Wed, Jan 28, 2026
Volume 36, Issue 1 (1-2026)
JHNM 2026, 36(1): 1-8 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Tunthanathip S, Laeheem K. Predictive Factors of Safe Sexual Behaviors among Adolescents in Thailand. JHNM 2026; 36 (1) :1-8
URL: http://hnmj.gums.ac.ir/article-1-2144-en.html
URL: http://hnmj.gums.ac.ir/article-1-2144-en.html



1- PhD Candidate of Human and Social Development, Department of Human and Social Development, School of Liberal Arts, Prince of Songkla University, Hat Yai, Thailand.
2- Associate Professor, Department of Human and Social Development, School of Liberal Arts, Prince of Songkla University, Hat Yai, Thailand. ,kasetchai.la@gmail.com, kasetchai.la@psu.ac.th
2- Associate Professor, Department of Human and Social Development, School of Liberal Arts, Prince of Songkla University, Hat Yai, Thailand. ,
Full-Text [PDF 492 kb]
(56 Downloads)
| Abstract (HTML) (156 Views)
Full-Text: (10 Views)
Introduction
Sexually transmitted diseases (STDs) in adolescents have become an important public health concern due to socioeconomic and cultural changes. The increasing focus on the sexual health of adolescents is needed to assess their exposure to STDs. According to the Centers for Disease Control and Prevention (CDC), approximately 50% of new STD cases are between the ages of 15-24 [1]. Syphilis, gonorrhea, chlamydia, and trichomoniasis are the most common STDs currently. Therefore, the World Health Organization (WHO) established goals for a 90% decrease in syphilis and gonorrhea incidence between 2018 and 2030 [2]. Risky sexual behaviors can impair people’s health, particularly their sexual health, by increasing their susceptibility to STDs and unwanted pregnancy [2, 3]. A study in Brazil showed that the incidence of acquired syphilis increased significantly from 12.3 cases per 100,000 population in 2011 to 81.4 cases per 100,000 population in 2017 [3], while the incidence rate of active syphilis in Colombia was 300 cases per 100,000 population in 2016 [4]. According to Thai national data, the incidence of STDs decreased from 1985 to 2005 but gradually increased since 2005. Syphilis and gonorrhea were the most common STDs, with incidence rates of 8.2 and 15.8 cases per 100,000 population, respectively. The increased incidence of STDs can be related to decreased condom use and increased risky sexual practices [5]. Hence, it is necessary to identify risk factors to increase safe sexual behaviors.
Knowledge, attitude, and practice regarding condom use in adolescents are important. Anyanwu et al. surveyed the knowledge and attitude of adolescents in Nigeria regarding condom use and found that knowledge and attitude are essential factors for sexual preventive practice. A negative attitude towards the use of condoms increased the refusal of condom use. In addition, errors in using condoms were common because of a lack of knowledge of the correct use of condoms [6]. Nesidai et al. studied factors associated with condom use among undergraduate students aged 15-24 years in Kenya and found a significant relationship between condom use and general attitude [7]. Yosef et al. studied 453 college students in southwest Ethiopia and reported that knowledge of STDs was significantly associated with a positive attitude towards condom use [8]. A study on homosexual men in Songkhla Province, Thailand, found that 87.5% and 94.6% of all cases had good knowledge and positive attitudes, respectively, while 62.5% had good behavior in STD prevention [9]. Lack of STD counseling can lead to misunderstanding and poor perception of safe sexual behaviors in students and young adults. Cohen et al. used a short group discussion, a role-playing session, and multimedia presentation during group counseling to promote safe sex behaviors that could reduce the re-infection rate among males [10]. However, seeking sexual information and counseling in Thailand is challenging among different socioeconomic and cultural contexts due to STD/AIDS-related social stigma [11].
Based on the literature review, various factors associated with safe sexual behaviors include good knowledge, positive attitude, and counseling. An investigation is required to determine whether these factors are related to safe sexual practice in Thailand, where there are higher incidence rates of STDs. Therefore, the present study aimed to identify predictors of safe sexual behaviors or practices among adolescents in Songkhla Province, Thailand.
Materials and Methods
This is a cross-sectional survey study conducted from November 2022 to January 2023. The study population was adolescents aged 15-24 years from two schools and one college in Southern Thailand. The sample size was determined using Cochran formula [12]. Based on data from Ampawa [9], the proportion of perceived self-protection in sexual intercourse was 87.5%. Using this value and considering a 0.05 margin of error and a 95% confidence interval, the minimum required sample size was calculated to be 169. Participants were invited via email sent to two schools and one college in Songkla Province, each with more than 1,000 students. There were 260 responses from students, of whom 255 were accepted to participate in the study and complete the questionnaires. Participants were selected by using a convenience sampling method.
The data were collected by a self-administered questionnaire measuring safe sexual practice, with two sections. The first section surveyed the baseline characteristics of participants, and the second section measured knowledge, attitude, counseling, assessed by three specialist physicians. The knowledge subscale had two domains; the attitude subscale, three domains; and counseling subscale, two domains. Each item was rated on a scale from 0 to 5. The quantitative content validity of this questionnaire was assessed using the item-objective congruence index by three physicians, yielding a value of 0.936. In addition, the questionnaire was used in a pilot study to determine its internal consistency. The Cronbach’s α coefficient for the overall scale was obtained at 0.925. For the knowledge, attitude, and counselling subscales, it was 0.884, 0.855, and 0.959, respectively.
Continuous variables were described as frequencies (percentages), while the Mean±SD were used for continuous variables. The Pearson correlation test and linear regression analysis were used to identify the factors associated with safe sexual practices. P<0.05 was considered statistically significant. Statistical analyses were performed in R software, version 4.1.0.
Results
The baseline characteristics of the participants are shown in Table 1.
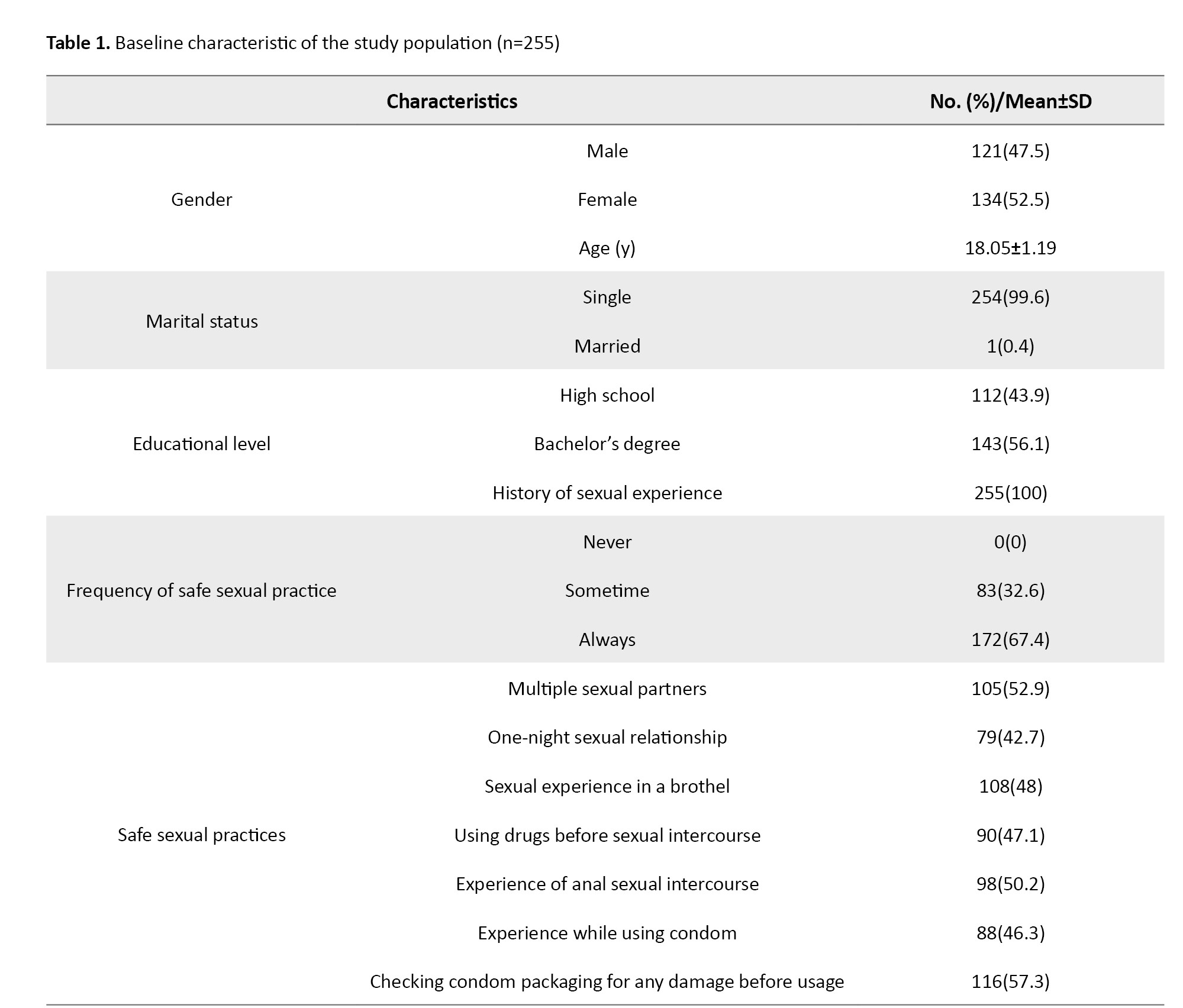
The mean age of the participants was 18.05±1.19 years. Among participants, 52.5% were female, and almost all were single. Also, 43.9% were high school students and 56.1% were college students. All of the participants had sexual experiences; 47.1% had multi-partner relationships, and 48.0% had experienced sexual intercourse in a brothel. In terms of safe sexual practice, 67.4% always had safe sexual behavior. In detail more than half had multiple sexual partners and 42.7% had experienced of one-night relationship. More than half of the participants had experienced anal sexual intercourse, while just 46.3% always used condom usage.
Mean scores of knowledge, attitude, and counseling domains for measuring safe sexual practices are shown in Table 2.
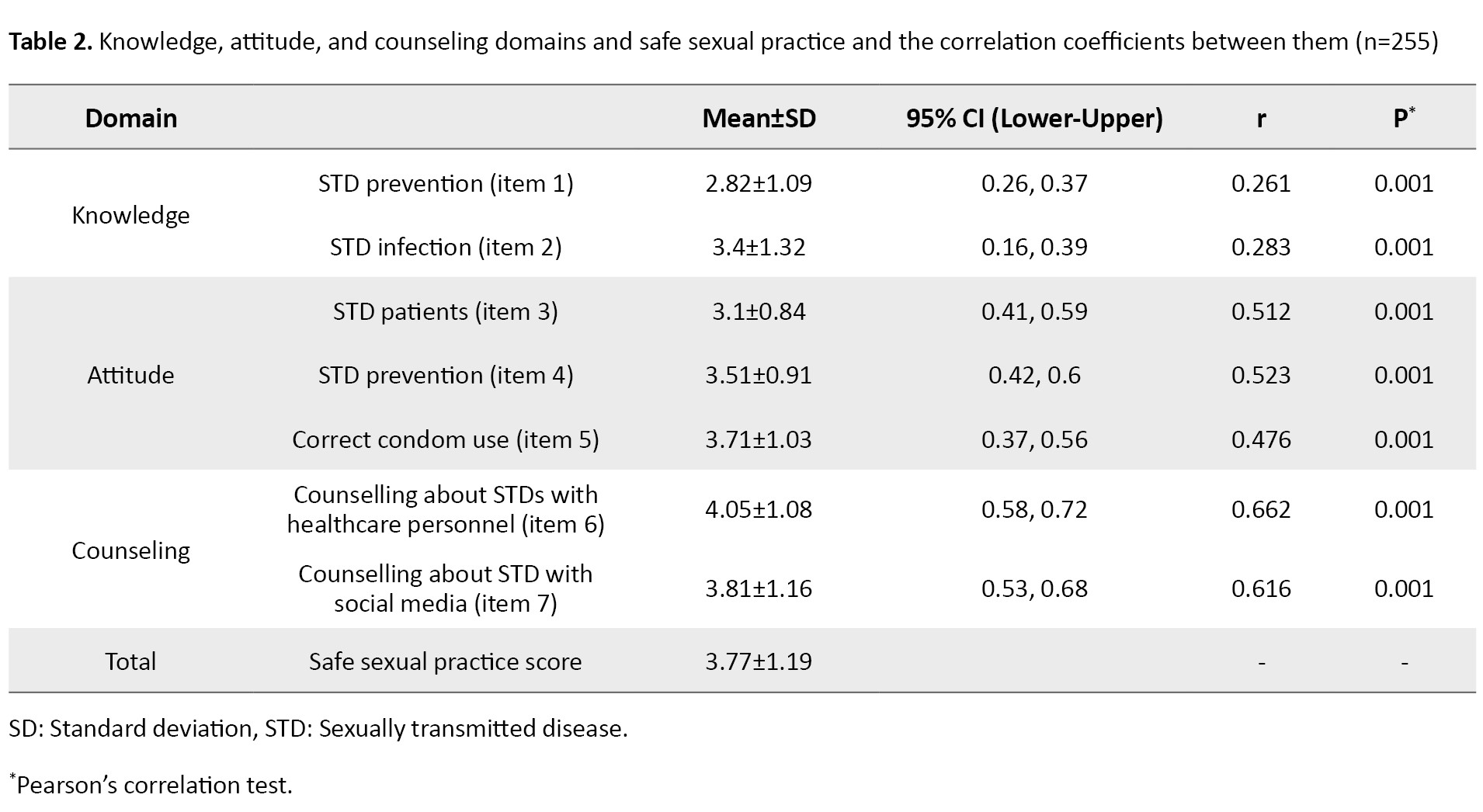
In the knowledge domain, the mean score of STD prevention was 2.82±1.09, whereas the STD infection score was 3.4±1.32. Mean scores of attitudes towards STD patients, STD prevention, and correct condom use were 3.1±0.84, 3.51±0.91, and 3.71±1.03, respectively. In the counseling domain, mean scores of counseling about STDs with healthcare personnel and social media were 4.05±1.08 and 3.81±1.16. The total safe sexual practice score was 3.77±1.19.
Pearson’s correlation coefficients for the relationship between demographic variables and the variables of knowledge, attitude, counseling, and safe sexual practice are shown in Table 3.
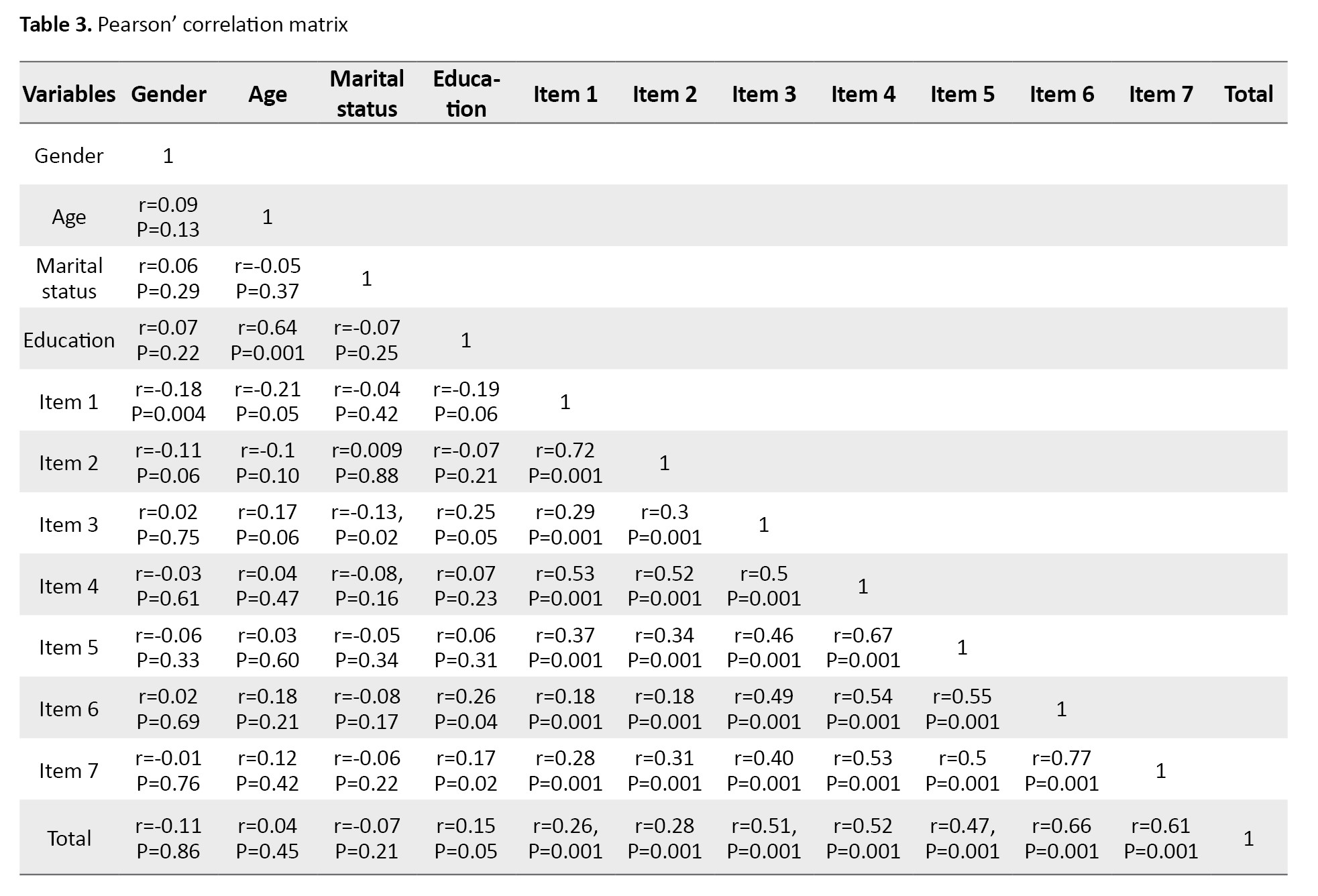
The knowledge domain score did not have a significant correlation with other variables, while scores of attitudes towards STD prevention (r=0.54, P=0.001) and attitudes towards correct condom use (r=0.55, P=0.001) were positively related with the score of counselling from healthcare personnel.
The results of linear regression analysis are shown in Table 4.
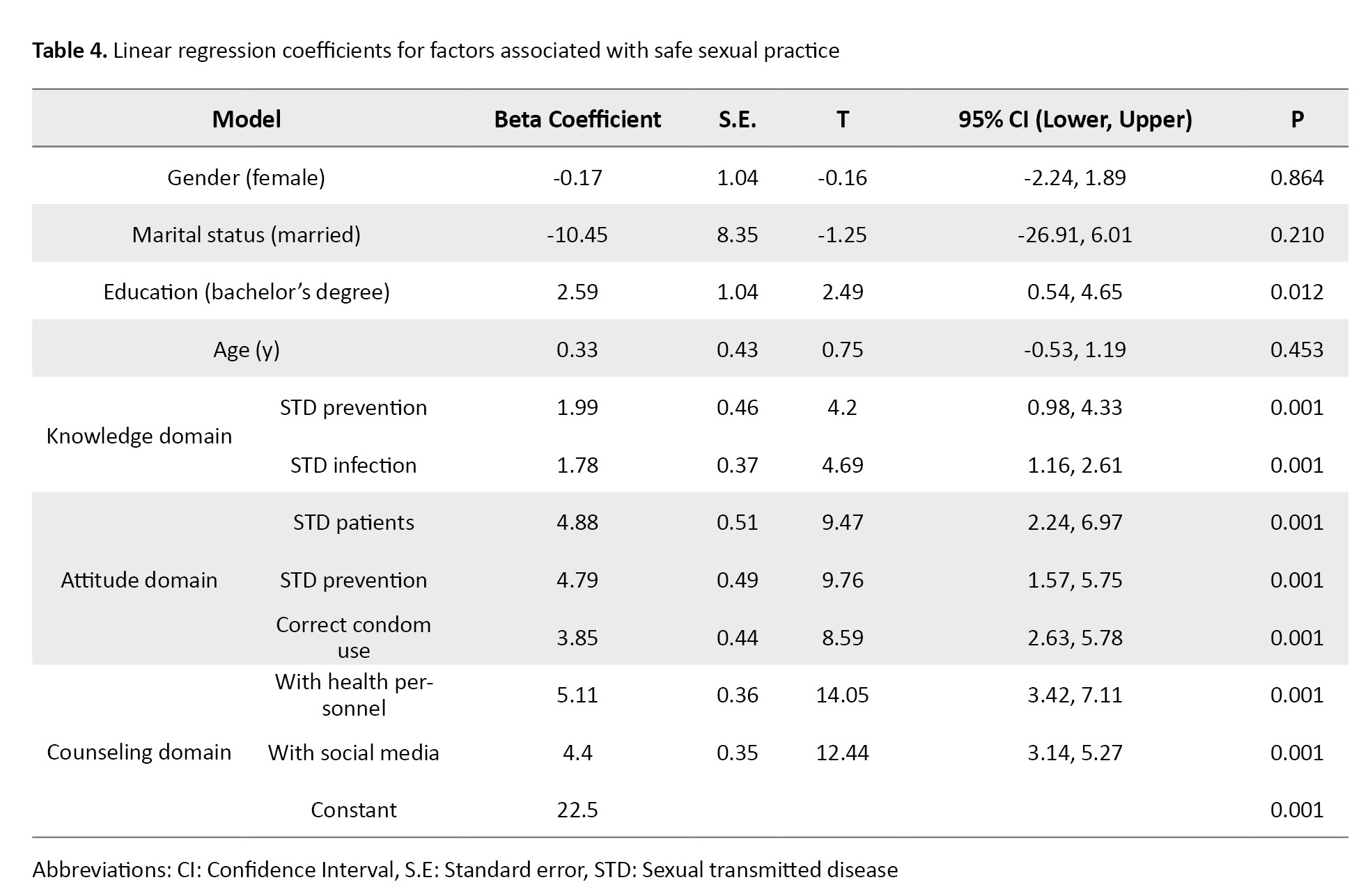
The knowledge, attitude, and counseling had significant association with safe sexual practice, while demographic data were not significantly associated with safe sexual practice scores. The knowledge of STD prevention (β=1.99, P=0.001) and STD infection (β=1.78, P=0.001); the attitude towards STD patients (β=4.88, P=0.001), STD prevention (β=4.79, P=0.001), and correct condom use (β=3.85, P=0.001); and counselling with healthcare personnel (β=5.11, P=0.001) and social media (β=4.4, P=0.001) had significant association with safe sexual practice. Therefore, these factors were included in the multiple regression model (Table 5).
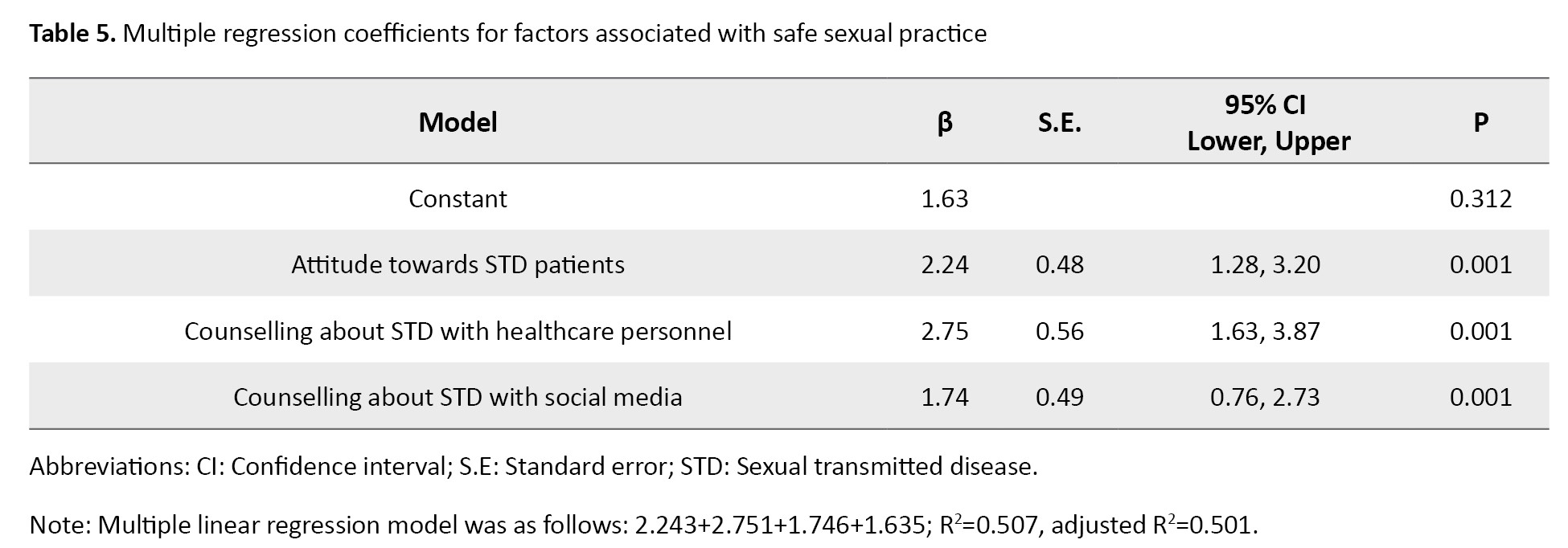
The attitude towards STD patients (β=2.24, 95% CI; 1.28%, 3.20%, P=0.001), counseling about STD with healthcare personnel (β=2.75, 95% CI; 1.63%, 3.87%, P=0.001), and counseling about STD with social media (β=1.74, 95% CI; 0.76%, 2.73%, P=0.001) were significant predictors of safe sexual practice.
Discussion
In the present study, it was found that attitudes towards STD patients, counseling about STDs with healthcare personnel, and receiving information/counseling about STDs from social media were significant positive predictors of STD prevention behaviors among Tai adolescents, which is consistent with the results of previous studies [5-8]. According to other studies, for identifying factors related to safe sexual practice among adolescents, their knowledge, attitude, and source of health information should be surveyed [5-11]. In our study, all three domains had a significant correlation with safe sexual practice, with the attitude and counseling domains showing greater correlation. Attitudes towards STD patients and counseling about STDs with healthcare personnel or receiving information from social media are important for having a safe sexual practice. Negative or positive attitudes can affect sexual practices. In the present study, clinical features and presentation of STDs can strongly affect the attitude of adolescents towards using a condom to have safe sex behaviors, since STD patients suffer from symptoms and social stigma. Nesidai et al. [7] surveyed adolescents in Kenya and found that a positive attitude towards condom use was associated with their use of condoms. In addition, knowledge, information/counseling of STDs and safe sexual behaviors were reported to be associated with safe sexual practice [6, 8].
The present study found risky sexual behaviors, which highlight the issue of sexual health among Tai adolescents. These results are similar to those reported in previous studies [13-15]. The rate of high-risk sexual behaviors in our study is close to that in previous studies conducted in Thailand. Somrongthong et al. studied sexual behaviors among teenagers in Bangkok and found that two-thirds of the adolescents engaged in unprotected sexual intercourse because they believed that having sexual intercourse with a partner was acceptable [16]. More than half of the participants in our study had multiple sexual partners. These findings are comparable with those of prior studies, which showed a rise in having multiple sexual partners [17, 18]. This can be explained by changes in social culture and current sexual norms across several countries [18, 19].
Providing information and counseling about STDs by parents, teachers, and healthcare personnel is challenged in Thailand due to cultural and social stigma. Tipwareerom et al. [20] studied condom usage among high school students through interviews and found that more than half of parents disagreed with placing condom vending machines in schools to inform the correct condom usage because high school students were too young to learn sexual topics. They perceived that counseling about the proper condom usage can promote students’ sexual experiences [20, 21]. Besides counseling with health personnel, the present study found that receiving information from social media had a high impact on adolescents’ safe sexual behaviors, which is in agreement with those of previous studies. Muanjan et al. studied social media addiction among high school students in Thailand and found that 15.7% of students were completely addicted to social media, while 51.3% were almost addicted regarding the use of social media, most of them used Instagram and Facebook 5.29 hours on weekday and 8.38 hours on weekend [22].When Thai adolescents’ behavior is influenced by social media, positive information and counseling about sexual problems may be one of the ways to inform them about the safety of sexual behaviors. Narkarat et al. presented a social media model to improve sexual health literacy among female students and reported that the intervention group’s average sexual health literacy score increased significantly compared to the control group [23]. Burns et al. conducted in-depth group interviews with African American adolescents regarding condom use and social media preferences. They reported that social media was predominantly utilized for the following purposes: Education, entertainment, browsing the site, self-expression, maintaining or seeking out relationships with family and friends, and social justice [24]. Condom-use education on social media platforms can be engaging if delivered by a well-known community member or a celebrity [25, 26]. In the future, it will be challenging to educate adolescents about safety in sexual relations via social media [25, 26].
In conclusion, attitude and counseling can predict safe sexual behavior among adolescents. However, this study had some limitations. We used a cross-sectional design over 3 months. By extending the duration and increasing the number of samples from other regions of Thailand and institutions, it is possible to obtain more information from adolescents. Further study should be conducted to improve safe sexual practices among Thai adolescents. Moreover, challenges of sexual health education and counseling for adolescents via social media platforms should be investigated.
Ethical Considerations
Compliance with ethical guidelines
The study was approved by the Ethics Review Committee of the Faculty of Nursing, Prince of Songkla University, Hat Yai, Thailand (Code: PSU IRB 2020-PSU-st010). The study objectives and methods were explained to the participants, and their written informed consent was obtained. All ethical principles were observed throughout the study.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for profit sectors.
Authors' contributions
Conceptualization, study design, review and editing: All authors: Data collection: Kasetchai Laeheem; Participant recruitment, data curation, data analysis, and initial draft preparation: Sopista Tunthanathip; Project administration: Kasetchai Laeheem.
Conflict of interest
The authors declare no conflict of interest.
Acknowledgments
The authors would like to thank the patients who participated in the research for their cooperation.
Sexually transmitted diseases (STDs) in adolescents have become an important public health concern due to socioeconomic and cultural changes. The increasing focus on the sexual health of adolescents is needed to assess their exposure to STDs. According to the Centers for Disease Control and Prevention (CDC), approximately 50% of new STD cases are between the ages of 15-24 [1]. Syphilis, gonorrhea, chlamydia, and trichomoniasis are the most common STDs currently. Therefore, the World Health Organization (WHO) established goals for a 90% decrease in syphilis and gonorrhea incidence between 2018 and 2030 [2]. Risky sexual behaviors can impair people’s health, particularly their sexual health, by increasing their susceptibility to STDs and unwanted pregnancy [2, 3]. A study in Brazil showed that the incidence of acquired syphilis increased significantly from 12.3 cases per 100,000 population in 2011 to 81.4 cases per 100,000 population in 2017 [3], while the incidence rate of active syphilis in Colombia was 300 cases per 100,000 population in 2016 [4]. According to Thai national data, the incidence of STDs decreased from 1985 to 2005 but gradually increased since 2005. Syphilis and gonorrhea were the most common STDs, with incidence rates of 8.2 and 15.8 cases per 100,000 population, respectively. The increased incidence of STDs can be related to decreased condom use and increased risky sexual practices [5]. Hence, it is necessary to identify risk factors to increase safe sexual behaviors.
Knowledge, attitude, and practice regarding condom use in adolescents are important. Anyanwu et al. surveyed the knowledge and attitude of adolescents in Nigeria regarding condom use and found that knowledge and attitude are essential factors for sexual preventive practice. A negative attitude towards the use of condoms increased the refusal of condom use. In addition, errors in using condoms were common because of a lack of knowledge of the correct use of condoms [6]. Nesidai et al. studied factors associated with condom use among undergraduate students aged 15-24 years in Kenya and found a significant relationship between condom use and general attitude [7]. Yosef et al. studied 453 college students in southwest Ethiopia and reported that knowledge of STDs was significantly associated with a positive attitude towards condom use [8]. A study on homosexual men in Songkhla Province, Thailand, found that 87.5% and 94.6% of all cases had good knowledge and positive attitudes, respectively, while 62.5% had good behavior in STD prevention [9]. Lack of STD counseling can lead to misunderstanding and poor perception of safe sexual behaviors in students and young adults. Cohen et al. used a short group discussion, a role-playing session, and multimedia presentation during group counseling to promote safe sex behaviors that could reduce the re-infection rate among males [10]. However, seeking sexual information and counseling in Thailand is challenging among different socioeconomic and cultural contexts due to STD/AIDS-related social stigma [11].
Based on the literature review, various factors associated with safe sexual behaviors include good knowledge, positive attitude, and counseling. An investigation is required to determine whether these factors are related to safe sexual practice in Thailand, where there are higher incidence rates of STDs. Therefore, the present study aimed to identify predictors of safe sexual behaviors or practices among adolescents in Songkhla Province, Thailand.
Materials and Methods
This is a cross-sectional survey study conducted from November 2022 to January 2023. The study population was adolescents aged 15-24 years from two schools and one college in Southern Thailand. The sample size was determined using Cochran formula [12]. Based on data from Ampawa [9], the proportion of perceived self-protection in sexual intercourse was 87.5%. Using this value and considering a 0.05 margin of error and a 95% confidence interval, the minimum required sample size was calculated to be 169. Participants were invited via email sent to two schools and one college in Songkla Province, each with more than 1,000 students. There were 260 responses from students, of whom 255 were accepted to participate in the study and complete the questionnaires. Participants were selected by using a convenience sampling method.
The data were collected by a self-administered questionnaire measuring safe sexual practice, with two sections. The first section surveyed the baseline characteristics of participants, and the second section measured knowledge, attitude, counseling, assessed by three specialist physicians. The knowledge subscale had two domains; the attitude subscale, three domains; and counseling subscale, two domains. Each item was rated on a scale from 0 to 5. The quantitative content validity of this questionnaire was assessed using the item-objective congruence index by three physicians, yielding a value of 0.936. In addition, the questionnaire was used in a pilot study to determine its internal consistency. The Cronbach’s α coefficient for the overall scale was obtained at 0.925. For the knowledge, attitude, and counselling subscales, it was 0.884, 0.855, and 0.959, respectively.
Continuous variables were described as frequencies (percentages), while the Mean±SD were used for continuous variables. The Pearson correlation test and linear regression analysis were used to identify the factors associated with safe sexual practices. P<0.05 was considered statistically significant. Statistical analyses were performed in R software, version 4.1.0.
Results
The baseline characteristics of the participants are shown in Table 1.
The mean age of the participants was 18.05±1.19 years. Among participants, 52.5% were female, and almost all were single. Also, 43.9% were high school students and 56.1% were college students. All of the participants had sexual experiences; 47.1% had multi-partner relationships, and 48.0% had experienced sexual intercourse in a brothel. In terms of safe sexual practice, 67.4% always had safe sexual behavior. In detail more than half had multiple sexual partners and 42.7% had experienced of one-night relationship. More than half of the participants had experienced anal sexual intercourse, while just 46.3% always used condom usage.
Mean scores of knowledge, attitude, and counseling domains for measuring safe sexual practices are shown in Table 2.
In the knowledge domain, the mean score of STD prevention was 2.82±1.09, whereas the STD infection score was 3.4±1.32. Mean scores of attitudes towards STD patients, STD prevention, and correct condom use were 3.1±0.84, 3.51±0.91, and 3.71±1.03, respectively. In the counseling domain, mean scores of counseling about STDs with healthcare personnel and social media were 4.05±1.08 and 3.81±1.16. The total safe sexual practice score was 3.77±1.19.
Pearson’s correlation coefficients for the relationship between demographic variables and the variables of knowledge, attitude, counseling, and safe sexual practice are shown in Table 3.
The knowledge domain score did not have a significant correlation with other variables, while scores of attitudes towards STD prevention (r=0.54, P=0.001) and attitudes towards correct condom use (r=0.55, P=0.001) were positively related with the score of counselling from healthcare personnel.
The results of linear regression analysis are shown in Table 4.
The knowledge, attitude, and counseling had significant association with safe sexual practice, while demographic data were not significantly associated with safe sexual practice scores. The knowledge of STD prevention (β=1.99, P=0.001) and STD infection (β=1.78, P=0.001); the attitude towards STD patients (β=4.88, P=0.001), STD prevention (β=4.79, P=0.001), and correct condom use (β=3.85, P=0.001); and counselling with healthcare personnel (β=5.11, P=0.001) and social media (β=4.4, P=0.001) had significant association with safe sexual practice. Therefore, these factors were included in the multiple regression model (Table 5).
The attitude towards STD patients (β=2.24, 95% CI; 1.28%, 3.20%, P=0.001), counseling about STD with healthcare personnel (β=2.75, 95% CI; 1.63%, 3.87%, P=0.001), and counseling about STD with social media (β=1.74, 95% CI; 0.76%, 2.73%, P=0.001) were significant predictors of safe sexual practice.
Discussion
In the present study, it was found that attitudes towards STD patients, counseling about STDs with healthcare personnel, and receiving information/counseling about STDs from social media were significant positive predictors of STD prevention behaviors among Tai adolescents, which is consistent with the results of previous studies [5-8]. According to other studies, for identifying factors related to safe sexual practice among adolescents, their knowledge, attitude, and source of health information should be surveyed [5-11]. In our study, all three domains had a significant correlation with safe sexual practice, with the attitude and counseling domains showing greater correlation. Attitudes towards STD patients and counseling about STDs with healthcare personnel or receiving information from social media are important for having a safe sexual practice. Negative or positive attitudes can affect sexual practices. In the present study, clinical features and presentation of STDs can strongly affect the attitude of adolescents towards using a condom to have safe sex behaviors, since STD patients suffer from symptoms and social stigma. Nesidai et al. [7] surveyed adolescents in Kenya and found that a positive attitude towards condom use was associated with their use of condoms. In addition, knowledge, information/counseling of STDs and safe sexual behaviors were reported to be associated with safe sexual practice [6, 8].
The present study found risky sexual behaviors, which highlight the issue of sexual health among Tai adolescents. These results are similar to those reported in previous studies [13-15]. The rate of high-risk sexual behaviors in our study is close to that in previous studies conducted in Thailand. Somrongthong et al. studied sexual behaviors among teenagers in Bangkok and found that two-thirds of the adolescents engaged in unprotected sexual intercourse because they believed that having sexual intercourse with a partner was acceptable [16]. More than half of the participants in our study had multiple sexual partners. These findings are comparable with those of prior studies, which showed a rise in having multiple sexual partners [17, 18]. This can be explained by changes in social culture and current sexual norms across several countries [18, 19].
Providing information and counseling about STDs by parents, teachers, and healthcare personnel is challenged in Thailand due to cultural and social stigma. Tipwareerom et al. [20] studied condom usage among high school students through interviews and found that more than half of parents disagreed with placing condom vending machines in schools to inform the correct condom usage because high school students were too young to learn sexual topics. They perceived that counseling about the proper condom usage can promote students’ sexual experiences [20, 21]. Besides counseling with health personnel, the present study found that receiving information from social media had a high impact on adolescents’ safe sexual behaviors, which is in agreement with those of previous studies. Muanjan et al. studied social media addiction among high school students in Thailand and found that 15.7% of students were completely addicted to social media, while 51.3% were almost addicted regarding the use of social media, most of them used Instagram and Facebook 5.29 hours on weekday and 8.38 hours on weekend [22].When Thai adolescents’ behavior is influenced by social media, positive information and counseling about sexual problems may be one of the ways to inform them about the safety of sexual behaviors. Narkarat et al. presented a social media model to improve sexual health literacy among female students and reported that the intervention group’s average sexual health literacy score increased significantly compared to the control group [23]. Burns et al. conducted in-depth group interviews with African American adolescents regarding condom use and social media preferences. They reported that social media was predominantly utilized for the following purposes: Education, entertainment, browsing the site, self-expression, maintaining or seeking out relationships with family and friends, and social justice [24]. Condom-use education on social media platforms can be engaging if delivered by a well-known community member or a celebrity [25, 26]. In the future, it will be challenging to educate adolescents about safety in sexual relations via social media [25, 26].
In conclusion, attitude and counseling can predict safe sexual behavior among adolescents. However, this study had some limitations. We used a cross-sectional design over 3 months. By extending the duration and increasing the number of samples from other regions of Thailand and institutions, it is possible to obtain more information from adolescents. Further study should be conducted to improve safe sexual practices among Thai adolescents. Moreover, challenges of sexual health education and counseling for adolescents via social media platforms should be investigated.
Ethical Considerations
Compliance with ethical guidelines
The study was approved by the Ethics Review Committee of the Faculty of Nursing, Prince of Songkla University, Hat Yai, Thailand (Code: PSU IRB 2020-PSU-st010). The study objectives and methods were explained to the participants, and their written informed consent was obtained. All ethical principles were observed throughout the study.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for profit sectors.
Authors' contributions
Conceptualization, study design, review and editing: All authors: Data collection: Kasetchai Laeheem; Participant recruitment, data curation, data analysis, and initial draft preparation: Sopista Tunthanathip; Project administration: Kasetchai Laeheem.
Conflict of interest
The authors declare no conflict of interest.
Acknowledgments
The authors would like to thank the patients who participated in the research for their cooperation.
Reference
- Centers for Disease Control and Prevention. Reported STDs reach all-time high for 6th consecutive year. Atlanta: Centers for Disease Control and Prevention; 2022. [Link]
- World Health Organization. Global Sexually Transmitted Infections Programme. Geneva: World Health Organization; 2022. [Link]
- Marques Dos Santos M, Lopes AKB, Roncalli AG, Lima KC. Trends of syphilis in Brazil: A growth portrait of the treponemic epidemic. PLoS One. 2020; 15(4):e0231029. [DOI:10.1371/journal.pone.0231029] [PMID]
- Korenromp EL, Ríos C, Apolinar ALS, Caicedo S, Cuellar D, Cárdenas I, et al. Prevalence and incidence estimates for syphilis, chlamydia, gonorrhea, and congenital syphilis in Colombia, 1995-2016. Rev Panam Salud Publica 2018; 42:e118. [DOI:10.26633/RPSP.2018.118] [PMID]
- Sharma M, Rewari BB, Aditama TY, Turlapati P, Dallabetta G, Steen R. Control of sexually transmitted infections and global elimination targets, South-East Asia Region. Bull World Health Organ. 2021; 99(4):304-11. [DOI:10.2471/BLT.20.254003] [PMID]
- Anyanwu PE, Fulton J. Knowledge and perception of young adults in Nigeria on effectiveness of condom use in prevention of sexually transmitted infections. Int J Adolesc Med Health. 2017; 29(2):1-3. [DOI:10.1515/ijamh-2015-0050] [PMID]
- Nesidai KBA, Ng’ang’a Z, Mwangi M, Wanzala P. Knowledge, Attitude and Practice factors associated with condom use among undergraduate Students of a Public University in Kenya. Afr J Health Sci.2011; 19:41-52. [Link]
- Yosef T, Nigussie T. Behavioral profiles and attitude toward condom use among college students in Southwest Ethiopia. Biomed Res Int. 2020; 2020:9582139. [DOI:10.1155/2020/9582139] [PMID]
- Ampawa P. Knowledge, understanding, and prevention behaviors regarding HIV infection and sexually transmitted diseases among men who have sex with men in Songkhla Province. Thai AIDS J. 2019; 31(1):21-31. [DOI:10.14456/taj.2019.3]
- Cohen DA, MacKinnon DP, Dent C, Mason HR, Sullivan E. Group counseling at STD clinics to promote use of condoms. Public Health Rep.1992; 107(6):727-31. [PMID]
- Logie CH, Newman PA, Weaver J, Roungkraphon S, Tepjan S. HIV-related stigma and HIV prevention uptake among young men who have sex with men and transgender women in Thailand. AIDS Patient Care STDS. 2016; 30(2):92-100. [DOI:10.1089/apc.2015.0197] [PMID]
- Thai Thanh Truc. Statistics and sample size pro [Internet]. 2013. [Updated 2023 Jun 21]. Available from: [Link]
- Hufstetler K, Llata E, Miele K, Quilter LAS. Clinical updates in sexually transmitted infections, 2024. J Womens Health (Larchmt). 2024; 33(6):827-37. [DOI:10.1089/jwh.2024.0367] [PMID]
- Siu WHS, Li PR, See LC. Rate of condom use among sexually active adolescents: a nationwide cross-sectional study in Taiwan from 2012 to 2016. BMJ Open. 2021; 11(8):e047727. [DOI:10.1136/bmjopen-2020-047727] [PMID]
- Wondimagegne YA, Anbese AT. Risky sexual behaviors and associated factors among adolescent in Gedeo Zone, South Ethiopia: A community based cross-sectional study. Sci Rep. 2024; 14(1):19908. [DOI:10.1038/s41598-024-67944-4] [PMID]
- Somrongthong R, Panuwatsuk P, Amarathithada D, Chaipayom O, Sitthi-amorn C. Sexual behaviors and opinions on sexuality of adolescents in a slum community in Bangkok. Southeast Asian J Trop Med Public Health. 2003; 34(2):443-6. [PMID]
- Zhou Y, Cheng F, Xu J. Religion, geography, and risky sexual behaviors among international immigrants living in China: Cross-sectional study. JMIR Public Health Surveill. 2024; 10:e44616. [DOI:10.2196/44616] [PMID]
- William DeShong MS, MA KA. Multiple sex partners, sexual networks, and condom use in Thailand. J Med Assoc Thai. 2018; 101:1686-96. [Link]
- Harris B, McCredie MN, Truong T, Regan T, Thompson CG, Leach W, et al. Relations between adolescent sensation seeking and risky sexual behaviors across sex, race, and age: A Meta-Analysis. Arch Sex Behav. 2023; 52(1):191-204. [DOI:10.1007/s10508-022-02384-7] [PMID]
- Tipwareerom W, Weglick L. Parents’ knowledge, attitudes, behaviors, and barriers to promoting condom use among their adolescent sons. Nurs Health Sci. 2017; 19(2):212-9. [DOI:10.1111/nhs.12331] [PMID]
- Andrzejewski J, Liddon N, Leonard S. Condom availability programs in schools: A review of the literature. Am J Health Promot. 2019; 33(3):457-67. [DOI:10.1177/0890117118791118] [PMID]
- Muanjan M. Tangwongchai S. Social media addiction and self-esteem of high school students in Hat Yai municipality, secondary educational service area office 16, Thailand. Chula Med J. 2022; 66(4):441-8. [DOI:10.58837/CHULA.CMJ.66.4.8]
- Narkarat P. Effect of social media model to improve sexual health literacy among secondary school female students in southern provinces, Thailand: a quasi experimental study [PhD dissertation]. Bangkok: Chulalongkorn University; 2022. [Link]
- Burns JC, Chakraborty S, Saint Arnault D. Social media preference and condom use behaviors: An analysis of digital spaces with young African American males. Health Educ Behav. 2021; 48(2):190-8. [DOI:10.1177/1090198121993043] [PMID]
- Escobar-Viera CG, Melcher EM, Miller RS, Whitfield DL, Jacobson-López D, Gordon JD, et al. A systematic review of the engagement with social media-delivered interventions for improving health outcomes among sexual and gender minorities. Internet Interv. 2021; 25:100428. [DOI:10.1016/j.invent.2021.100428] [PMID]
- Purba AK, Thomson RM, Henery PM, Pearce A, Henderson M, Katikireddi SV. Social media use and health risk behaviours in young people: Systematic review and meta-analysis. BMJ. 2023; 383:e073552. [DOI:10.1136/bmj-2022-073552] [PMID]
Article Type : Research |
Subject:
General
Received: 2023/05/1 | Accepted: 2024/02/24 | Published: 2026/01/11
Received: 2023/05/1 | Accepted: 2024/02/24 | Published: 2026/01/11
Send email to the article author
| Rights and permissions | |
 | This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
