Mon, Dec 1, 2025
Volume 35, Issue 1 (1-2025)
JHNM 2025, 35(1): 35-44 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Heidari F, Mirbagri F, Moridi M. Effects of Multimedia-based Puberty Health Education on Knowledge, Practice, Self-esteem and Emotion Regulation of Adolescent Girls. JHNM 2025; 35 (1) :35-44
URL: http://hnmj.gums.ac.ir/article-1-2215-en.html
URL: http://hnmj.gums.ac.ir/article-1-2215-en.html



1- Psychology (MSc), Department of Clinical Psychology, Faculty of Medicine, Arak Branch, Islamic Azad University, Arak, Iran.
2- Assistance Professor, Department of Midwifery and Reproductive Health, School of Nursing and Midwifery, Tehran University of Medical Sciences, Tehran, Iran. ,mmoridi@sina.tums.ac.ir
2- Assistance Professor, Department of Midwifery and Reproductive Health, School of Nursing and Midwifery, Tehran University of Medical Sciences, Tehran, Iran. ,
Full-Text [PDF 505 kb]
(444 Downloads)
| Abstract (HTML) (648 Views)
Full-Text: (284 Views)
Introduction
Adolescence is one of the most important and critical stages in life, a transition phase from childhood to adulthood that includes physical, mental and social changes in the person. Globally, about 9-12% of adolescents experience high emotional distress, which negatively affects their daily functioning [1]. It is important to identify the factors that trigger emotional problems in adolescents and consider how they are developed, which suggested that emotional distress is caused by complex interactions of multiple personal and contextual factors [2]. Individual factors include genetic makeup, temperament, cognitive skills, self-esteem, social cognition and moral development. Contextual factors include attachment, parenting styles, parent-child cohesion, family functioning, school environment, relationships with peers, and the broad socio-cultural context [3]. Growing evidence shows that emotional abilities are associated with prosocial behaviors such as stress management and physical health [4]. Teaching adolescents about pubertal changes can help them experience greater self-esteem and better emotional regulation [5]. High self-esteem in individuals, especially adolescents, creates a sense of self-confidence that enables them to adapt to difficult situations in life [6]. Low self-esteem leads to isolation, anger, and anti-social behaviors [7]. One of the most important abilities to improve self-esteem is emotion regulation skills, which are developed in infancy and childhood and continue into adolescence [8]. Physical changes during puberty can intensify low self-esteem and increase anxiety, leading to decreased emotion regulation ability [2].
Adolescents have a limited knowledge of the physical and mental changes during puberty. They get information about these changes mostly from their friends or the internet, who usually share their own experiences or perceptions that are mostly incorrect or incomplete [9]. Qualitative studies on identifying Iranian adolescents’ experiences during puberty have demonstrated that most of the adolescents do not receive any special education on physical and sexual changes in puberty; hence, they get information from their peers [10]. Since conversations about body changes and puberty are taboo among adolescents and in society in Iran, and it is difficult to find a proper source of information about them, many of the changes are ignored. Education to adolescents about how to adapt to the physical and mental conditions during puberty can increase their self-esteem, social, relational, and emotional regulation skills, and satisfaction with life [11]. Modern teaching methods, such as multimedia, have some advantages over traditional teaching methods, such as being more productive, more interesting, more diverse content, and having a higher learning speed [12]. Multimedia-based education can increase the quality of education and students’ ability to put their knowledge into practice. It not only provides a good chance for access to more participants and inhibits the feeling of shame for learning about the body changes, but also develops proper conditions to perceive a substantial amount of information about puberty. A study showed that multimedia-based education increased adolescents’ knowledge of puberty [13].
There is a need to pay attention to the physical and mental health education of adolescent girls in Iran due to their insufficient knowledge. In addition, most of the previous studies have used traditional teaching methods, and a few studies have used educational programs based on modern teaching methods, such as multimedia-based methods, to promote the self-esteem of adolescents in Iran. Therefore, in this study, we aim to assess the effects of multimedia-based physical and psychological puberty health education on self-esteem and emotional regulation of adolescent girls aged 11-14 years in Iran.
Materials and Methods
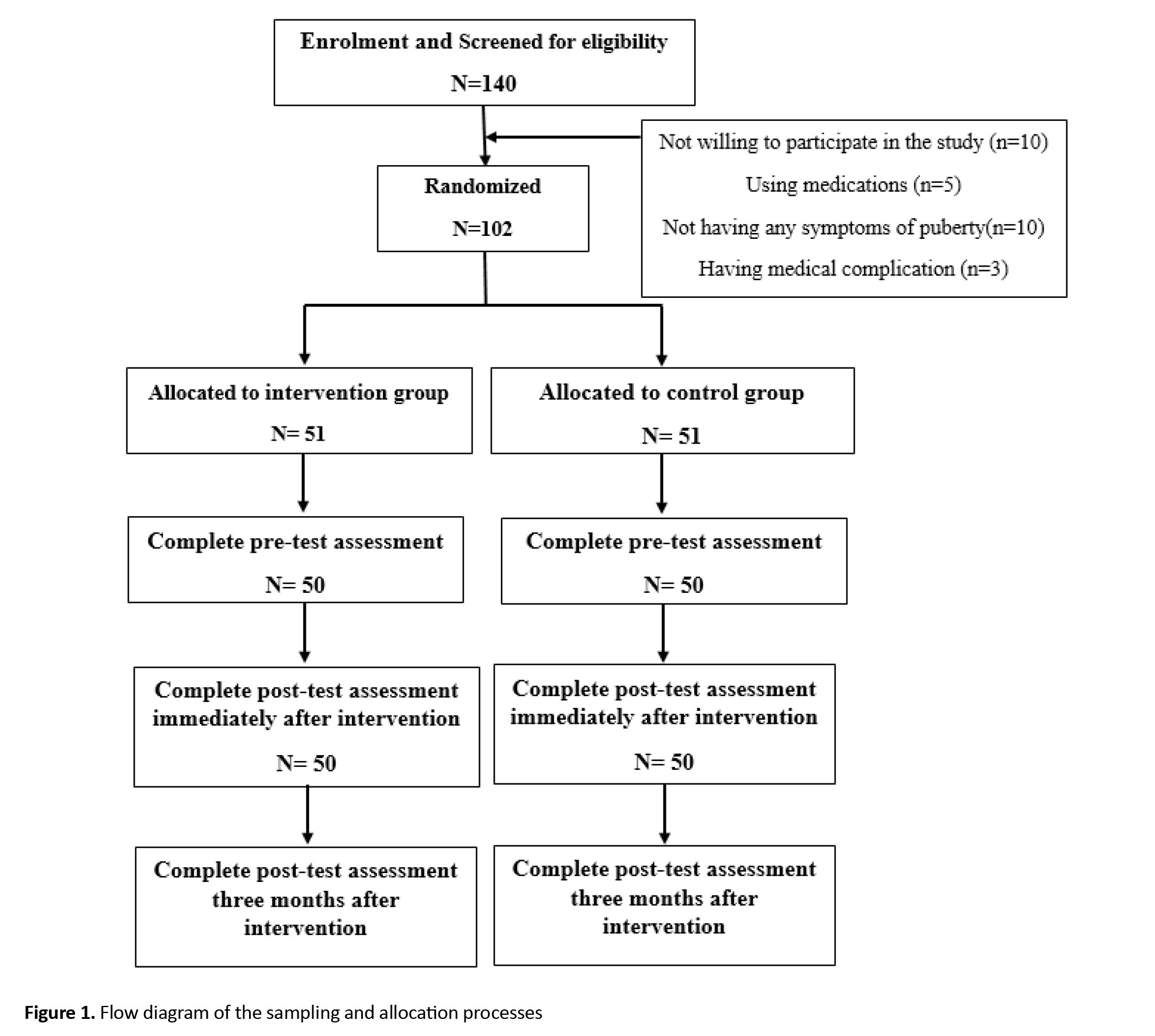
This is a quasi-experimental study with pre-test/post-test/follow-up design that was conducted on 100 adolescent girls aged 11-14 years in Saveh, Markazi Province of Iran, from May to December 2022. The inclusion criteria were: At least two or more symptoms of puberty, being unmarried, no any medical complications, not using any medication, and willingness to participate in the study. Exclusion criteria were absent from two or more sessions or the return of incomplete questionnaires. By considering the mean score of self-esteem before (28.37±2.57) and after (32.17±1.64) educational intervention in Alimohammadi et al.’s study [13], a test power of 95% and a 99% confidence interval, the sample size was estimated at 36.5 per group. Then, considering 40% sample dropout, it increased to 51 per group. The samples were selected from two public middle schools in Saveh City. One of them was randomly selected to recruit students for the intervention group, and the other school was chosen for the control group. Next, 51 eligible adolescent girls were selected randomly from each school. They were randomly divided into two intervention and control groups using the random number table. The parents of students were invited to attend an introduction meeting in which the study objectives and methods were explained entirely to them, and informed consent was obtained from all girls and their parents. Figure 1 shows the CONSORT diagram for the study procedure.
 Four questionnaires were used to collect data before, immediately after, and three months after educational intervention, which included a researcher-made puberty health knowledge scale, a researcher-made puberty health practice scale, the Coopersmith self-esteem inventory (CSEI) and the emotion regulation questionnaire (ERQ). The questionnaires were prepared using the Google Forms. Furthermore, a sociodemographic form with 6 items (age, father’s age, mother’s age, socio-economic status, number of family numbers and source of information about puberty) was completed with the help of parents before the intervention.
Four questionnaires were used to collect data before, immediately after, and three months after educational intervention, which included a researcher-made puberty health knowledge scale, a researcher-made puberty health practice scale, the Coopersmith self-esteem inventory (CSEI) and the emotion regulation questionnaire (ERQ). The questionnaires were prepared using the Google Forms. Furthermore, a sociodemographic form with 6 items (age, father’s age, mother’s age, socio-economic status, number of family numbers and source of information about puberty) was completed with the help of parents before the intervention.
The knowledge scale had 12 items scored as 0 (I do not know or no) and 1 (I know or yes), and the practice scale had 20 items rated on a five-point Likert scale from 1 (strongly disagree) to 5 (strongly agree). The higher scores in both questionnaires indicated higher knowledge and practice of puberty health. For calculating their content validity ratio (CVR) and content validity index (CVI), the opinions of an expert panel consisting of 10 specialists in midwifery, reproductive health, and health education were used. The CVI and CVR values for both questionnaires were up to 0.90 and Cronbach’s α coefficient for the knowledge and practice scales was 0.922 and 0.814, respectively, indicating their high validity and reliability.
The ERQ is a 10-item self-report scale designed to assess the habitual use of two commonly used strategies to regulate emotions: Cognitive reappraisal and expressive suppression [14]. Participants respond to each item using a 7-point Likert scale ranging from 1 (strongly disagree) to 7 (strongly agree) [15]. The CSEI is a self-report tool designed to measure the attitudes toward the self in a variety of areas including family, peers, school and general social activities for adolescents and adults [16]. The CSEI consists of 50 items and yields a global score and four separate scores representing more specific aspects of self-esteem, viz. general self, social self-peers, home parents, and school academic (or professional for adult form). Additional items constitute a lie scale (defensive responses; 8 items). The CSEI items require the participant to report feelings about the self directly and are typically scored using a dichotomous scale (“like me” vs “unlike me”). Thus, CSEI scores can range from 0 to 50, with higher scores reflecting higher self-esteem. A score below average (<25) shows low self-esteem, and a score above average (>25) indicates high self-esteem [17].
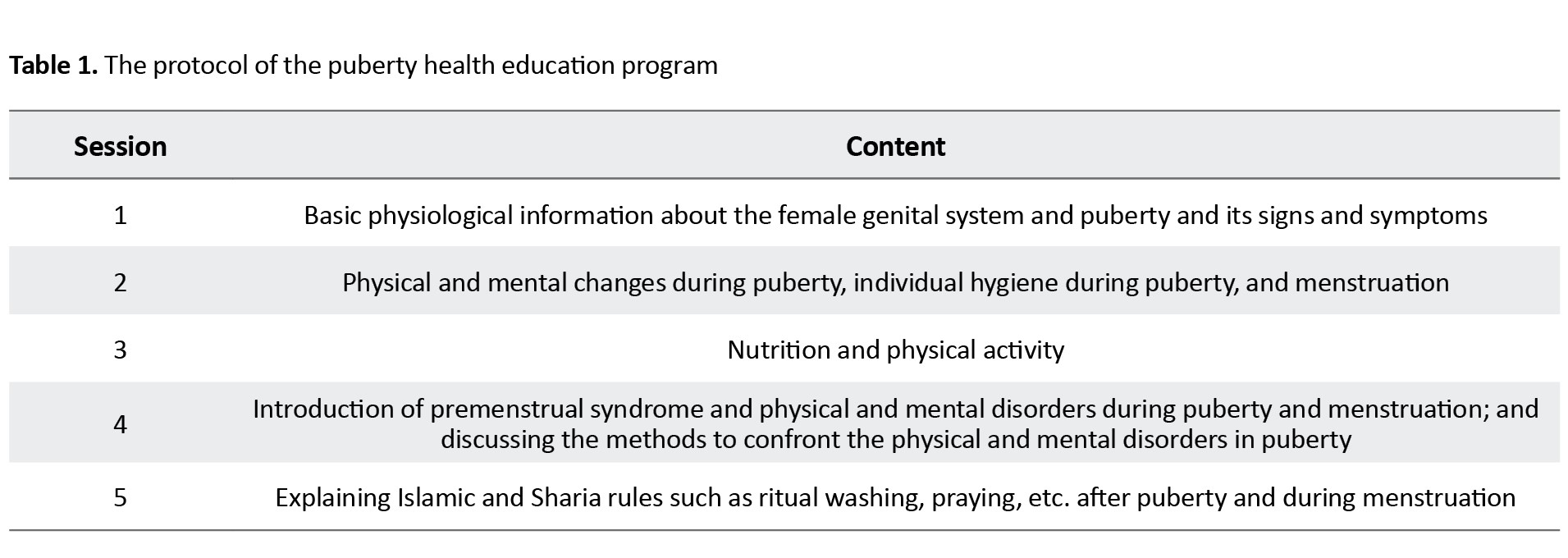
After collecting the baseline data, the educational sessions were held for the intervention group using an Iranian application called “SHAD”, developed by the Iranian Ministry of Education. The students had this app on their computer or smartphone, which is free for all users. By pressing/tapping on the “Student” key button after completing the requested information, they can connect to their classroom. In total, five educational sessions (Table 1) were held (every Saturday at 4:00 PM for 90 minutes).
Between each educational session, the researchers designed educational posters with content and pictures about the physical and mental puberty health and sent them to the students in a social network group created on WhatsApp. This group included all participants in the intervention group No. intervention was done for control group.
The SPSS software, version 24 was used for data analysis. Participants’ characteristics were compared using chi-square test. To measure the difference between the two groups in the pre-intervention phase, Fisher’s exact test was used. Repeated measures of ANOVA and multiple regression analysis were used to compare the mean scores of knowledge, practice, self-esteem and emotional regulation at the pre-test, post-test and follow-up phases. The Greenhouse–Geisser test was used if Mauchly’s test result was significant and the sphericity assumption was applied if Mauchly’s test was not significant. It should be noted that the analyses were performed with the intention-to-treat (ITT) approach. The significance level was set at 0.05.
Results
There was no significant difference between the intervention and control groups in demographic characteristics (Table 2).
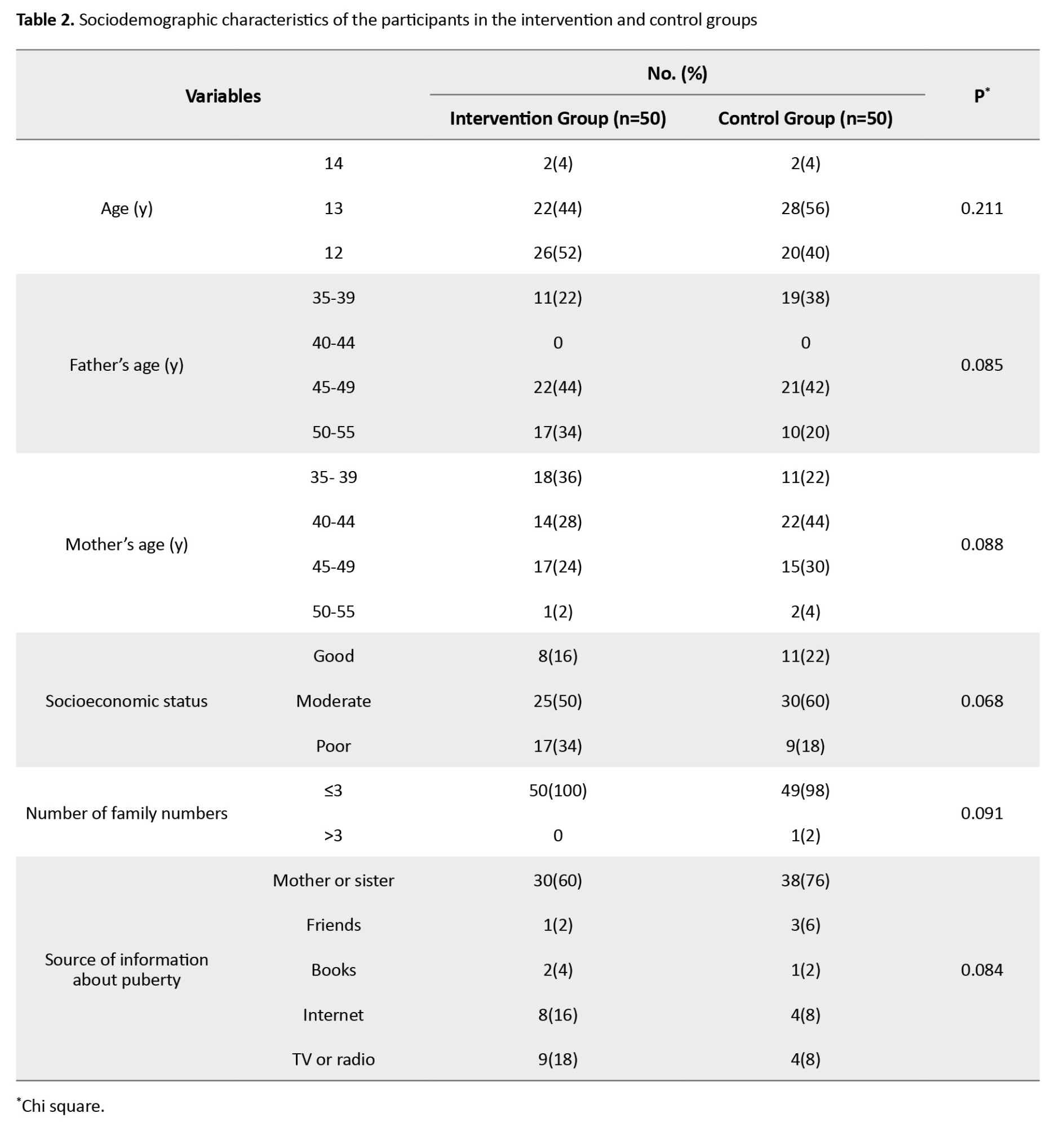
The majority of participants were 13 years old and had moderate socio-economic status. In the control group, the mean scores of physical and psychological knowledge and practice, ERQ and CSEI and their dimensions were not signifcanly different over three time periods (pre-test, post-test and follow-up). However, in the intervention group, the mean scores of these variables were significantly different over time (P<0.05) (Table 3).

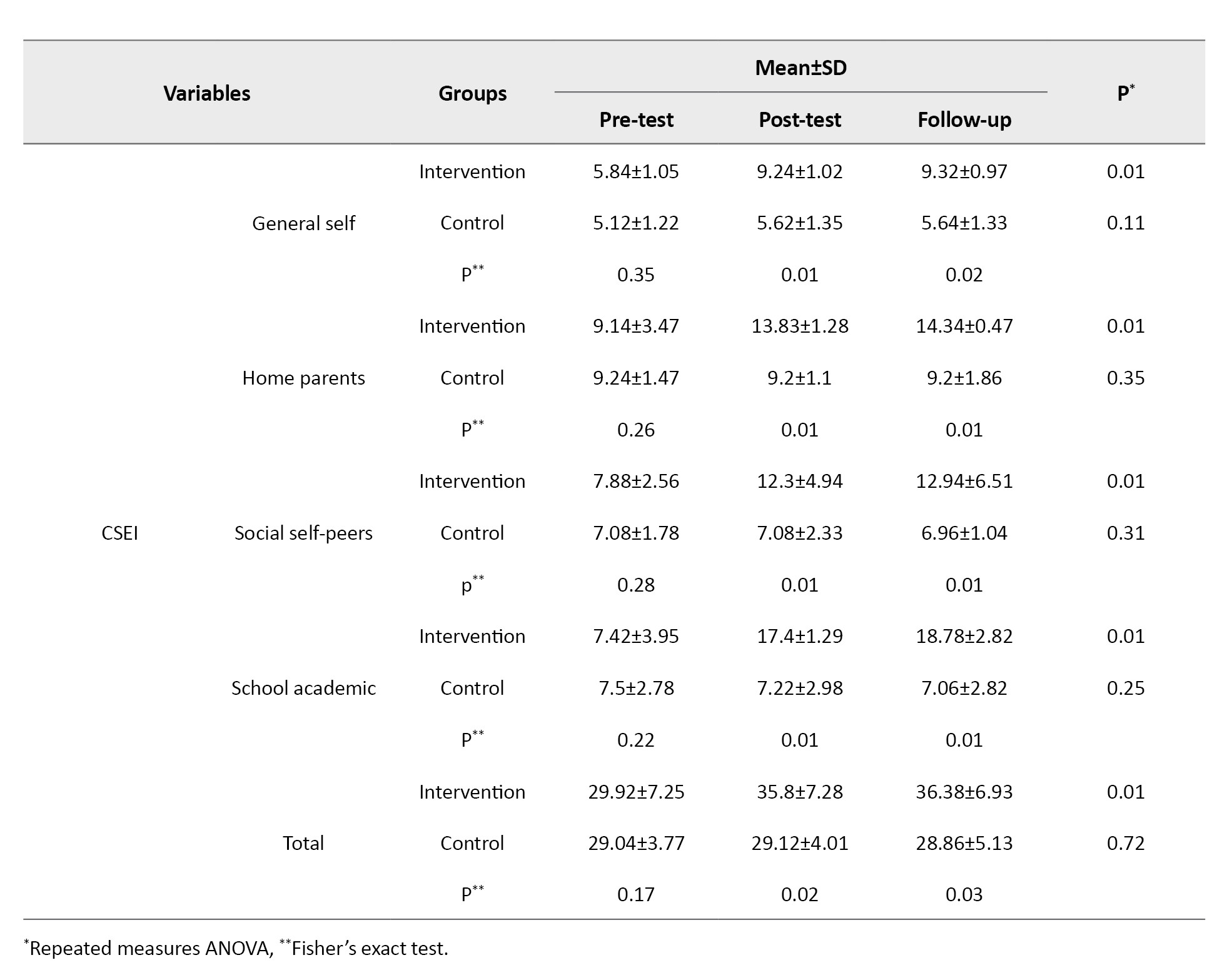
The repeated measure ANOVA results showed that the total puberty health practice scores in the intervention group in the post-test and follow-up phases (68.94±4.84 and 71.68±5.93, respectively) were significantly higher than in the pre-test phase (37.98±6.93) (P=0.001). The scores of ERQ and CSEI in the intervention group also significantly improved in the post-test (56.5±11.83 and 35.8±7.28, respectively) and follow-up (58.08±8.74 and 36.38±9.39, respectively) phases (P=0.01) compared to the pre-test phase. However, in the control group, the ERQ score (44±10.45 in the post-test phase and 43.36±9.39 in the follow-up phase; p=0.12) and CSEI score (29.12±4.01 in the post-test phase and 28.86±5.13 in the follow-up phase; P=0.72) did not change significantly.
The between-group comparisons showed no significant difference between the two groups before intervention in ERQ (P=0.33) and CSEI (P=0.17) scores, but these scores were significantly higher in the intervention group compared to the control group in the post-test (P=0.01 and 0.02, respectively) and follow-up (P=0.02 and 0.03, respectively) phases.
The independent variables, including knowledge and practice in the three time periods, were entered into the logistic regression model using the forward LR approach. The coefficients of the final regression model are presented in Table 4.
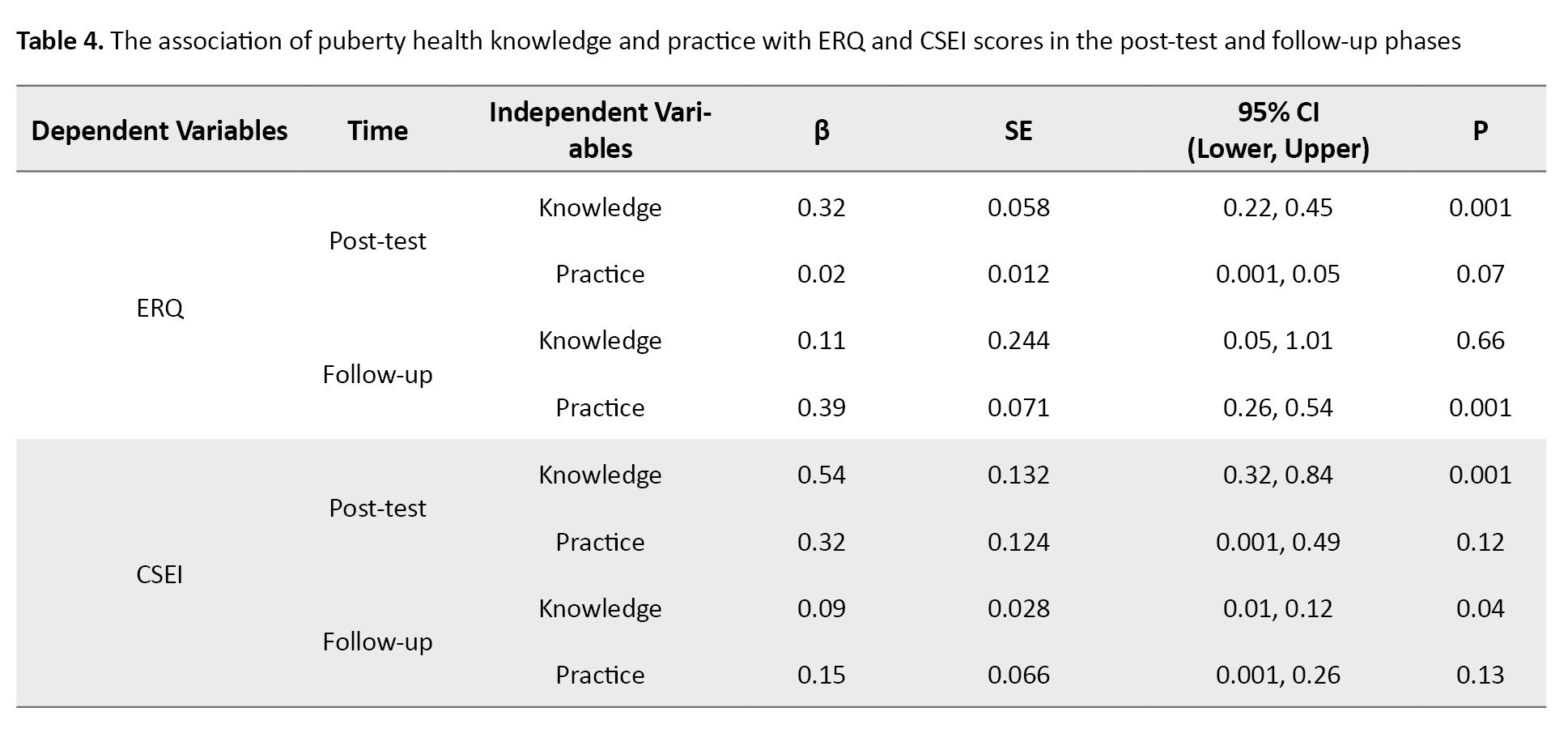
The knowledge factor had a significant association with emotion regulation (β=0.32, 95% CI; 0.22%, 0.45%, P=0.001) and self-esteem (β=0.54, 95% CI; 0.32%, 0.84%, P=0.001) in the post-test phase. In addition, knowledge had a significant association with self-esteem (β=0.09, 95% CI; 0.01%, 0.12%, P=0.04), and practice had a significant association with emotion regulation (β=0.39, 95% CI; 0.26%, 0.54%, P=0.001) in the follow-up phase. According to these findings, for every one unit increase in the knowledge score, the ERQ score increases by 68% and the CSEI score increases by 46% immediately after intervention. Moreover, for every one unit increase in the puberty health practice, the ERQ score increases by 61% three months after the intervention.
Discussion
The results of this study showed that the Iranian adolescent girls’ knowledge and practice of puberty health (physical and psychological) are not at a desirable level. However, their levels increased significantly after educational intervention. A review study on the menstrual health and hygiene knowledge of adolescent girls in low and middle-income countries concluded that girls in these countries are often uninformed and unprepared for puberty [18]. Our results are consistent with the results of studies in Bangladesh [19], Thailand [20] and Iran [10]. The effectiveness of educational interventions about puberty health on knowledge, attitude and practice has also been confirmed in previous studies [9, 21].
In the pre-test phase, self-esteem and emotion regulation did not differ between control and intervention groups. After the intervention, the self-esteem and emotion regulation of the intervention group improved significantly compared to the control group, which did not show significant changes. A study showed that puberty knowledge and practice affected the psychological stress of adolescent girls and concluded that psychological stress management during menstruation should be considered in the health education programs for adolescent girls. During adolescence, healthcare providers should not only pay attention to the physical changes of adolescent girls but also teach them stress management skills to help them cope with menstruation-related concerns [22]. Emotion regulation helps adolescents to flexibly respond to the current situations and needs that lead to new emotions. This flexibility is highly correlated with mental health. Adolescents with effective emotion regulation show better social skills. In contrast, adolescents with difficulty regulating emotions have impaired social functioning and, therefore, receive less social support [23]. Studies have also shown that, by increasing adolescents’ knowledge of puberty health, the adverse effects of body changes on adolescents’ self-esteem can be reduced [11]. Studies have shown that puberty, if ignored, has an adverse impact on adolescents’ self-esteem and emotional regulation. Therefore, teaching puberty-related issues and increasing adolescents’ knowledge in this field is very important for their self-esteem and positive emotional regulation [24]. Alimohammadi et al. showed that multimedia-based puberty health education could increase the self-esteem of adolescent boys [13]. Ning examined the effects of puberty mental health education and stated that the education could solve various psychological problems through emotional communication, emotional guidance and other activities [25]. In line with the present study, a qualitative study from Iran showed that most adolescent girls needed education on how to address issues related to puberty, as puberty was an unpleasant experience for them [10] which can cause psychological stress and reduce adolescents’ emotion regulation and self-esteem.
In the present study, in addition to education about physical and psychological changes during puberty and the strategies to cope with them, the religious rules during puberty and menstruation were taught to the girls, since the studies in Iran have shown that the lack of knowledge of religious rules has an adverse effect on the psychological well-being of adolescent girls [10]. However, the effect of the puberty-related religious rules education on emotion regulation and self-esteem of the girls was not examined separately. It is recommended that the effect of the knowledge and practice regarding puberty-related religious rules be assessed on these variables, especially in Islamic countries where these rules are mandatory.
This is the first study that assesses the effectiveness of multimedia-based puberty health education on self-esteem and emotion regulation of adolescent girls in Iran. One of the limitations of this study was the use of virtual education, which may have affected the quality of teaching and the attendance of adolescents. However, the educational topics were interesting for participants due to the lack of a reliable source of information, which motivated them to participate actively in the sessions. Also, this teaching method eliminates the feeling of shame for asking questions about body parts and puberty that may exist in face-to-face education. Another limitation was that some families prevented the girls’ participation in the training sessions despite their initial informed consent.
The knowledge and practice of puberty health can predict better emotion regulation and self-esteem in adolescent girls. The findings in this study confirm the importance of puberty health education for adolescent girls, especially in Iran, due to the lack of a reliable information source and their shame in seeking the information because of cultural norms. Therefore, health professionals and planners should be aware of and develop puberty health educational programs for improving adolescent girls’ physical and psychological health. This can provide appropriate guidance to foster a healthier lifestyle in girls, particularly those at risk. Further studies are needed to explore the risk and protective factors that can mediate or moderate the adverse developmental problems before implementing educational interventions that are more suitable for local/social contexts.
Ethical Considerations
Compliance with ethical guidelines
The girls and their parents were informed about the study objectives and were free to leave the study anytime. They signed a consent form to participate in the study. The study was conducted according to the principles outlined in the Declaration of Helsinki and approved by the Ethics Committee of the Islamic Azad University, Arak Branch, Arak, Iran (Code: IR.IAU.ARAK.REC.1401.007).
Funding
This study was extracted from a master’s thesis, approved by the Islamic Azad University, Arak Branch, Arak, Iran.
Authors' contributions
Project administration, and writing: Maryam Moridi; Data collection: Fatemeh Mirbagheri and Fatemeh Heidari; Study design, statistical analysis, literature review and final approval: All authors.
Conflict of interest
The authors declared no conflict of interests
Acknowledgments
The authors would like to thank the adolescent girls, their parents, and schools for cooperating in this study.
References
Adolescence is one of the most important and critical stages in life, a transition phase from childhood to adulthood that includes physical, mental and social changes in the person. Globally, about 9-12% of adolescents experience high emotional distress, which negatively affects their daily functioning [1]. It is important to identify the factors that trigger emotional problems in adolescents and consider how they are developed, which suggested that emotional distress is caused by complex interactions of multiple personal and contextual factors [2]. Individual factors include genetic makeup, temperament, cognitive skills, self-esteem, social cognition and moral development. Contextual factors include attachment, parenting styles, parent-child cohesion, family functioning, school environment, relationships with peers, and the broad socio-cultural context [3]. Growing evidence shows that emotional abilities are associated with prosocial behaviors such as stress management and physical health [4]. Teaching adolescents about pubertal changes can help them experience greater self-esteem and better emotional regulation [5]. High self-esteem in individuals, especially adolescents, creates a sense of self-confidence that enables them to adapt to difficult situations in life [6]. Low self-esteem leads to isolation, anger, and anti-social behaviors [7]. One of the most important abilities to improve self-esteem is emotion regulation skills, which are developed in infancy and childhood and continue into adolescence [8]. Physical changes during puberty can intensify low self-esteem and increase anxiety, leading to decreased emotion regulation ability [2].
Adolescents have a limited knowledge of the physical and mental changes during puberty. They get information about these changes mostly from their friends or the internet, who usually share their own experiences or perceptions that are mostly incorrect or incomplete [9]. Qualitative studies on identifying Iranian adolescents’ experiences during puberty have demonstrated that most of the adolescents do not receive any special education on physical and sexual changes in puberty; hence, they get information from their peers [10]. Since conversations about body changes and puberty are taboo among adolescents and in society in Iran, and it is difficult to find a proper source of information about them, many of the changes are ignored. Education to adolescents about how to adapt to the physical and mental conditions during puberty can increase their self-esteem, social, relational, and emotional regulation skills, and satisfaction with life [11]. Modern teaching methods, such as multimedia, have some advantages over traditional teaching methods, such as being more productive, more interesting, more diverse content, and having a higher learning speed [12]. Multimedia-based education can increase the quality of education and students’ ability to put their knowledge into practice. It not only provides a good chance for access to more participants and inhibits the feeling of shame for learning about the body changes, but also develops proper conditions to perceive a substantial amount of information about puberty. A study showed that multimedia-based education increased adolescents’ knowledge of puberty [13].
There is a need to pay attention to the physical and mental health education of adolescent girls in Iran due to their insufficient knowledge. In addition, most of the previous studies have used traditional teaching methods, and a few studies have used educational programs based on modern teaching methods, such as multimedia-based methods, to promote the self-esteem of adolescents in Iran. Therefore, in this study, we aim to assess the effects of multimedia-based physical and psychological puberty health education on self-esteem and emotional regulation of adolescent girls aged 11-14 years in Iran.
Materials and Methods
This is a quasi-experimental study with pre-test/post-test/follow-up design that was conducted on 100 adolescent girls aged 11-14 years in Saveh, Markazi Province of Iran, from May to December 2022. The inclusion criteria were: At least two or more symptoms of puberty, being unmarried, no any medical complications, not using any medication, and willingness to participate in the study. Exclusion criteria were absent from two or more sessions or the return of incomplete questionnaires. By considering the mean score of self-esteem before (28.37±2.57) and after (32.17±1.64) educational intervention in Alimohammadi et al.’s study [13], a test power of 95% and a 99% confidence interval, the sample size was estimated at 36.5 per group. Then, considering 40% sample dropout, it increased to 51 per group. The samples were selected from two public middle schools in Saveh City. One of them was randomly selected to recruit students for the intervention group, and the other school was chosen for the control group. Next, 51 eligible adolescent girls were selected randomly from each school. They were randomly divided into two intervention and control groups using the random number table. The parents of students were invited to attend an introduction meeting in which the study objectives and methods were explained entirely to them, and informed consent was obtained from all girls and their parents. Figure 1 shows the CONSORT diagram for the study procedure.
The knowledge scale had 12 items scored as 0 (I do not know or no) and 1 (I know or yes), and the practice scale had 20 items rated on a five-point Likert scale from 1 (strongly disagree) to 5 (strongly agree). The higher scores in both questionnaires indicated higher knowledge and practice of puberty health. For calculating their content validity ratio (CVR) and content validity index (CVI), the opinions of an expert panel consisting of 10 specialists in midwifery, reproductive health, and health education were used. The CVI and CVR values for both questionnaires were up to 0.90 and Cronbach’s α coefficient for the knowledge and practice scales was 0.922 and 0.814, respectively, indicating their high validity and reliability.
The ERQ is a 10-item self-report scale designed to assess the habitual use of two commonly used strategies to regulate emotions: Cognitive reappraisal and expressive suppression [14]. Participants respond to each item using a 7-point Likert scale ranging from 1 (strongly disagree) to 7 (strongly agree) [15]. The CSEI is a self-report tool designed to measure the attitudes toward the self in a variety of areas including family, peers, school and general social activities for adolescents and adults [16]. The CSEI consists of 50 items and yields a global score and four separate scores representing more specific aspects of self-esteem, viz. general self, social self-peers, home parents, and school academic (or professional for adult form). Additional items constitute a lie scale (defensive responses; 8 items). The CSEI items require the participant to report feelings about the self directly and are typically scored using a dichotomous scale (“like me” vs “unlike me”). Thus, CSEI scores can range from 0 to 50, with higher scores reflecting higher self-esteem. A score below average (<25) shows low self-esteem, and a score above average (>25) indicates high self-esteem [17].
After collecting the baseline data, the educational sessions were held for the intervention group using an Iranian application called “SHAD”, developed by the Iranian Ministry of Education. The students had this app on their computer or smartphone, which is free for all users. By pressing/tapping on the “Student” key button after completing the requested information, they can connect to their classroom. In total, five educational sessions (Table 1) were held (every Saturday at 4:00 PM for 90 minutes).
Between each educational session, the researchers designed educational posters with content and pictures about the physical and mental puberty health and sent them to the students in a social network group created on WhatsApp. This group included all participants in the intervention group No. intervention was done for control group.
The SPSS software, version 24 was used for data analysis. Participants’ characteristics were compared using chi-square test. To measure the difference between the two groups in the pre-intervention phase, Fisher’s exact test was used. Repeated measures of ANOVA and multiple regression analysis were used to compare the mean scores of knowledge, practice, self-esteem and emotional regulation at the pre-test, post-test and follow-up phases. The Greenhouse–Geisser test was used if Mauchly’s test result was significant and the sphericity assumption was applied if Mauchly’s test was not significant. It should be noted that the analyses were performed with the intention-to-treat (ITT) approach. The significance level was set at 0.05.
Results
There was no significant difference between the intervention and control groups in demographic characteristics (Table 2).
The majority of participants were 13 years old and had moderate socio-economic status. In the control group, the mean scores of physical and psychological knowledge and practice, ERQ and CSEI and their dimensions were not signifcanly different over three time periods (pre-test, post-test and follow-up). However, in the intervention group, the mean scores of these variables were significantly different over time (P<0.05) (Table 3).
The repeated measure ANOVA results showed that the total puberty health practice scores in the intervention group in the post-test and follow-up phases (68.94±4.84 and 71.68±5.93, respectively) were significantly higher than in the pre-test phase (37.98±6.93) (P=0.001). The scores of ERQ and CSEI in the intervention group also significantly improved in the post-test (56.5±11.83 and 35.8±7.28, respectively) and follow-up (58.08±8.74 and 36.38±9.39, respectively) phases (P=0.01) compared to the pre-test phase. However, in the control group, the ERQ score (44±10.45 in the post-test phase and 43.36±9.39 in the follow-up phase; p=0.12) and CSEI score (29.12±4.01 in the post-test phase and 28.86±5.13 in the follow-up phase; P=0.72) did not change significantly.
The between-group comparisons showed no significant difference between the two groups before intervention in ERQ (P=0.33) and CSEI (P=0.17) scores, but these scores were significantly higher in the intervention group compared to the control group in the post-test (P=0.01 and 0.02, respectively) and follow-up (P=0.02 and 0.03, respectively) phases.
The independent variables, including knowledge and practice in the three time periods, were entered into the logistic regression model using the forward LR approach. The coefficients of the final regression model are presented in Table 4.
The knowledge factor had a significant association with emotion regulation (β=0.32, 95% CI; 0.22%, 0.45%, P=0.001) and self-esteem (β=0.54, 95% CI; 0.32%, 0.84%, P=0.001) in the post-test phase. In addition, knowledge had a significant association with self-esteem (β=0.09, 95% CI; 0.01%, 0.12%, P=0.04), and practice had a significant association with emotion regulation (β=0.39, 95% CI; 0.26%, 0.54%, P=0.001) in the follow-up phase. According to these findings, for every one unit increase in the knowledge score, the ERQ score increases by 68% and the CSEI score increases by 46% immediately after intervention. Moreover, for every one unit increase in the puberty health practice, the ERQ score increases by 61% three months after the intervention.
Discussion
The results of this study showed that the Iranian adolescent girls’ knowledge and practice of puberty health (physical and psychological) are not at a desirable level. However, their levels increased significantly after educational intervention. A review study on the menstrual health and hygiene knowledge of adolescent girls in low and middle-income countries concluded that girls in these countries are often uninformed and unprepared for puberty [18]. Our results are consistent with the results of studies in Bangladesh [19], Thailand [20] and Iran [10]. The effectiveness of educational interventions about puberty health on knowledge, attitude and practice has also been confirmed in previous studies [9, 21].
In the pre-test phase, self-esteem and emotion regulation did not differ between control and intervention groups. After the intervention, the self-esteem and emotion regulation of the intervention group improved significantly compared to the control group, which did not show significant changes. A study showed that puberty knowledge and practice affected the psychological stress of adolescent girls and concluded that psychological stress management during menstruation should be considered in the health education programs for adolescent girls. During adolescence, healthcare providers should not only pay attention to the physical changes of adolescent girls but also teach them stress management skills to help them cope with menstruation-related concerns [22]. Emotion regulation helps adolescents to flexibly respond to the current situations and needs that lead to new emotions. This flexibility is highly correlated with mental health. Adolescents with effective emotion regulation show better social skills. In contrast, adolescents with difficulty regulating emotions have impaired social functioning and, therefore, receive less social support [23]. Studies have also shown that, by increasing adolescents’ knowledge of puberty health, the adverse effects of body changes on adolescents’ self-esteem can be reduced [11]. Studies have shown that puberty, if ignored, has an adverse impact on adolescents’ self-esteem and emotional regulation. Therefore, teaching puberty-related issues and increasing adolescents’ knowledge in this field is very important for their self-esteem and positive emotional regulation [24]. Alimohammadi et al. showed that multimedia-based puberty health education could increase the self-esteem of adolescent boys [13]. Ning examined the effects of puberty mental health education and stated that the education could solve various psychological problems through emotional communication, emotional guidance and other activities [25]. In line with the present study, a qualitative study from Iran showed that most adolescent girls needed education on how to address issues related to puberty, as puberty was an unpleasant experience for them [10] which can cause psychological stress and reduce adolescents’ emotion regulation and self-esteem.
In the present study, in addition to education about physical and psychological changes during puberty and the strategies to cope with them, the religious rules during puberty and menstruation were taught to the girls, since the studies in Iran have shown that the lack of knowledge of religious rules has an adverse effect on the psychological well-being of adolescent girls [10]. However, the effect of the puberty-related religious rules education on emotion regulation and self-esteem of the girls was not examined separately. It is recommended that the effect of the knowledge and practice regarding puberty-related religious rules be assessed on these variables, especially in Islamic countries where these rules are mandatory.
This is the first study that assesses the effectiveness of multimedia-based puberty health education on self-esteem and emotion regulation of adolescent girls in Iran. One of the limitations of this study was the use of virtual education, which may have affected the quality of teaching and the attendance of adolescents. However, the educational topics were interesting for participants due to the lack of a reliable source of information, which motivated them to participate actively in the sessions. Also, this teaching method eliminates the feeling of shame for asking questions about body parts and puberty that may exist in face-to-face education. Another limitation was that some families prevented the girls’ participation in the training sessions despite their initial informed consent.
The knowledge and practice of puberty health can predict better emotion regulation and self-esteem in adolescent girls. The findings in this study confirm the importance of puberty health education for adolescent girls, especially in Iran, due to the lack of a reliable information source and their shame in seeking the information because of cultural norms. Therefore, health professionals and planners should be aware of and develop puberty health educational programs for improving adolescent girls’ physical and psychological health. This can provide appropriate guidance to foster a healthier lifestyle in girls, particularly those at risk. Further studies are needed to explore the risk and protective factors that can mediate or moderate the adverse developmental problems before implementing educational interventions that are more suitable for local/social contexts.
Ethical Considerations
Compliance with ethical guidelines
The girls and their parents were informed about the study objectives and were free to leave the study anytime. They signed a consent form to participate in the study. The study was conducted according to the principles outlined in the Declaration of Helsinki and approved by the Ethics Committee of the Islamic Azad University, Arak Branch, Arak, Iran (Code: IR.IAU.ARAK.REC.1401.007).
Funding
This study was extracted from a master’s thesis, approved by the Islamic Azad University, Arak Branch, Arak, Iran.
Authors' contributions
Project administration, and writing: Maryam Moridi; Data collection: Fatemeh Mirbagheri and Fatemeh Heidari; Study design, statistical analysis, literature review and final approval: All authors.
Conflict of interest
The authors declared no conflict of interests
Acknowledgments
The authors would like to thank the adolescent girls, their parents, and schools for cooperating in this study.
References
- WHO. Mental health of adolescents. Geneva: WHO; 2021. [Link]
- Moridi M, Amin Shokravi F, Ahmadi F. The paradox of acceptance: A content analysis of Iranian married female adolescent in confronting pregnancy. Plos One. 2019; 14(5):e0216649. [DOI:10.1371/journal.pone.0216649] [PMID]
- Wells AE, Hunnikin LM, Ash DP, Van Goozen SH. Low self-esteem and impairments in emotion recognition predict behavioural problems in children. J Psychopathol Behav Assess. 2020; 42:693-701. [Link]
- Peña-Sarrionandia A, Mikolajczak M, Gross JJ. Integrating emotion regulation and emotional intelligence traditions: A meta-analysis. Front Psychol. 2015; 6:160. [DOI:10.3389/fpsyg.2015.00160] [PMID]
- Bailen NH, Green LM, Thompson RJ. Understanding emotion in adolescents: A review of emotional frequency, intensity, instability, and clarity. Emot Rev. 2019; 11(1):63-73. [DOI:10.1177/1754073918768878]
- Sowislo JF, Orth U. Does low self-esteem predict depression and anxiety? A meta-analysis of longitudinal studies. Psychol Bull. 2013; 139(1):213-40 [DOI:10.1037/a0028931] [PMID]
- Brandt L, Liu S, Heim C, Heinz A. The effects of social isolation stress and discrimination on mental health. Transl Psychiatry. 2022; 12(1):398. [DOI:10.1038/s41398-022-02178-4] [PMID]
- Paulus FW, Ohmann S, Möhler E, Plener P, Popow C. Emotional dysregulation in children and adolescents with psychiatric disorders. A narrative review. Front Psychiatry. 2021; 12:628252. [DOI:10.3389/fpsyt.2021.628252] [PMID]
- Charles Shapu R, Ismail S, Ahmad N, Lim PY, Abubakar Njodi I. Systematic Review: Effect of health education intervention on improving knowledge, attitudes and practices of adolescents on malnutrition. Nutrients. 2020; 12(8):2426. [DOI:10.3390/nu12082426] [PMID]
- Golchin NA, Hamzehgardeshi Z, Fakhri M, Hamzehgardeshi L. The experience of puberty in Iranian adolescent girls: A qualitative content analysis. BMC Public Health. 2012; 12:698. [DOI:10.1186/1471-2458-12-698] [PMID]
- Hulme Chambers A, Tomnay J, Clune S, Roberts S. Sexuality education delivery in Australian regional secondary schools: A qualitative case study. Health Educ J. 2017; 76(4): 467-78. [DOI:10.1177/00178969176917]
- Khaleghi M, Shokravi FA, Peyman N, Moridi M. Evaluating the effect of educational interventions on health literacy through social networking services to promote students’ quality of life. Korean J Fam Med. 2019; 40(3):188-93. [DOI:10.4082/kjfm.18.0060] [PMID]
- Alimohammadi M, Neisani Samani L, Khanjari S, Haghani H. The Effects of Multimedia-Based Puberty Health Education on Male Students' Self-Esteem in the Middle School. Int J Community Based Nurs Midwifery. 2019; 7(2):109-17. [PMID]
- Preece DA, Becerra R, Robinson K, Gross JJ. The Emotion Regulation Questionnaire: Psychometric properties in general community samples. J Pers Assess. 2020; 102(3):348-56. [DOI:10.1080/00223891.2018.1564319] [PMID]
- Khorsand Khatibani S, Khosrojavid M, Abolghasemi A. [Predicting Bullying based on personality traits, cognitive emotion regulation and distress tolerance in students (Persian)]. J Mod Psychol Res. 2021; 15(60):131-48. [Link]
- Coopersmith S. Coopersmith self-esteem inventories. 1981. [DOI:10.1037/t06456-000]
- Soliemanifar O, Shaabani F, Rezaei Z, Nikoubakht N. [Disposition toward critical thinking, self-esteem, assertiveness, social anxiety and worry in students: A causal model (Persian)]. Clin Psychol Pers. 2018; 15(2):155-66. [DOI:10.22070/cpap.2020.2825]
- Chandra-Mouli V, Patel SV. Mapping the knowledge and understanding of menarche, menstrual hygiene and menstrual health among adolescent girls in low- and middle-income countries. Reprod Health. 2017; 14(1):30. [DOI:10.1186/s12978-017-0293-6] [PMID]
- Zakaria M, Karim F, Mazumder S, Cheng F, Xu J. Knowledge on, Attitude towards, and Practice of Sexual and Reproductive Health among Older Adolescent Girls in Bangladesh: An Institution-Based Cross-Sectional Study. Int J Environ Res Public Health. 2020; 17(21):7720. [DOI:10.3390/ijerph17217720] [PMID]
- Sychareun V, Chaleunvong K, Essink DR, Phommavongsa P, Durham J. Menstruation practice among school and out-of-school adolescent girls, Lao PDR. Glob Health Action. 2020; 13(sup2):1785170. [DOI:10.1080/16549716.2020.1785170] [PMID]
- Bahari R, Amin Shokravi F, Anosheh M, Moridi M. Effect of a health education program on puberty knowledge among visually impaired female adolescent students. Med J Islam Repub Iran. 2021; 35:74. [DOI:10.47176/mjiri.35.74] [PMID]
- Borjigen A, Huang C, Liu M, Lu J, Peng H, Sapkota C, et al. Status and factors of menstrual knowledge, attitudes, behaviors and their correlation with psychological stress in adolescent girls. J Pediatr Adolesc Gynecol. 2019; 32(6):584-9. [DOI:10.1016/j.jpag.2019.08.007] [PMID]
- Aldao A, Nolen-Hoeksema S. Specificity of cognitive emotion regulation strategies: A transdiagnostic examination. Behav Res Ther. 2010; 48(10):974-83. [DOI:10.1016/j.brat.2010.06.002] [PMID]
- Wierenga LM, Bos MGN, Schreuders E, Vd Kamp F, Peper JS, Tamnes CK, et al. Unraveling age, puberty and testosterone effects on subcortical brain development across adolescence. Psychoneuroendocrinology. 2018; 91:105-14. [DOI:10.1016/j.psyneuen.2018.02.034] [PMID]
- Ning S. Analysis of the network mental health education. J EducTeach Soc Stud. 2020; 2:24. [Link]
Article Type : Research |
Subject:
General
Received: 2023/08/15 | Accepted: 2024/05/8 | Published: 2025/01/12
Received: 2023/08/15 | Accepted: 2024/05/8 | Published: 2025/01/12
Send email to the article author
| Rights and permissions | |
 | This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
