Mon, Dec 29, 2025
Volume 35, Issue 3 (6-2025)
JHNM 2025, 35(3): 217-227 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Fathnezhad-Kazemi A, ranjbar M, Khalili F. Factors Impacting Anxiety Levels During Gynecological Examinations: The Role of Self-esteem, Coping Strategies. JHNM 2025; 35 (3) :217-227
URL: http://hnmj.gums.ac.ir/article-1-2224-en.html
URL: http://hnmj.gums.ac.ir/article-1-2224-en.html



1- Associate Professor, Department of Midwifery, TaMS.C., Islamic Azad University, Tabriz, Iran. , afnkazemi@gmail.com
2- Instructor, Department of Midwifery, TaMS.C., Islamic Azad University, Tabriz, Iran.
3- Medical Physician (MD), Department of Midwifery, TaMS.C., Islamic Azad University, Tabriz, Iran.
2- Instructor, Department of Midwifery, TaMS.C., Islamic Azad University, Tabriz, Iran.
3- Medical Physician (MD), Department of Midwifery, TaMS.C., Islamic Azad University, Tabriz, Iran.
Full-Text [PDF 507 kb]
(252 Downloads)
| Abstract (HTML) (628 Views)
Full-Text: (245 Views)
Introduction
Performing regular gynecological exams for the prognosis of venereal infections, vaginal cancers, and adverse conditions is very important for looking after women’s health [1, 2]. Also, gynecological examinations, including the bimanual and speculum exams, are common for periodic control of women [3]. Annual pelvic examinations, especially for cervical cancer screening, have been emphasized by the American Cancer Society (ACS) and the US Preventive Services Task Force (USPSTF) [4].
Most women experience undesirable feelings such as embarrassment and loss of control during sexual organ examinations, and they believe that sexual organs are a private part of their body and must be covered and concealed [5, 6]. Therefore, pelvic examinations might cause reactions such as mild to severe anxiety and embarrassment, which may result in the avoidance of the examinations and referral to physicians for health care services [5, 7]. Hereditary characteristics, gender, personality, emotional state, intelligence, social role and position, creativity, and social interaction contribute to the formation and variation of anxiety in people [8].
Self-esteem is one of the major aspects of adaptation in all life stages, contributing to emotional, social, and psychological adaptation. Low self-esteem can intensify anxiety [9, 10]. High self-esteem in an individual would result in self-confidence, enabling the individual to adapt to difficult conditions [10-12]. A study on girls showed a negative relationship between self-esteem and anxiety [13].
In addition, the most important factors affecting mental health include the manner of coping with stressful situations and life challenges. Some individuals lose their capability to cope with problems and challenging conditions very soon and experience anxiety [14]. Coping and adaptation to anxiety and stress are very important in women undergoing pelvic examinations [15, 16]. In a study on adolescents undergoing pelvic examination for the first time, results indicate a reverse relationship between the anxiety level and the self-confidence approach and optimistic coping strategy. Also, there is a direct relationship between anxiety, obedience, and a hopeless approach [8].
Due to various reasons such as religious and cultural differences, it is highly important to investigate the level of anxiety, self-esteem, and strategies of coping with and adaptation to stressful situations that may be created [3]. So, we conducted a study to investigate the role of self-esteem and coping strategies in pelvic examination-induced anxiety.
Materials and Methods
This cross-sectional study was conducted on 270 women attending obstetrics and gynecology clinics in one of the teaching and treatment centers in Tabriz City, Iran, during the first 6 months of 2022. They were selected using a convenience sampling method. The inclusion criteria were as follows: Women aged 18 and above, ability to read and write in Persian, absence of taking antidepressants, absence of chronic disease such as diabetes, having a genital examination during the visit, and willingness to participate in the study. The exclusion criterion was failure to complete the questionnaire.
The sample size was estimated at 243 cases based on the prevalence of anxiety reported by Yilmaz and Demirel’s study in Turkey; P=28.9% [17]. However, considering an increase in the study’s accuracy by 10%, the final sample size was calculated as 270 cases. Other parameters used were α=0.05, power=0.80, and d=20%.
The following four questionnaires were used to collect the data. The sociodemographic and obstetrics characteristics checklist consists of the sociodemographic variables of age, educational level, occupational status of women, self-assessment of household economic status, as well as obstetrics characteristics, including the number of pregnancies, the reason for the application to the gynecology clinic, duration of gynecological examination, and experienced emotion during gynecological examination.
The Rosenberg Self-esteem Scale (RSES) was developed by Rosenberg [18]. The scale consists of 10 items, five positive and five negative statements, and 12 categories to measure self-esteem. RSES is scored on a 4-point scale with response options ranging from 1=not at all true of me to 4=very true of me. Five items are inversely scored. Items 1, 2, 4, 6, and 7 investigate one’s positive self-evaluation and are scored from 3 to 0. Items 3, 5, 8, 9, and 10 investigate one’s negative self-evaluation and are scored from 0 to 3. Satisfactory self-esteem is defined as higher than or equal to 30 on the Rosenberg scale [19]. Joshanloo and Ghaedi assessed the validity and reliability of this scale in Iran [20].
Lazarus and Folkman compiled the Coping Strategies Inventory (CSI) in 1985 [21]. It comprises 66 items divided into 8 subscales: Confrontation, distancing, self-control, social support, accepting responsibility, escape-avoidance, problem-solving, and positive reappraisal. The respondents must indicate what they did in a given situation according to the classification, ranging from 0- a strategy not used; 1- used somewhat; 2- used quite a bit; to 3- used a great deal [22, 23]. This tool was used in many Iranian studies [24, 25].
Zung et al. designed the Situational Anxiety Scores (SAS) [26]. This scale included 20 questions about psychotic emotional symptoms, psychomotor disturbance, somatic disorder, and mental disorders of anxiety or depression. To answer each question, volunteers select the option that best describes their mental state. Each question is scored on a Likert-type scale of 1 to 4 or reverse scoring (“a little of the time”, “some of the time,” “a good part of the time”, and “most of the time”). On this scale, the maximum score is 80. The raw total scores were obtained by summarizing the total scores of the 20 questions and were converted to percentile standard scores. A final score of more than 50 was considered an anxiety symptom. Scores of 50–59, 60–69, and 70 or more are classified as mild, moderate, and severe anxiety, respectively [27]. In Iran, this tool was used in a study [28].
The reliability of questionnaires was assessed using the Cronbach α method in 20 women who had a pelvic examination. Thus, the reliability of self-esteem, coping strategies, and anxiety tools were found to be 0.82, 0.74, and 0.89, respectively.
The sampling was performed by acquiring the ethics permit from the Islamic Azad University of Tabriz Medical Sciences Ethics Committee and obtaining permission from the hospital authorities. All participants completed the questionnaires using the self-report method. Before recruiting the participants, they were informed about the study’s aims and their voluntary participation. If participants had problems understanding the questionnaire items while completing it, the author would answer them immediately.
The quantitative data were analyzed using SPSS software, version 24. First, frequency, percentage, and Mean±SD were determined using descriptive statistics. The normal distribution of the data was evaluated using the Kolmogorov-Smirnov test, skewness, and kurtosis. The Pearson correlation, Analysis of Variance (ANOVA), and t-test were used to determine the relationship between demographic and obstetric variables with the main research variables. Bivariate logistic regression with the “enter” method was used to investigate predictors of anxiety. The two-dimensional variable of anxiety (below 50 and above 50 scores) and the independent variables of coping strategies, self-esteem, and demographic variables with a significant level were entered into the model. The level of significance in this study was set at P<0.05.
Results
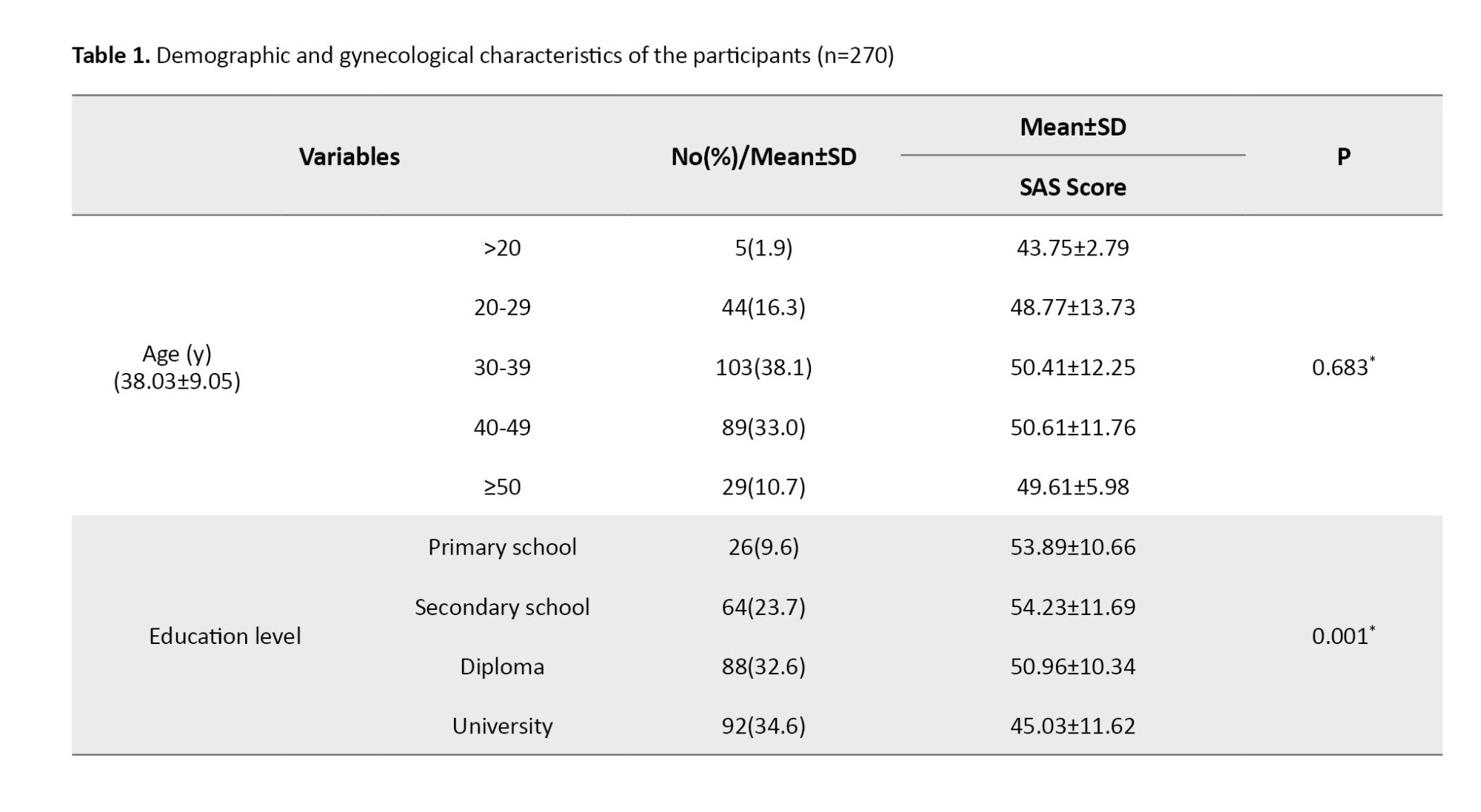
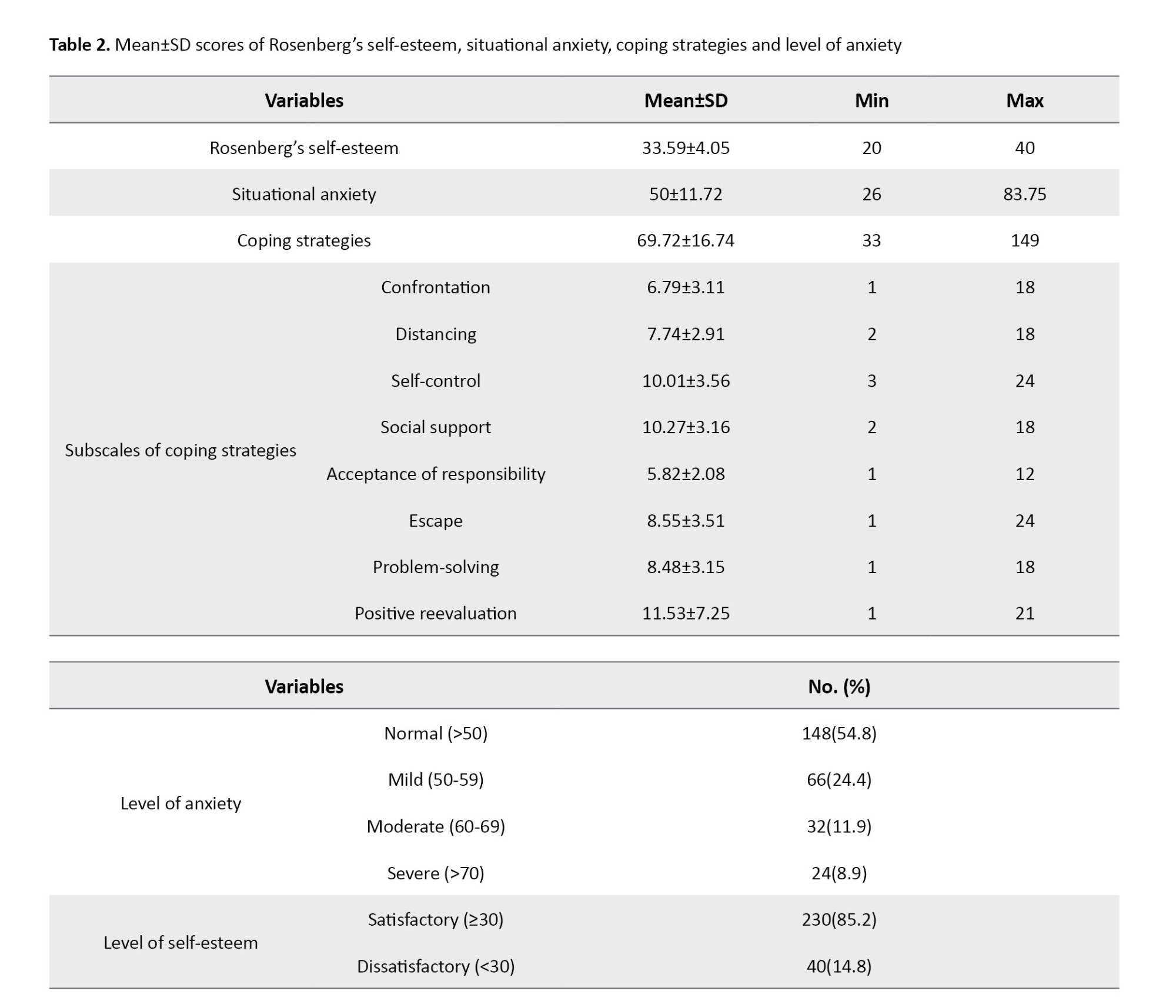
A total of 270 women who underwent gynecological examination participated in the study. In the present study, the Mean±SD age of the women was 38.03±9.05 years (range: 18-61 years). Most participants (67.2%) had high educational levels (high school diplomas and academic degrees). Nearly 79% of them had no job. Among the participants, 236(87.4%) were married and 34(12.6%) were divorced. Most of these women were multiparous, and only 23.3% were experiencing their first gynecological examination. The major cause of referral was bleeding and related problems. Also, the problem’s duration was specified until referral and examination duration. Nearly 85% of them reported a sense of embarrassment during the gynecological examination. Feelings such as stress, pain, and fear were reported in 66%, 62%, and 36% of the cases, respectively.
The examination of anxiety in different age groups showed that anxiety in the age group of 30-40 years was higher than in other groups; however, no statistical difference was observed between different age groups. The results indicate that the difference between the SAS in terms of educational level, job status, and income level was statistically significant. Hence, women with academic degrees experienced lower anxiety than other educational groups (P=0.001). These results were shown in Table 1.
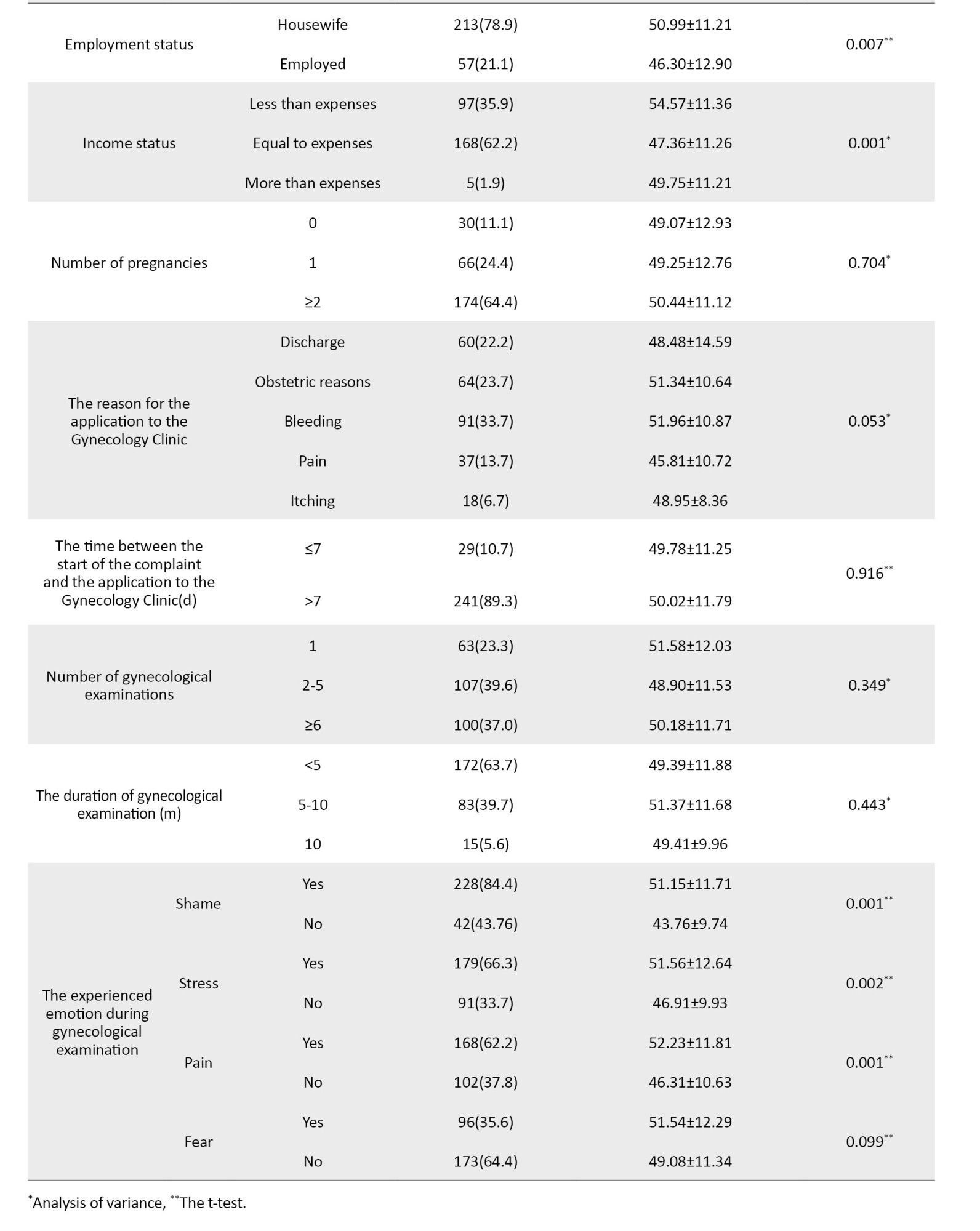
The Mean±SD of the SAS score of the participant women was 50±11.72 (range: 26-83.75). Based on the obtained results, 45.2% of the women experienced different levels of anxiety, including mild, medium, and severe levels. Their Mean±SD self-esteem score was equal to 33.59±4.05. So, based on the classification, almost 82% of the women had a satisfactory level of self-esteem. The coping strategies investigation showed that the Mean±SD total score on this scale was 69.72±16.74 (Table 2).
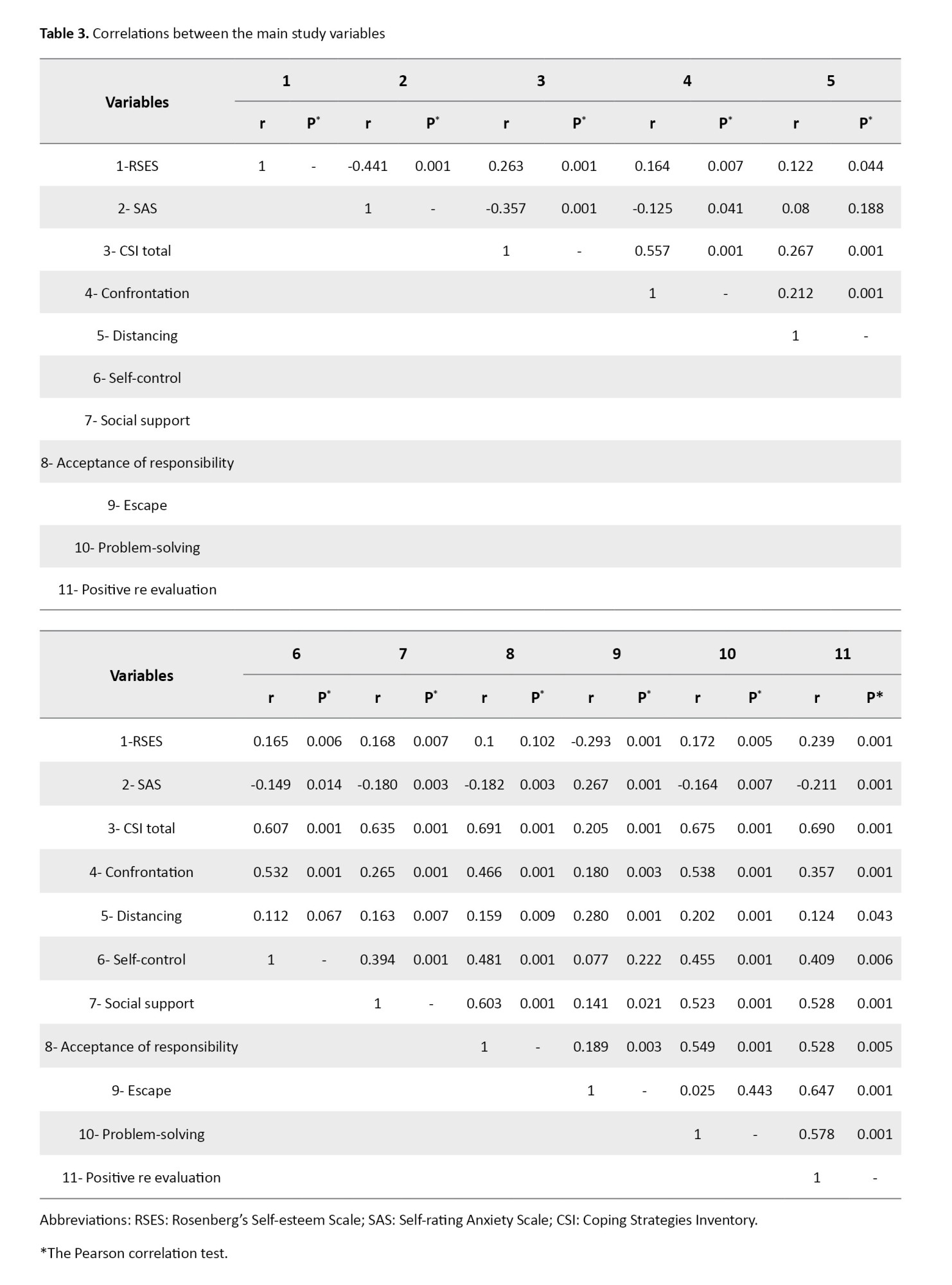
Based on the Pearson correlation coefficient results, there were significant reverse correlations between self-esteem (r=-0.441, P=0.001) and coping strategies (r=-0.357, P=0.001) with SAS. All subscales of coping strategies, except distancing and avoidance, had a reverse correlation with anxiety. Although the distancing subscale had a positive relationship with anxiety, this relationship was not significant. However, the avoidance subscale showed a significant positive relationship (r=0.267, P=0.001) with anxiety (Table 3).
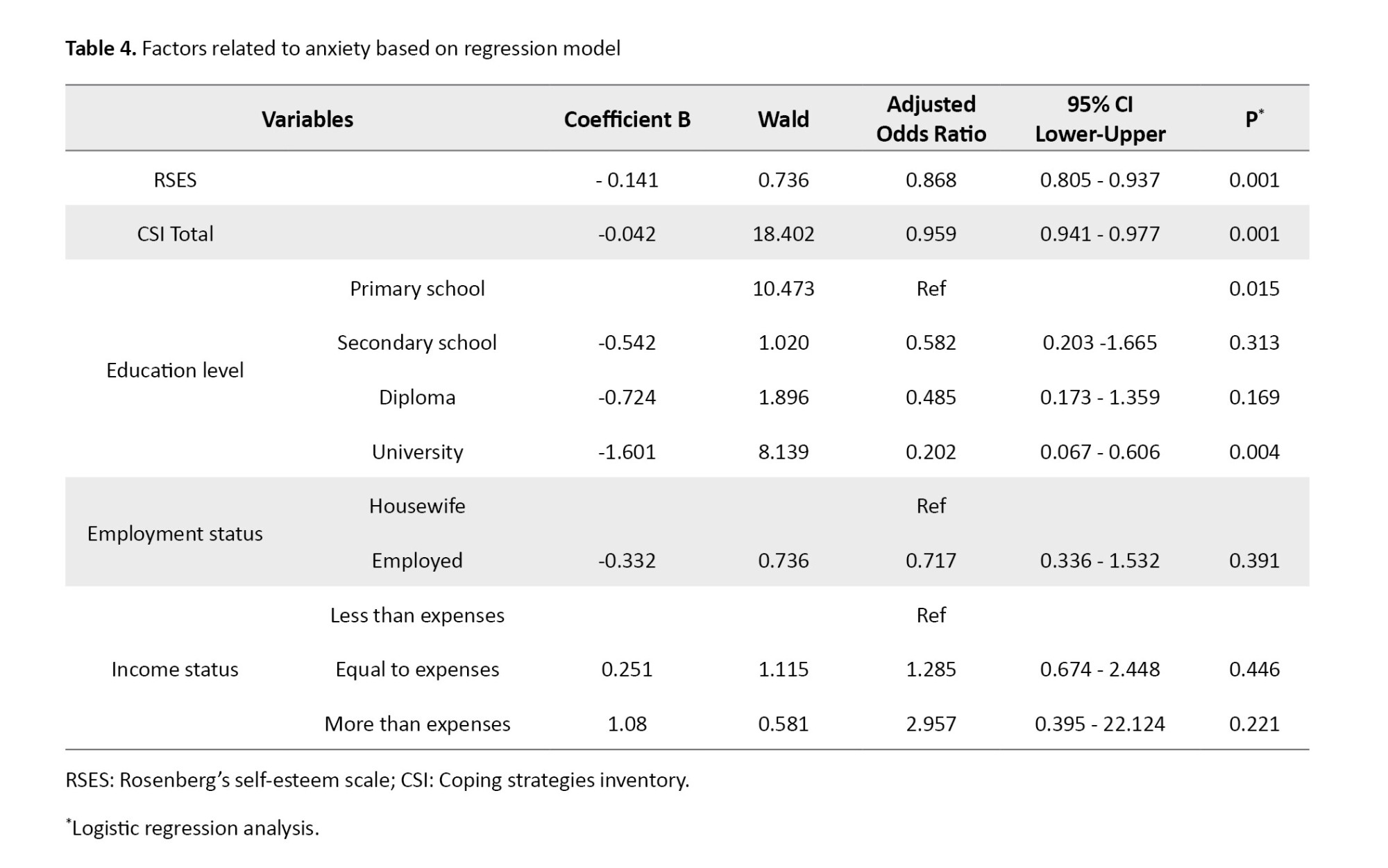
The results of the logistic regression test showed that the five independent variables (self-esteem, coping strategies, educational level, job status, and income level) could explain 22.8% to 30.4% of the anxiety variations in women. Based on the obtained results, the self-esteem (OR=0.86, 95% CI, 0.80, 0.93, P=0.001), coping strategies (OR=0.95, 95% CI, 0.94, 0.97, P=0.001), and education levels (OR=0.20, 95% CI, 0.06, 0.60, P=0.001) were significantly capable of explaining the variations of the dependent variable.
According to the result, with one unit increase in self-esteem and coping strategies, the anxiety level decreases by 13.2% and 7.5%, respectively. Also, an increase in the educational level was associated with a rise of 79.8% in the anxiety level (Table 4).
Discussion
Our study results found a significant inverse relationship between the independent variables (self-esteem and coping strategies) and the dependent variable (anxiety). Additionally, these independent variables, along with women’s education levels, could significantly explain the anxiety variable.
This study observed that the self-esteem levels were satisfactory, and most women reported high self-esteem. In the study in Turkey, the self-esteem level of the women undergoing gynecological examination was reported to be good [13]. Studies have shown that self-esteem affects fertility and women’s health and can also be effective in making fertility health-related decisions [29-31]. In this study, the mean total score of coping strategies was medium. People exhibit unique coping mechanisms when confronting events in their lives; nevertheless, the coping strategies are trainable and can be helpful for individuals when facing stressful and anxiety-creating factors [14, 32]. Furthermore, studies have shown that younger women, especially adolescents, cannot cope with problems appropriately, and in stressful situations such as gynecological examinations, not being alone before and during the examination, and also being with a supportive relative can help the adolescents to cope with the anxiety-creating situation [8, 33]. Therefore, it seems that social support, especially by health care givers and family, can be helpful because this component is one of the strategies that has been used even by the women participating in the present study.
Based on the present study’s findings, self-esteem has a direct and significant relationship with the total score of coping strategies and their components, except avoidance. The results indicate that individuals with high self-esteem use the “reassessment” component more than others and the “avoidance” strategy less. It has been shown that the preferential coping strategies of the individuals can affect the interventional strategy for improving the disliked aspects of the gynecological examination. Some individuals usually seek information as the main strategy for coping with their existing conditions. Most seek kindness and respect from the caregiver and examiner to overcome the stress of receiving information [13, 34]. It seems that individuals with high self-esteem can use more coping strategies, both of which affect the reduction of anxiety levels.
Another important finding of this study was that the mean total score of anxiety was at a medium level, and most women had experienced mild levels of anxiety. The review of the literature shows that women undergoing gynecological examination report medium levels of anxiety [8, 17, 35]. In the present study, the obtained results indicated no statistically significant difference between age, number of pregnancies, cause of referral for health care, duration of the problem, and the number of anxiety-associated examinations. However, the women with high educational levels, job status, and income levels experienced significantly lower levels of anxiety compared to those with low educational levels, job status, and income sufficiency levels. The study conducted by Timur et al. in Turkey shows no significant relations between the age, marital status, and employment status of women and their anxiety level, which is consistent with the findings of the present work [5]. Moreover, in Hilden et al.’s study in Denmark [36], younger women report higher levels of anxiety. Some studies have shown a significant relationship between age [8, 37] and job [1] with anxiety. However, other studies have shown no significant relationship between age [7, 38], job status [5], and marital status [1] with anxiety. The discrepancy between the results of different studies can be attributed to the study time since some studies have been conducted before the examination. Also, some studies have been web-based and conducted a long while after the exam, which might have affected the recall of the experiences. Using different instruments to assess anxiety might be another reason for the difference in results. However, it seems that higher education and income levels, which are associated with more access to information about gynecological examinations, can affect anxiety levels.
In the present study, the majority of women had a sense of embarrassment. Also, most of them felt stress, pain, and fear. All of these feelings had a significant relationship with anxiety levels. In Timur et al.’s study [5], most women report a sense of embarrassment and express feeling upset for showing their sexual organs. Kartal et al. found that 60% of the women felt embarrassed before the gynecological examination [39]. As reported by researchers, women often prefer to be examined by female physicians, and a reason for such a choice is the respectful behavior of the female caregivers during the examination [7, 39].
Finally, the regression analysis showed that the five variables “entered” into the model could explain the variations of the dependent variable, anxiety. Also, the three variables of educational level, self-esteem, and coping strategies could significantly predict the anxiety variations, and an increase in each of them could contribute to the reduction of anxiety. As mentioned in earlier studies, factors such as self-efficacy and self-esteem can contribute to the reaction induced by stressful situations. If we accept that self-esteem is an important and effective variable in individuals’ coping strategies against stressful situations, promoting self-esteem can play a major role in managing and controlling stress and anxiety.
In general, the findings of the present study provided evidence-based information about the self-esteem status, the applied coping strategies, and the anxiety levels among Iranian women undergoing gynecological examinations. Although the self-esteem among the women was at a satisfactory level, and these women used different strategies for coping with the anxiety-creating situations, most women had experienced various levels of anxiety. Finally, it must be noted that having positive experiences in clinical examinations can encourage women to make timely referrals. Also, it is better to design interventions based on the demands of the under-gynecological examination women, and designing such interventions necessitates exact investigations for a better understanding of the women’s needs and other effective factors. Using a questionnaire to examine purely subjective variables was one of the limitations of the present study.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by Ethics Committee of Tabriz Medical Sciences Branch, Islamic Azad University, Tabriz, Iran (Code: IR.IAU.TABRIZ.REC.1401.011). Relevant guidelines and regulations were available in all methods. Ethical considerations were followed throughout the data collection and analysis. Written informed consent was obtained from the participants before data collection.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization, data analysis, and interpretation: Azita Fathnezhad-Kazemi; Data collection, administration, and writing the original draft: Fatemeh Khalili and Minoo Ranjbar; Review and editing: Azita Fathnezhad-Kazemi and Minoo Ranjbar; Study design and final approval: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors thank the women who participated in the study. We also appreciate the support from Tabriz Medical Sciences Branch, Islamic Azad University, Tabriz, Iran.
References
Performing regular gynecological exams for the prognosis of venereal infections, vaginal cancers, and adverse conditions is very important for looking after women’s health [1, 2]. Also, gynecological examinations, including the bimanual and speculum exams, are common for periodic control of women [3]. Annual pelvic examinations, especially for cervical cancer screening, have been emphasized by the American Cancer Society (ACS) and the US Preventive Services Task Force (USPSTF) [4].
Most women experience undesirable feelings such as embarrassment and loss of control during sexual organ examinations, and they believe that sexual organs are a private part of their body and must be covered and concealed [5, 6]. Therefore, pelvic examinations might cause reactions such as mild to severe anxiety and embarrassment, which may result in the avoidance of the examinations and referral to physicians for health care services [5, 7]. Hereditary characteristics, gender, personality, emotional state, intelligence, social role and position, creativity, and social interaction contribute to the formation and variation of anxiety in people [8].
Self-esteem is one of the major aspects of adaptation in all life stages, contributing to emotional, social, and psychological adaptation. Low self-esteem can intensify anxiety [9, 10]. High self-esteem in an individual would result in self-confidence, enabling the individual to adapt to difficult conditions [10-12]. A study on girls showed a negative relationship between self-esteem and anxiety [13].
In addition, the most important factors affecting mental health include the manner of coping with stressful situations and life challenges. Some individuals lose their capability to cope with problems and challenging conditions very soon and experience anxiety [14]. Coping and adaptation to anxiety and stress are very important in women undergoing pelvic examinations [15, 16]. In a study on adolescents undergoing pelvic examination for the first time, results indicate a reverse relationship between the anxiety level and the self-confidence approach and optimistic coping strategy. Also, there is a direct relationship between anxiety, obedience, and a hopeless approach [8].
Due to various reasons such as religious and cultural differences, it is highly important to investigate the level of anxiety, self-esteem, and strategies of coping with and adaptation to stressful situations that may be created [3]. So, we conducted a study to investigate the role of self-esteem and coping strategies in pelvic examination-induced anxiety.
Materials and Methods
This cross-sectional study was conducted on 270 women attending obstetrics and gynecology clinics in one of the teaching and treatment centers in Tabriz City, Iran, during the first 6 months of 2022. They were selected using a convenience sampling method. The inclusion criteria were as follows: Women aged 18 and above, ability to read and write in Persian, absence of taking antidepressants, absence of chronic disease such as diabetes, having a genital examination during the visit, and willingness to participate in the study. The exclusion criterion was failure to complete the questionnaire.
The sample size was estimated at 243 cases based on the prevalence of anxiety reported by Yilmaz and Demirel’s study in Turkey; P=28.9% [17]. However, considering an increase in the study’s accuracy by 10%, the final sample size was calculated as 270 cases. Other parameters used were α=0.05, power=0.80, and d=20%.
The following four questionnaires were used to collect the data. The sociodemographic and obstetrics characteristics checklist consists of the sociodemographic variables of age, educational level, occupational status of women, self-assessment of household economic status, as well as obstetrics characteristics, including the number of pregnancies, the reason for the application to the gynecology clinic, duration of gynecological examination, and experienced emotion during gynecological examination.
The Rosenberg Self-esteem Scale (RSES) was developed by Rosenberg [18]. The scale consists of 10 items, five positive and five negative statements, and 12 categories to measure self-esteem. RSES is scored on a 4-point scale with response options ranging from 1=not at all true of me to 4=very true of me. Five items are inversely scored. Items 1, 2, 4, 6, and 7 investigate one’s positive self-evaluation and are scored from 3 to 0. Items 3, 5, 8, 9, and 10 investigate one’s negative self-evaluation and are scored from 0 to 3. Satisfactory self-esteem is defined as higher than or equal to 30 on the Rosenberg scale [19]. Joshanloo and Ghaedi assessed the validity and reliability of this scale in Iran [20].
Lazarus and Folkman compiled the Coping Strategies Inventory (CSI) in 1985 [21]. It comprises 66 items divided into 8 subscales: Confrontation, distancing, self-control, social support, accepting responsibility, escape-avoidance, problem-solving, and positive reappraisal. The respondents must indicate what they did in a given situation according to the classification, ranging from 0- a strategy not used; 1- used somewhat; 2- used quite a bit; to 3- used a great deal [22, 23]. This tool was used in many Iranian studies [24, 25].
Zung et al. designed the Situational Anxiety Scores (SAS) [26]. This scale included 20 questions about psychotic emotional symptoms, psychomotor disturbance, somatic disorder, and mental disorders of anxiety or depression. To answer each question, volunteers select the option that best describes their mental state. Each question is scored on a Likert-type scale of 1 to 4 or reverse scoring (“a little of the time”, “some of the time,” “a good part of the time”, and “most of the time”). On this scale, the maximum score is 80. The raw total scores were obtained by summarizing the total scores of the 20 questions and were converted to percentile standard scores. A final score of more than 50 was considered an anxiety symptom. Scores of 50–59, 60–69, and 70 or more are classified as mild, moderate, and severe anxiety, respectively [27]. In Iran, this tool was used in a study [28].
The reliability of questionnaires was assessed using the Cronbach α method in 20 women who had a pelvic examination. Thus, the reliability of self-esteem, coping strategies, and anxiety tools were found to be 0.82, 0.74, and 0.89, respectively.
The sampling was performed by acquiring the ethics permit from the Islamic Azad University of Tabriz Medical Sciences Ethics Committee and obtaining permission from the hospital authorities. All participants completed the questionnaires using the self-report method. Before recruiting the participants, they were informed about the study’s aims and their voluntary participation. If participants had problems understanding the questionnaire items while completing it, the author would answer them immediately.
The quantitative data were analyzed using SPSS software, version 24. First, frequency, percentage, and Mean±SD were determined using descriptive statistics. The normal distribution of the data was evaluated using the Kolmogorov-Smirnov test, skewness, and kurtosis. The Pearson correlation, Analysis of Variance (ANOVA), and t-test were used to determine the relationship between demographic and obstetric variables with the main research variables. Bivariate logistic regression with the “enter” method was used to investigate predictors of anxiety. The two-dimensional variable of anxiety (below 50 and above 50 scores) and the independent variables of coping strategies, self-esteem, and demographic variables with a significant level were entered into the model. The level of significance in this study was set at P<0.05.
Results
A total of 270 women who underwent gynecological examination participated in the study. In the present study, the Mean±SD age of the women was 38.03±9.05 years (range: 18-61 years). Most participants (67.2%) had high educational levels (high school diplomas and academic degrees). Nearly 79% of them had no job. Among the participants, 236(87.4%) were married and 34(12.6%) were divorced. Most of these women were multiparous, and only 23.3% were experiencing their first gynecological examination. The major cause of referral was bleeding and related problems. Also, the problem’s duration was specified until referral and examination duration. Nearly 85% of them reported a sense of embarrassment during the gynecological examination. Feelings such as stress, pain, and fear were reported in 66%, 62%, and 36% of the cases, respectively.
The examination of anxiety in different age groups showed that anxiety in the age group of 30-40 years was higher than in other groups; however, no statistical difference was observed between different age groups. The results indicate that the difference between the SAS in terms of educational level, job status, and income level was statistically significant. Hence, women with academic degrees experienced lower anxiety than other educational groups (P=0.001). These results were shown in Table 1.
The Mean±SD of the SAS score of the participant women was 50±11.72 (range: 26-83.75). Based on the obtained results, 45.2% of the women experienced different levels of anxiety, including mild, medium, and severe levels. Their Mean±SD self-esteem score was equal to 33.59±4.05. So, based on the classification, almost 82% of the women had a satisfactory level of self-esteem. The coping strategies investigation showed that the Mean±SD total score on this scale was 69.72±16.74 (Table 2).
Based on the Pearson correlation coefficient results, there were significant reverse correlations between self-esteem (r=-0.441, P=0.001) and coping strategies (r=-0.357, P=0.001) with SAS. All subscales of coping strategies, except distancing and avoidance, had a reverse correlation with anxiety. Although the distancing subscale had a positive relationship with anxiety, this relationship was not significant. However, the avoidance subscale showed a significant positive relationship (r=0.267, P=0.001) with anxiety (Table 3).
The results of the logistic regression test showed that the five independent variables (self-esteem, coping strategies, educational level, job status, and income level) could explain 22.8% to 30.4% of the anxiety variations in women. Based on the obtained results, the self-esteem (OR=0.86, 95% CI, 0.80, 0.93, P=0.001), coping strategies (OR=0.95, 95% CI, 0.94, 0.97, P=0.001), and education levels (OR=0.20, 95% CI, 0.06, 0.60, P=0.001) were significantly capable of explaining the variations of the dependent variable.
According to the result, with one unit increase in self-esteem and coping strategies, the anxiety level decreases by 13.2% and 7.5%, respectively. Also, an increase in the educational level was associated with a rise of 79.8% in the anxiety level (Table 4).
Discussion
Our study results found a significant inverse relationship between the independent variables (self-esteem and coping strategies) and the dependent variable (anxiety). Additionally, these independent variables, along with women’s education levels, could significantly explain the anxiety variable.
This study observed that the self-esteem levels were satisfactory, and most women reported high self-esteem. In the study in Turkey, the self-esteem level of the women undergoing gynecological examination was reported to be good [13]. Studies have shown that self-esteem affects fertility and women’s health and can also be effective in making fertility health-related decisions [29-31]. In this study, the mean total score of coping strategies was medium. People exhibit unique coping mechanisms when confronting events in their lives; nevertheless, the coping strategies are trainable and can be helpful for individuals when facing stressful and anxiety-creating factors [14, 32]. Furthermore, studies have shown that younger women, especially adolescents, cannot cope with problems appropriately, and in stressful situations such as gynecological examinations, not being alone before and during the examination, and also being with a supportive relative can help the adolescents to cope with the anxiety-creating situation [8, 33]. Therefore, it seems that social support, especially by health care givers and family, can be helpful because this component is one of the strategies that has been used even by the women participating in the present study.
Based on the present study’s findings, self-esteem has a direct and significant relationship with the total score of coping strategies and their components, except avoidance. The results indicate that individuals with high self-esteem use the “reassessment” component more than others and the “avoidance” strategy less. It has been shown that the preferential coping strategies of the individuals can affect the interventional strategy for improving the disliked aspects of the gynecological examination. Some individuals usually seek information as the main strategy for coping with their existing conditions. Most seek kindness and respect from the caregiver and examiner to overcome the stress of receiving information [13, 34]. It seems that individuals with high self-esteem can use more coping strategies, both of which affect the reduction of anxiety levels.
Another important finding of this study was that the mean total score of anxiety was at a medium level, and most women had experienced mild levels of anxiety. The review of the literature shows that women undergoing gynecological examination report medium levels of anxiety [8, 17, 35]. In the present study, the obtained results indicated no statistically significant difference between age, number of pregnancies, cause of referral for health care, duration of the problem, and the number of anxiety-associated examinations. However, the women with high educational levels, job status, and income levels experienced significantly lower levels of anxiety compared to those with low educational levels, job status, and income sufficiency levels. The study conducted by Timur et al. in Turkey shows no significant relations between the age, marital status, and employment status of women and their anxiety level, which is consistent with the findings of the present work [5]. Moreover, in Hilden et al.’s study in Denmark [36], younger women report higher levels of anxiety. Some studies have shown a significant relationship between age [8, 37] and job [1] with anxiety. However, other studies have shown no significant relationship between age [7, 38], job status [5], and marital status [1] with anxiety. The discrepancy between the results of different studies can be attributed to the study time since some studies have been conducted before the examination. Also, some studies have been web-based and conducted a long while after the exam, which might have affected the recall of the experiences. Using different instruments to assess anxiety might be another reason for the difference in results. However, it seems that higher education and income levels, which are associated with more access to information about gynecological examinations, can affect anxiety levels.
In the present study, the majority of women had a sense of embarrassment. Also, most of them felt stress, pain, and fear. All of these feelings had a significant relationship with anxiety levels. In Timur et al.’s study [5], most women report a sense of embarrassment and express feeling upset for showing their sexual organs. Kartal et al. found that 60% of the women felt embarrassed before the gynecological examination [39]. As reported by researchers, women often prefer to be examined by female physicians, and a reason for such a choice is the respectful behavior of the female caregivers during the examination [7, 39].
Finally, the regression analysis showed that the five variables “entered” into the model could explain the variations of the dependent variable, anxiety. Also, the three variables of educational level, self-esteem, and coping strategies could significantly predict the anxiety variations, and an increase in each of them could contribute to the reduction of anxiety. As mentioned in earlier studies, factors such as self-efficacy and self-esteem can contribute to the reaction induced by stressful situations. If we accept that self-esteem is an important and effective variable in individuals’ coping strategies against stressful situations, promoting self-esteem can play a major role in managing and controlling stress and anxiety.
In general, the findings of the present study provided evidence-based information about the self-esteem status, the applied coping strategies, and the anxiety levels among Iranian women undergoing gynecological examinations. Although the self-esteem among the women was at a satisfactory level, and these women used different strategies for coping with the anxiety-creating situations, most women had experienced various levels of anxiety. Finally, it must be noted that having positive experiences in clinical examinations can encourage women to make timely referrals. Also, it is better to design interventions based on the demands of the under-gynecological examination women, and designing such interventions necessitates exact investigations for a better understanding of the women’s needs and other effective factors. Using a questionnaire to examine purely subjective variables was one of the limitations of the present study.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by Ethics Committee of Tabriz Medical Sciences Branch, Islamic Azad University, Tabriz, Iran (Code: IR.IAU.TABRIZ.REC.1401.011). Relevant guidelines and regulations were available in all methods. Ethical considerations were followed throughout the data collection and analysis. Written informed consent was obtained from the participants before data collection.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization, data analysis, and interpretation: Azita Fathnezhad-Kazemi; Data collection, administration, and writing the original draft: Fatemeh Khalili and Minoo Ranjbar; Review and editing: Azita Fathnezhad-Kazemi and Minoo Ranjbar; Study design and final approval: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors thank the women who participated in the study. We also appreciate the support from Tabriz Medical Sciences Branch, Islamic Azad University, Tabriz, Iran.
References
- Erbil N, Şenkul A, Sağlam Y, Ergül N. Determination of attitudes with gynecologic examination and anxiety of Turkish women before gynecologic examination. J Hum Sci. 2008; 5(1). [Link]
- Ruiz MJ, Chisholm B, de Martelly V, Chor J. Sexual and gender minority patients' first pelvic examination experiences: What clinicians need to know. J Pediatr Adolesc Gynecol. 2024; 37(3):342-7. [DOI:10.1016/j.jpag.2023.11.008] [PMID]
- Tugut N, Golbasi Z. Aspects of emotional and physical discomfort in gynecologic examination: A study of Turkish women. J Obstet Gynaecol Res. 2014; 40(6):1777-84. [DOI:10.1111/jog.12409] [PMID]
- O'Laughlin DJ, Strelow B, Fellows N, Kelsey E, Peters S, Stevens J, et al. Addressing anxiety and fear during the female pelvic examination. J Prim Care Community Health. 2021; 12:2150132721992195. [DOI:10.1177/2150132721992195] [PMID]
- Tashan Timur S, Uçar T, Aksoy Derya Y, Kucukkelepce Şimsek D. Influence of gynecologic examination anxiety on application period to gynecology. Asian Pac J Health Sci. 2016; 3(2):84-91. [Link]
- Tancman S, HaCohen N, Lazarus G, Solt I, Sagi-Dain L. Silent voices that must be heard - women's perceptions of gynecologic examinations. J Psychosom Obstet Gynaecol. 2022; 43(2):190-7. [DOI:10.1080/0167482X.2020.1864727] [PMID]
- Aktas D, Kumas MB, Odabasıoglu BS, Kaya A. Effect of a special examination gown and nature-based sounds on anxiety in women undergoing a gynecological examination. Clin Nurs Res. 2018; 27(5):521-39. [DOI:10.1177/1054773816686475] [PMID]
- Demirel G, Ertekin Pinar S, Bilgic D. Anxiety levels and methods of coping with stress of adolescents undergoing their first gynecological examination. J Psychosom Obstet Gynaecol. 2020; 41(2):131-6. [DOI:10.1080/0167482X.2019.1643314] [PMID]
- Abolghasemi Nejhad P, Borhaninejad V, Khanjani N, Saber M, Alizadeh S. Investigating the relationship between healthy lifestyle with self-esteem and subjective vitality in the elderly population of Sirjan in 2020. [Unpublished]. [DOI:10.21203/rs.3.rs-1542332/v1]
- Kheirkhah M, Mokarie H, Nisanisamani L, Hosseini AF. [Relationship between anxiety and self-concept in female adolescents (Persian)]. Iran J Nurs. 2013; 26(83):19-29. [Link]
- Sharifi Neyestanak ND, Ghodoosi Boroojeni M, Seyedfatemi N, Heydari M, Hoseini AF. [Self esteem and its associated factors in patients with multiple sclerosis (Persian)]. Iran J Nurs. 2012; 25 (78):14-22. [Link]
- Timkova V, Mikula P, Fedicova M, Szilasiova J, Nagyova I. Psychological well-being in people with multiple sclerosis and its association with illness perception and self-esteem. Mult Scler Relat Disord. 2021; 54:103114. [DOI:10.1016/j.msard.2021.103114] [PMID]
- Bay H, Akin B. Privacy, self-esteem, anxiety in women having pelvic examination. Clin Nurs Res. 2022; 31(7):1376-83.[DOI:10.1177/10547738211058597] [PMID]
- Choy B, Arunachalam K, Gupta S, Taylor M, Lee A. Systematic review: Acculturation strategies and their impact on the mental health of migrant populations. Public Health Pract (Oxf). 2020; 2:100069. [DOI:10.1016/j.puhip.2020.100069] [PMID]
- Hennigen L, Kollar LM, Rosenthal SL. Methods for managing pelvic examination anxiety: Individual differences and relaxation techniques. J Pediatr Health Care. 2000; 14(1):9-12. [DOI:10.1016/S0891-5245(00)70038-1] [PMID]
- Miller SM, Mangan CE. Interacting effects of information and coping style in adapting to gynecologic stress: Should the doctor tell all? J Pers Soc Psychol. 1983; 45(1):223-36. [DOI:10.1037//0022-3514.45.1.223] [PMID]
- Yilmaz FT, Demirel G. The relationship between body privacy and anxiety in women having gynecological examination. J Obstet Gynaecol. 2021; 41(7):1112-5. [DOI:10.1080/01443615.2020.1835845] [PMID]
- Rosenberg M. Rosenberg self-esteem scale (RSE). In: Ciarrochi J, Bilich L, editors. Acceptance and commitment therapy. Measures package. Wollongong: University of Wollongong; 1965. [DOI:10.1037/t01038-000]
- Maçola L, do Vale IN, Carmona EV. [Assessment of self-esteem in pregnant women using Rosenberg's Self-Esteem Scale (Portuguese)]. Rev Esc Enferm USP. 2010; 44(3):570-7. [DOI:10.1590/S0080-62342010000300004] [PMID]
- Joshanloo M, Ghaedi GH. [Reinvestigation of the reliability and validity of the rosenberg self-esteem scale in Iran (Persian)]. Clin Psychol Pers. 2008; 6(2):49-56. [Link]
- Folkman S, Lazarus RS. If it changes it must be a process: Study of emotion and coping during three stages of a college examination. J Pers Soc Psychol. 1985; 48(1):150-70. [DOI:10.1037//0022-3514.48.1.150] [PMID]
- Joshi R, Surira V. Parenting style and coping strategies among adolescents. Int J Indian Psychȯl. 2022; 10(4). [Link]
- Greenaway KH, Louis WR, Parker SL, Kalokerinos EK, Smith JR, Terry DJ. Measures of coping for psychological well-being. In: Boyle GJ, Saklofske DH, Matthews G, editors. Measures of personality and social psychological constructs. Amsterdam: Elsevier; 2015. [DOI:10.1016/B978-0-12-386915-9.00012-7]
- Nedaei A, Paghoosh A, Sadeghi-Hosnijeh A. [Relationship between coping strategies and quality of life: Mediating role of cognitive emotion regulation skills (Persian)]. J Clin Psychol. 2016, 8(4):35-48. [DOI: 10.22075/jcp.2017.2252]
- Mazlum BN, Afkhami AM, Shams EA, Jalali M. [Investigating the simple and multiple resilience and hardiness with problem-oriented and emotional-oriented coping styles in diabetes type 2 in Yazd city (Persian)]. J Diabetes Nurs. 2014; 1(2). [Link]
- Zung WW: A rating instrument for anxiety disorders. Psychosomatics. 1971; 12(6):371-9. [DOI:10.1016/S0033-3182(71)71479-0] [PMID]
- Dong H, Hu R, Lu C, Huang D, Cui D, Huang G, et al. Investigation on the mental health status of pregnant women in China during the Pandemic of COVID-19. Arch Gynecol Obstet. 2021; 303(2):463-9. [DOI:10.1007/s00404-020-05805-x] [PMID]
- Hossein-Sabet F. [Effectiveness of patience training in anxiety, depression and happiness (Persian)]. Stud Islamic Psycholol. 2008, 1(2):79-92. [Link]
- D'Souza MS, Karkada SN, Somayaji G, Venkatesaperumal R. Women's well-being and reproductive health in Indian mining community: Need for empowerment. Reprod Health. 2013; 10:24.[DOI:10.1186/1742-4755-10-24] [PMID]
- Misra R, Srivastava S, Mahajan R, Thakur R. Decision making as a contributor for Women empowerment: A study in the Indian context. J Comp Asian Dev. 2021; 18(1):79-99. [DOI:10.4018/JCAD.2021010104]
- Kiani Z, Simbar M, Dolatian M, Zayeri F. [The relationship between self-esteem and empowerment of women in fertility (Persian)]. J Mazandaran Univ Med Sci. 2017; 27(150):187-91. [Link]
- Stanisławski K. The Coping Circumplex Model: An integrative model of the structure of coping with stress. Front Psychol. 2019; 10:694. [DOI:10.3389/fpsyg.2019.00694] [PMID]
- Gerber M, Brand S, Feldmeth AK, Lang C, Elliot C, Holsboer-Trachsler E, etal. Adolescents with high mental toughness adapt better to perceived stress: A longitudinal study with Swiss vocational students. Pers Individ Dif. 2013; 54(7):808-14. [DOI:10.1016/j.paid.2012.12.003]
- Lin YP, Tsai YF. Maintaining patients' dignity during clinical care: A qualitative interview study. J Adv Nurs. 2011; 67(2):340-8. [DOI:10.1111/j.1365-2648.2010.05498.x] [PMID]
- Ulker K, Kivrak Y. The effect of information about gynecological examination on the anxiety level of women applying to gynecology clinics: A prospective, randomized, controlled study. Iran Red Crescent Med J. 2016; 18(6):e23864. [DOI:10.5812/ircmj.23864] [PMID]
- Hilden M, Sidenius K, Langhoff-Roos J, Wijma B, Schei B. Women's experiences of the gynecologic examination: factors associated with discomfort. Acta Obstet Gynecol Scand. 2003; 82(11):1030-6. [DOI:10.1080/j.1600-0412.2003.00253.x] [PMID]
- Fiddes P, Scott A, Fletcher J, Glasier A. Attitudes towards pelvic examination and chaperones: A questionnaire survey of patients and providers. Contraception. 2003; 67(4):313-7. [DOI:10.1016/S0010-7824(02)00540-1] [PMID]
- Hocaoğlu M, Erşahin AA, Akdeniz E. Evaluation on the practice and behaviour of women applied for gynecology outpatient clinics about screening methods for early diagnosis of breast cancer. Eur J Breast Health. 2017; 13(3):150-5. [DOI:10.5152/ejbh.2017.3230] [PMID]
- Kartal B, Kızılırmak A, Işıkçı H, Akçay L, Ay A: [The anxiety levels of women prior to the application of intrauterine devices (Turkish)]. J Contin Med Educ. 2013: 22:8-13. [Link]
Article Type : Research |
Subject:
General
Received: 2023/09/14 | Accepted: 2025/03/28 | Published: 2025/06/10
Received: 2023/09/14 | Accepted: 2025/03/28 | Published: 2025/06/10
Send email to the article author
| Rights and permissions | |
 | This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
