiveness of ACT on high-risk behaviors. These studies showed that the high-risk behaviors in the intervention group reduced significantly compared to the control group after the ACT [7, 15, 16, 17, 18, 19]. Saiedmanesh and Pahlavan reported that the score of self-control and self-regulation of the adolescents with drug abuse disorder in the intervention group increased compared to the pre-test after ACT [7]. Spidel found that symptom severity and anxiety in individuals with psychosis and those with a history of childhood trauma decreased over the treatment, and participants’ ability to regulate their emotional reactions increased. The study also found that treatment engagement increased regarding help-seeking for those in the ACT group, compared with the control group [20]. Moreover, a meta-analysis review evaluated the effectiveness of internet-based ACT on mental health outcomes in individuals with different psychological and somatic conditions/complaints. The measured results indicated greater efficacy in improving some mental health outcomes, such as depression and psychological flexibility outcomes, compared to non-guided ACT [6].
Perhaps the similarity between the findings of this study and those studies can be attributed to the research sample, the implementation of the ACT by a competent psychologist, and the use of a similar intervention protocol. It should be acknowledged that attention to educational techniques plays an essential role in shaping adolescent behavior. Therefore, it is recommended to incorporate ACT by experienced psychologists in different adolescent training programs to prevent high-risk behaviors.
However, a study that assessed the efficacy of an abbreviated, classroom-based, teacher-taught ACT program to improve mental health in adolescents showed no significant improvements in any outcome measure compared with the control group. Researchers suggested that their ACT was delivered by teachers instead of mental health professionals, so professionally trained therapists may be needed for ACT to be efficacious [21].
The results of this study showed that at the post-test stage, the score of high-risk behaviors decreased significantly in the control group compared with the pre-test. Still, this decrease was lower than in the intervention group. This change may be due to the corrective and educational measures routinely performed in juvenile detention centers. Furthermore, the participants’ behavior in the intervention group after ACT could slightly affect the control group members. These issues were beyond the researchers’ control in this study. However, studies showed that the score of high-risk behaviors in the control group after the ACT did not change significantly compared to their scores before the ACT [6, 22]. These conflicting findings can be attributed to cultural factors, the conditions governing data collection tools, the research setting, and time.
One of the limitations of this study was the difference in the adolescents’ personal, psychological, and family characteristics that could affect their responses to the questions. Thus, the researchers tried to minimize these differences by randomly assigning the participants to the intervention and control groups. Moreover, due to the complexity of the ACT intervention sessions, the exchange of information between the participants in the intervention and control groups must have been minimal. However, some information might have been slightly shared between the two groups, beyond the researchers’ control.
This study showed that the ACT intervention significantly decreased the high-risk behaviors of delinquent adolescents in the detention center. Since adolescents in the detention center are going through a critical period of their lives, ACT can effectively reduce the incidence of high-risk behaviors in them. Therefore, ACT can be implemented with other routine training programs in detention centers. Policymakers, social workers, and community health nurses are recommended to design psychological interventions such as ACT to significantly impact the lives of adolescents, especially adolescents with high-risk behaviors. Moreover, they should investigate the effectiveness of these interventions in reducing delinquent adolescents’ high-risk behaviors.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of Kerman University of Medical Sciences (Code: IR.KMU.REC.1398.434). All methods were carried out in accordance with relevant guidelines and regulations. Written informed consent was obtained from the adolescents and their legal guardians. The participants were assured of the confidentiality of their information and voluntary participation. They could withdraw from the study at all stages without any negative consequences, and the results would be provided to them if they were willing. After completing the research project, the training package was also given to the control group members.
Funding
This research project received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Authors' contributions
Conceptualization and study design: Esmat Nouhi, Jamileh Farokhzadian, and Nargess Sohrabzade; Data collection: Nargess Sohrabzadeh; Data analysis and data interpretation Yunes Jahani; drafting the manuscript and final approval: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors would like to thank those who contributed to conducting this study and spent their time generously participating. We also acknowledge the directors and trainers of the detention center, the prison administration, the adolescents, and the security guards who assisted the research team in organizing and holding the training sessions.
References
The content of the ACT intervention was prepared based on the research of Hayes et al. [14]. To implement the ACT, a brief description of the intervention sessions, the schedule of the ACT, and the research objectives were provided to the participants and the officials of the center by the first researcher. A clinical psychologist professional in ACT, who was not a research team member, conducted the ACT intervention package in eight 90-minute sessions for 2 months (4 face-to-face and 4 offline sessions). All sessions were held at a hall located within a juvenile detention center with sufficient training facilities. Online sessions were held through the presentation of recorded videos in the form of lectures, questions and answers, and PowerPoint slides in a hall. Participants were also encouraged to do practical exercises. Researchers closely monitored the study conditions to ensure the program was implemented according to the schedule and the participants completed assigned exercises. A detailed description of ACT sessions is shown in Table 1.
During the intervention program, the control group members did not undergo any intervention and only received the routine training provided by the juvenile detention center. One month after the intervention, the participants in the two groups completed the two questionnaires. Upon the data collection, an educational package containing all training materials was provided to the control group members. Therefore, the treatment was not shared between the intervention and control groups. Moreover, the researchers reminded the intervention group not to discuss the training contents with the control group until the end of the study.
Data were collected using an anonymous, self-reported, and structured questionnaire. The second researcher referred to the study setting, distributed the questionnaires among participants of the intervention and control groups in the pre-test (before ACT) and post-test stages (1 month after the ACT), and trained participants on how to fill out the questionnaires.
The data were entered into the SPSS software, version 21 and analyzed using descriptive (frequency, percentage, Mean±SD) and inferential statistics (independent samples t-test, paired samples t-test, chi-square test, and the analysis of covariance [ANCOVA]). The Kolmogorov-Smirnov test showed that the data followed a normal distribution. The significance level was considered at <0.05.
Results
In this study, all 60 male adolescents in the intervention group (n=30) and the control group (n=30) completed the study (100% response rate). Most adolescents in the intervention and control groups were in the age group of 16-20 years (96.7% and 93.3%, respectively), had a middle school degree (56.7% and 40%, respectively), and their fathers were illiterate or passed primary school (43% and 40% respectively). Their mothers in the intervention and control groups had a high school diploma (40% and 50%, respectively), their fathers were self-employed (80% and 76.7%, respectively), their mothers were housewives (76.7% and 86.7%, respectively), and their family income was $60 to $100 per month (73.3% and 86.7%, respectively). Besides, most of the participants in the intervention group were alive (63%), and most of the participants in the control group were divorced (53%). Moreover, the participants in both intervention and control groups had no significant differences in terms of all variables except the parents’ marital status (Table 2).
Results showed that the score of risk-taking for the participants in the intervention group in the post-test stage (39.64±10.26) significantly (P=0.001) decreased compared with the pre-test stage (56.53±11.4). Moreover, the post-test score of risk-taking for the control group (56.31±11.5) was significantly (P=0.005) lower than the pre-test score (57.28±11.18), with a mean difference of 0.97 (Table 3).
Using the analysis of covariance and controlling the demographic variables, after the intervention, the Mean±SD risk-taking parents’ marital status for the participants in the intervention group was higher than the control (56.38±11.4 vs 41.14±11.3), and these differences were statistically significant (Cohen’s d=15.24; 95% CI, 10.91%-19.56%). The information is presented in Table 4.
Discussion
The present study evaluated the effect of ACT on the high-risk behaviors of delinquent adolescents in a juvenile detention center. The findings indicated that the ACT decreased self-reported risk-taking of the intervention group significantly on the post-test. Accordingly, several studies have examined the effectiveness of ACT on high-risk behaviors. These studies showed that the high-risk behaviors in the intervention group reduced significantly compared to the control group after the ACT [7, 15, 16, 17, 18, 19]. Saiedmanesh and Pahlavan reported that the score of self-control and self-regulation of the adolescents with drug abuse disorder in the intervention group increased compared to the pre-test after ACT [7]. Spidel found that symptom severity and anxiety in individuals with psychosis and those with a history of childhood trauma decreased over the treatment, and participants’ ability to regulate their emotional reactions increased. The study also found that treatment engagement increased regarding help-seeking for those in the ACT group, compared with the control group [20]. Moreover, a meta-analysis review evaluated the effectiveness of internet-based ACT on mental health outcomes in individuals with different psychological and somatic conditions/complaints. The measured results indicated greater efficacy in improving some mental health outcomes, such as depression and psychological flexibility outcomes, compared to non-guided ACT [6].
Perhaps the similarity between the findings of this study and those studies can be attributed to the research sample, the implementation of the ACT by a competent psychologist, and the use of a similar intervention protocol. It should be acknowledged that attention to educational techniques plays an essential role in shaping adolescent behavior. Therefore, it is recommended to incorporate ACT by experienced psychologists in different adolescent training programs to prevent high-risk behaviors.
However, a study that assessed the efficacy of an abbreviated, classroom-based, teacher-taught ACT program to improve mental health in adolescents showed no significant improvements in any outcome measure compared with the control group. Researchers suggested that their ACT was delivered by teachers instead of mental health professionals, so professionally trained therapists may be needed for ACT to be efficacious [21].
The results of this study showed that at the post-test stage, the score of high-risk behaviors decreased significantly in the control group compared with the pre-test. Still, this decrease was lower than in the intervention group. This change may be due to the corrective and educational measures routinely performed in juvenile detention centers. Furthermore, the participants’ behavior in the intervention group after ACT could slightly affect the control group members. These issues were beyond the researchers’ control in this study. However, studies showed that the score of high-risk behaviors in the control group after the ACT did not change significantly compared to their scores before the ACT [6, 22]. These conflicting findings can be attributed to cultural factors, the conditions governing data collection tools, the research setting, and time.
One of the limitations of this study was the difference in the adolescents’ personal, psychological, and family characteristics that could affect their responses to the questions. Thus, the researchers tried to minimize these differences by randomly assigning the participants to the intervention and control groups. Moreover, due to the complexity of the ACT intervention sessions, the exchange of information between the participants in the intervention and control groups must have been minimal. However, some information might have been slightly shared between the two groups, beyond the researchers’ control.
This study showed that the ACT intervention significantly decreased the high-risk behaviors of delinquent adolescents in the detention center. Since adolescents in the detention center are going through a critical period of their lives, ACT can effectively reduce the incidence of high-risk behaviors in them. Therefore, ACT can be implemented with other routine training programs in detention centers. Policymakers, social workers, and community health nurses are recommended to design psychological interventions such as ACT to significantly impact the lives of adolescents, especially adolescents with high-risk behaviors. Moreover, they should investigate the effectiveness of these interventions in reducing delinquent adolescents’ high-risk behaviors.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of Kerman University of Medical Sciences (Code: IR.KMU.REC.1398.434). All methods were carried out in accordance with relevant guidelines and regulations. Written informed consent was obtained from the adolescents and their legal guardians. The participants were assured of the confidentiality of their information and voluntary participation. They could withdraw from the study at all stages without any negative consequences, and the results would be provided to them if they were willing. After completing the research project, the training package was also given to the control group members.
Funding
This research project received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Authors' contributions
Conceptualization and study design: Esmat Nouhi, Jamileh Farokhzadian, and Nargess Sohrabzade; Data collection: Nargess Sohrabzadeh; Data analysis and data interpretation Yunes Jahani; drafting the manuscript and final approval: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors would like to thank those who contributed to conducting this study and spent their time generously participating. We also acknowledge the directors and trainers of the detention center, the prison administration, the adolescents, and the security guards who assisted the research team in organizing and holding the training sessions.
References
- Barghandan S, Akbari B, Khalatbari J, Varaste A. [Comparison of the effectiveness of acceptance and commitment therapy and compassion focused therapy on quality of life among female adolescents with high-risk behaviors (Persian)]. J Ilam Univ Med Sci. 2018, 26(3):158-68. [DOI:10.29252/sjimu.26.3.158]
- Boyer CB, Greenberg L, Chutuape K, Walker B, Monte D, Kirk J, et al. Exchange of sex for drugs or money in adolescents and young adults: an examination of sociodemographic factors, HIV-related risk, and community context.J Community Health. 2017; 42(1):90-100. [DOI:10.1007/s10900-016-0234-2] [PMID]
- Rashid KH. [High-risk behaviors among adolescent male and female students in Tehran (Persian)]. Soc Welfare. 2015, 15(57):31-56. [Link]
- Ghazanfari H, Miri S, Taebi M, Farokhzadian J. Psychological wellbeing, family cohesion, and purposeful life in male prisoners: A cross-sectional study. Front Psychiatry. 2023; 13:1054149. [DOI:10.3389/fpsyt.2022.1054149] [PMID]
- Edelson M. Special education in adult correctional facilities. A right not a privilege. Loy LAL REv. 2017; 50:93. [Link]
- Thompson EM, Destree L, Albertella L, Fontenelle LF. Internet-based acceptance and commitment therapy: A transdiagnostic systematic review and meta-analysis for mental health outcomes. Behav Ther. 2021; 52(2):492-507. [DOI:10.1016/j.beth.2020.07.002] [PMID]
- Saiedmanesh M, Pahlavan M. [Evaluation of the effectiveness of Acceptance and Commitment Therapy (ACT) on self-regulation and self-control of the adolescents with drug abuse disorder (Persian)]. Soc work. 2018; 6(4):14-22. [Link]
- Takahashi F, Ishizu K, Matsubara K, Ohtsuki T, Shimoda Y. Acceptance and commitment therapy as a school-based group intervention for adolescents: An open-label trial. J Contextual Behav Sci. 2020; 16:71-9. [DOI:10.1016/j.jcbs.2020.03.001]
- Gómez MJ, Luciano C, Páez-Blarrina M, Ruiz FJ, Valdivia-Salas S, Gil-Luciano B. Brief ACT protocol in at-risk adolescents with conduct disorder and impulsivity. Int J Psychol Psychol Ther. 2014; 14(3):307-32. [Link]
- Petersen JM, Davis CH, Renshaw TL, Levin ME, Twohig MP. School-based acceptance and commitment therapy for adolescents with anxiety: A pilot trial. Cogn Behav Pract. 2023; 30(3):436-52. [DOI:10.1016/j.cbpra.2022.02.021]
- Lanza PV, García PF, Lamelas FR, González-Menéndez A. Acceptance and commitment therapy versus cognitive behavioral therapy in the treatment of substance use disorder with incarcerated women. J Clin Psychol. 2014; 70(7):644-57. [DOI:10.1002/jclp.22060] [PMID]
- A-Tjak JG, Davis ML, Morina N, Powers MB, Smits JA, Emmelkamp PM. A meta-analysis of the efficacy of acceptance and commitment therapy for clinically relevant mental and physical health problems. Psychother Psychosom. 2015; 84(1):30-6. [DOI:10.1159/000365764] [PMID]
- Zadeh Mohammadi A, Ahmadabadi Z, Heidari M. [Construction and assessment of psychometric features of Iranian adolescents risk-taking scale (Persian)]. Iran J Psychiatry Clin Psychol. 2011; 17(3):218-25. [Link]
- Hayes L, Boyd CP, Sewell J. Acceptance and commitment therapy for the treatment of adolescent depression: A pilot study in a psychiatric outpatient setting. Mindfulness 2011, 2:86-94. [DOI:10.1007/s12671-011-0046-5]
- Heffner M, Eifert GH, Parker BT, Hernandez DH, Sperry JA. Valued directions: Acceptance and commitment therapy in the treatment of alcohol dependence. Cogn Behav Pract. 2013; 10(4):378-83. [DOI:10.1016/S1077-7229(03)80055-X]
- Courtemanche C, Marton J, Ukert B, Yelowitz A, Zapata D. Early effects of the Affordable Care Act on health care access, risky health behaviors, and self-assessed health. South Econ J. 2018; 84(3):660-91. [DOI:10.1002/soej.12245]
- Byrne SP, Haber P, Baillie A, Costa DS, Fogliati V, Morley K. Systematic reviews of mindfulness and acceptance and commitment therapy for alcohol use disorder: should we be using third wave therapies? Alcohol Alcohol. 2019; 54(2):159-66. [DOI:10.1093/alcalc/agy089] [PMID]
- Bricker JB, Mull KE, Kientz JA, Vilardaga R, Mercer LD, Akioka KJ, et al. Randomized, controlled pilot trial of a smartphone app for smoking cessation using acceptance and commitment therapy. Drug Alcohol Depend. 2014; 143:87-94. [DOI:10.1016/j.drugalcdep.2014.07.006] [PMID]
- Heffner M, Eifert GH, Parker BT, Hernandez DH, Sperry JA. Valued directions: Acceptance and commitment therapy in the treatment of alcohol dependence. Cogn Behav Pract. 2003; 10(4):378-83. [DOI:10.1016/S1077-7229(03)80055-X]
- Spidel A, Lecomte T, Kealy D, Daigneault I. Acceptance and commitment therapy for psychosis and trauma: Improvement in psychiatric symptoms, emotion regulation, and treatment compliance following a brief group intervention. Psychol Psychother. 2018; 91(2):248-61. [DOI:10.1111/papt.12159] [PMID]
- Van der Gucht K, Griffith JW, Hellemans R, Bockstaele M, Pascal-Claes F, Raes F. Acceptance and commitment therapy (ACT) for adolescents: Outcomes of a large-sample, school-based, cluster-randomized controlled trial. Mindfulness. 2017; 8:408-16. [DOI:10.1007/s12671-016-0612-y]
- Mofid V, Fatehizadeh M, Dorosti F. [Effectiveness of acceptance and commitment therapy on depression and quality of life of women criminal prisoners in Isfahan city (Persian)]. Strateg Res Soc Probl Iran. 2017; 6(3):17-30. [DOI:10.22108/SSOSS.2017.85488.0]
Article Type : Research |
Subject:
General
Received: 2023/09/18 | Accepted: 2023/09/3 | Published: 2023/09/3
Received: 2023/09/18 | Accepted: 2023/09/3 | Published: 2023/09/3
Send email to the article author
| Rights and permissions | |
 | This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
