Wed, Feb 4, 2026
Volume 35, Issue 3 (6-2025)
JHNM 2025, 35(3): 208-216 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Joseph J, Sequira L, christabel S. Knowledge, Symptoms, Quality of Life, and Health-seeking Behavior in Menopausal Nuns. JHNM 2025; 35 (3) :208-216
URL: http://hnmj.gums.ac.ir/article-1-2129-en.html
URL: http://hnmj.gums.ac.ir/article-1-2129-en.html



1- Nursing (MSc), M.Phil. (Nursing), MBAHCS. Vice Principal, Thiruhrudaya College of Nursing, Kerala, India.
2- Associate Professor, Manipal College of Nursing, Manipal Academy of Higher Education, Manipal, India. ,cliffleena@gmail.com
3- Assistant Professor- Senior scale, Manipal College of Nursing, Manipal Academy of Higher Education, Manipal, India.
2- Associate Professor, Manipal College of Nursing, Manipal Academy of Higher Education, Manipal, India. ,
3- Assistant Professor- Senior scale, Manipal College of Nursing, Manipal Academy of Higher Education, Manipal, India.
Full-Text [PDF 534 kb]
(203 Downloads)
| Abstract (HTML) (643 Views)
Full-Text: (169 Views)
Introduction
In women, menopause is the phase of ending of menstruation. Many women experience menopausal symptoms, which are not life-threatening but self-recovering. At the same time, it leads to vasomotor, somatic, sexual, and psychological symptoms that decrease the overall Quality of Life (QoL) of women [1]. The “menopausal transition” causes various bodily and mental changes for women. Many of them experience different symptoms, like irregular menstrual cycles, sleep disturbance, and vaginal dryness [2]. The association between menopause and menopausal symptoms appears transient, showing an increase in perimenopause and a compensatory decrease during the post-menopause [3].
Symptoms of menopause due to hormonal changes may greatly affect various organ systems, including the musculoskeletal and cardiovascular systems, affecting QoL [4]. A noticeable negative correlation to the QoL indicates symptoms for both users and nonusers of hormonal therapy, except for stress and frequency of symptoms for users [5]. A study on menopause showed a notable difference in vasomotor symptoms in the perimenopausal and postmenopausal groups. The prevalence of postmenopausal symptoms, health-seeking behavior, and associated factors were explored in postmenopausal women. The study shows a high range of physical and vasomotor symptoms. Most participants did not seek treatment for their problems [4]. The study reiterated the need for behavior change in communication toward healthcare practices [6]. An 8-week exercise program for postmenopausal women revealed an expressive decline in menopausal symptoms other than urogenital manifestations, and it was found that there was a powerful rise in lumbar strength and flexibility after 8 weeks of the Pilates exercise program [7].
Menopause is the edge of women’s reproducing action, but it proposes them to a new phase of life. The challenge is facilitated by the culture of silence that shrouds this phase. During menopause, women undergo many changes in their bodies. It can be taken in a positive or negative aspect. Many women are not aware of the symptoms that can occur and how they can be managed. Hence, teaching menopausal women about managing menopausal symptoms helps improve their QoL [1, 2].
Nuns often live in a unique cultural and social context. The study can explore the effectiveness of multimodal interventions, contributing to a more nuanced understanding of healthcare practices in this demographic. Our study findings can have implications for public health policies aimed at improving the health and well-being of nuns. It may guide the development of targeted interventions and support systems for this demographic. It provides valuable insights that can apply to nuns and other populations, contributing to advancing scientific understanding of women’s health. Multimodal interventions often involve a holistic approach, addressing physical, emotional, and spiritual aspects. The study may highlight the importance of comprehensive care, promoting empowerment and well-being among menopausal nuns. Thus, this study was done to assess the knowledge on menopause nuns, analyze the symptoms, understand the health-seeking behavior, describe the QoL, and evaluate the effect of multimodal intervention on the knowledge, symptoms, health-seeking behavior, and QoL among nuns at menopausal age.
Materials and Methods
This study used a quantitative experimental pre-test-post-test design. The present study assessed the knowledge, symptoms, health-seeking behavior, and QoL of nuns at menopausal age in 2020.
Kerala has 14 districts, and Kottayam District was selected using purposive sampling. There are 26 convents under St. Mathew’s Province in Kottayam District in India 20 were selected using the chit method. The St. Mathew’s Province consists of 437 sisters. An enumeration sampling technique was used to recruit women of menopausal age (nuns) residing in those selected convents. A pilot study was conducted in a subset of convents before the full-scale study, which allowed for the refinement of intervention protocols, assessment tools, and sampling strategies based on feedback from the pilot phase. The baseline characteristics such as health status, educational background, and previous exposure to menopause-related information can be used to assess the homogeneity or heterogeneity of the sample.
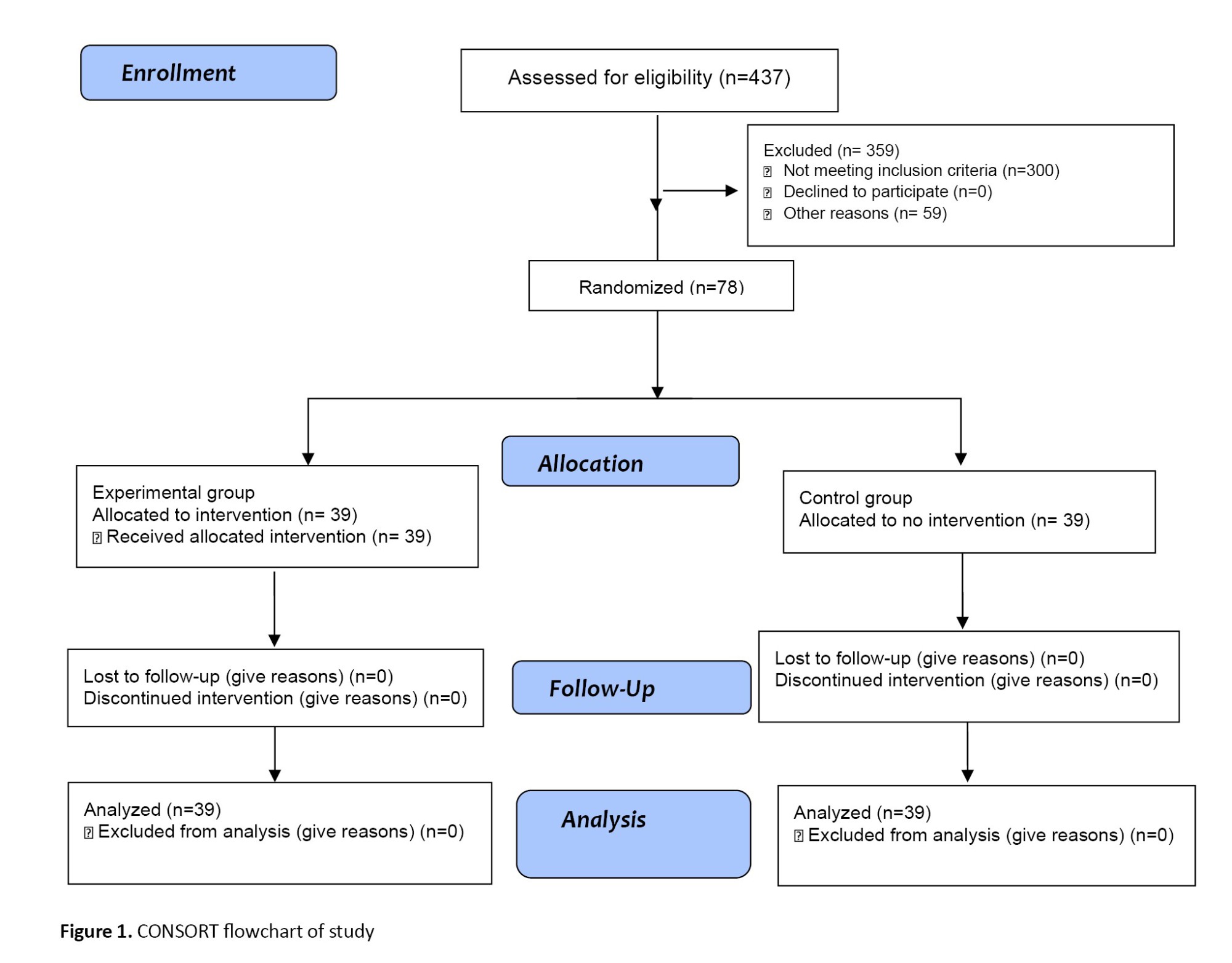
A total of 78 women of menopausal age who fulfilled the inclusion criteria (women in the menopausal period who are religious nuns) were selected. Women with serious medical illnesses like stroke and musculoskeletal problems were not included in the study. These respondents were divided into experimental and control groups. Accordingly, 39 subjects were designated to the experimental group, and the remaining 39 were treated as the control group. To facilitate the experiment’s smooth conducting, the experimental group was chosen from the first 10 convents and the control group from the remaining 10 (Figure 1). The sample size was calculated based on the findings of the pilot study.
The datasets include sociodemographic proforma. The tool consisted of age, educational status, occupation, information regarding menopause, attainment of menopause, and type of menopause. The structured knowledge questionnaire on menopause was developed based on definition, incidence, causes, physiology, symptoms, management, and complications. This tool’s validity (Content Validity Index [CVI]=0.747) and reliability (Intraclass Correlation [ICC]=0.877) were confirmed.
The menopausal symptoms were assessed using the modified menopause rating scale. It is a validated questionnaire comprising 25 items grouped into four categories: Vasomotor, psychosomatic, psychological, and urinary symptoms. Each item is a menopausal symptom, which is graded on a 4-point rating scale with a minimum score of 1 and a maximum of 4. The tool’s validity (CVI) and reliability (Cronbach α) were 0.876 and 0.877, respectively.
The QoL of menopausal-aged women is assessed by the modified 5-point Utian QoL (UQoL) scale [8]. The scale consists of 20 items and three domains: Occupation (7 items numbered 2, 3, 4, 14, 15, 16, 20), health (7 items numbered 5, 6, 7, 8, 13, 18, 19), emotional (6 items numbered 1, 9, 10, 11, 12, 17). Every item in the UQoL scale is scored using a 5-point Likert scale. The validity and reliability of the tool were 0.890 and 0.863, respectively.
The health-seeking behavior questionnaire had 9 questions that assessed the individuals in maintaining and improving their health and wellbeing. In the context of menopausal women, it could involve seeking medical advice, adopting healthy lifestyle practices, undergoing screenings, or following recommended healthcare guidelines. The approach involved using straightforward, dichotomous, and close-ended questions to gather specific and structured information about the health-seeking behavior of women in the menopausal age group. The minimum score was 0, and the maximum score was 9. The higher score is interpreted as good health-seeking behaviors.
Multimodal intervention includes a booklet on menopause and a video on pranayama and relaxation techniques. A booklet on menopause was given to the experimental group with a one-to-one teaching. The researcher demonstrated pranayama and relaxation techniques and a video to the participants. Instructed the participants to practice pranayama and relaxation techniques for 10 minutes daily for one month and to maintain a logbook. A post-test was conducted after one month to understand the effectiveness of multimodal interventions. After this, multimodal interventions were given to the control group as well.
The study was conducted among religious nuns who know how to read and write English. The participants were identified directly by the principal investigator. Written consent was obtained from the institution’s authority. Women at menopausal age who fulfilled the inclusion criteria were selected. Twenty institutions (convents) were chosen from the Kottayam District and divided into two groups of 10 each. Thirty-nine participants were selected from 10 convents and assigned as an experimental group; another 39 were selected from the other 10 convents and assigned as the control group. The researcher gave a self-introduction to the participants.
An explanation of the study and its confidentiality was provided. A pre-test on a structured knowledge questionnaire on menopause, a rating scale on symptoms experienced by women at menopausal age, a questionnaire on health-seeking behavior, and a modified Utian 5-point scale on QoL were administered to the experimental and control group, and the resulting data were collected. A booklet on menopause was given to the experimental group, and one-to-one teaching was given. The researcher underwent training on premenopausal exercise at the Punarjani School of Yoga. The researcher conducted one hour of training for the participants on pranayama and relaxation techniques, along with a video. Instructions were given to the participants on how to practice pranayama. Relaxation techniques of 10 minutes daily in the morning and evening for one month and maintaining a logbook are also included. The training was conducted at their respective convents. An information booklet on menopause was prepared for the participants by the researcher based on the literature review and suggestions from the experts. It briefly described the definition, incidence, causes, physiology, symptoms, management, and complications. A post-test was conducted after one month to understand the effectiveness of multimodal interventions, and the resulting data were collected.
Sample characteristics based on demographic variables, knowledge of menopause, menopausal symptoms, health-seeking behavior, and QoL among menopausal-age women were described using frequency and percentage. Effectiveness of multimodal intervention on knowledge, menopausal symptoms, and QoL assessed by Mann-Whitney U test. The association between knowledge, symptoms, and QoL among menopausal women was assessed by the chi-square test. The correlation between the score of symptoms and health-seeking behavior, QoL, and health-seeking behavior was evaluated using the Spearman rank correlation, and the Multivariate Analysis of covariance (Mancova) test was also used for the study.
Results
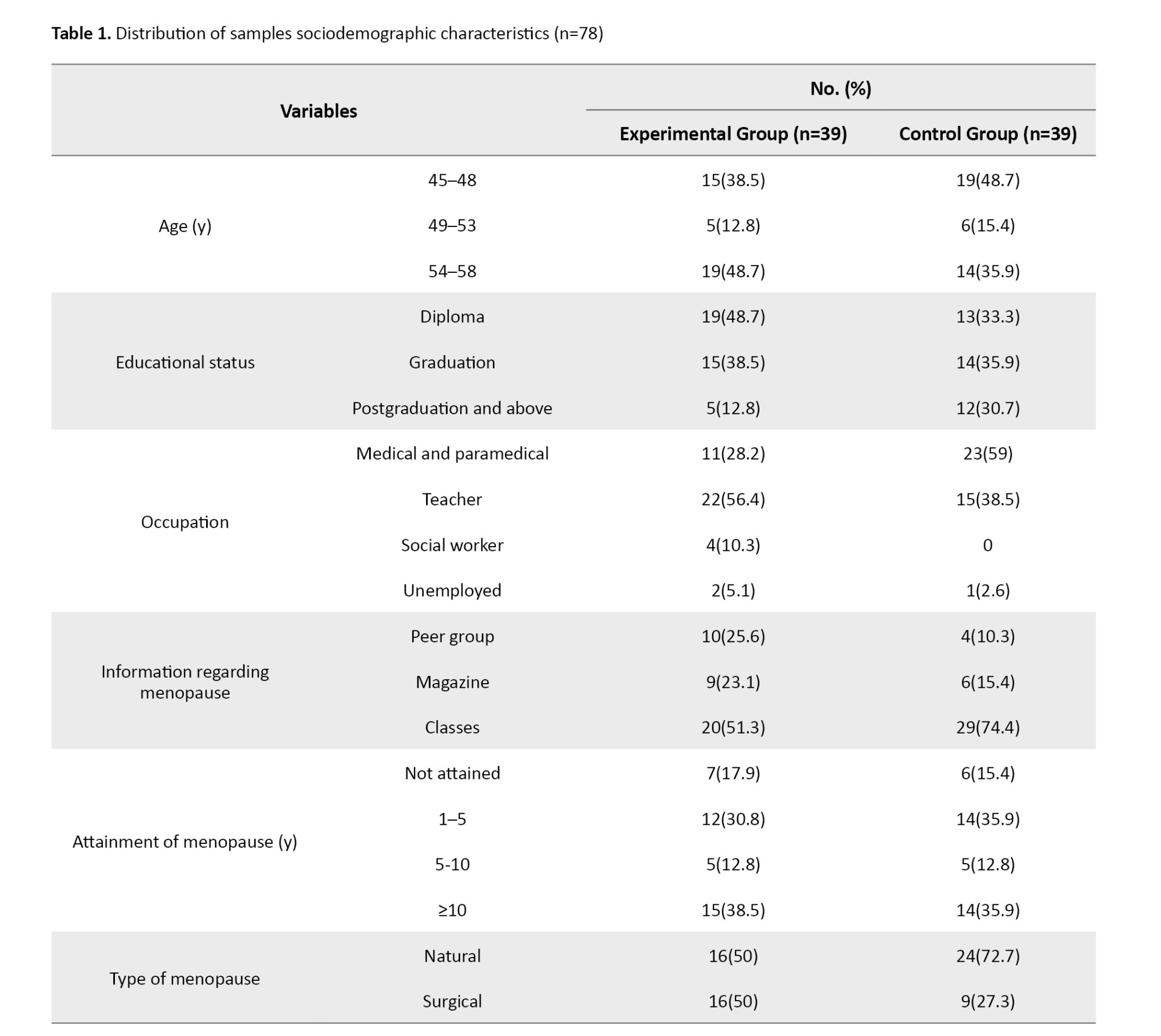
The study’s findings showed that most participants (48.7%) were 54-58 years in the experimental group and 45-48 years old in the control group (Table 1).
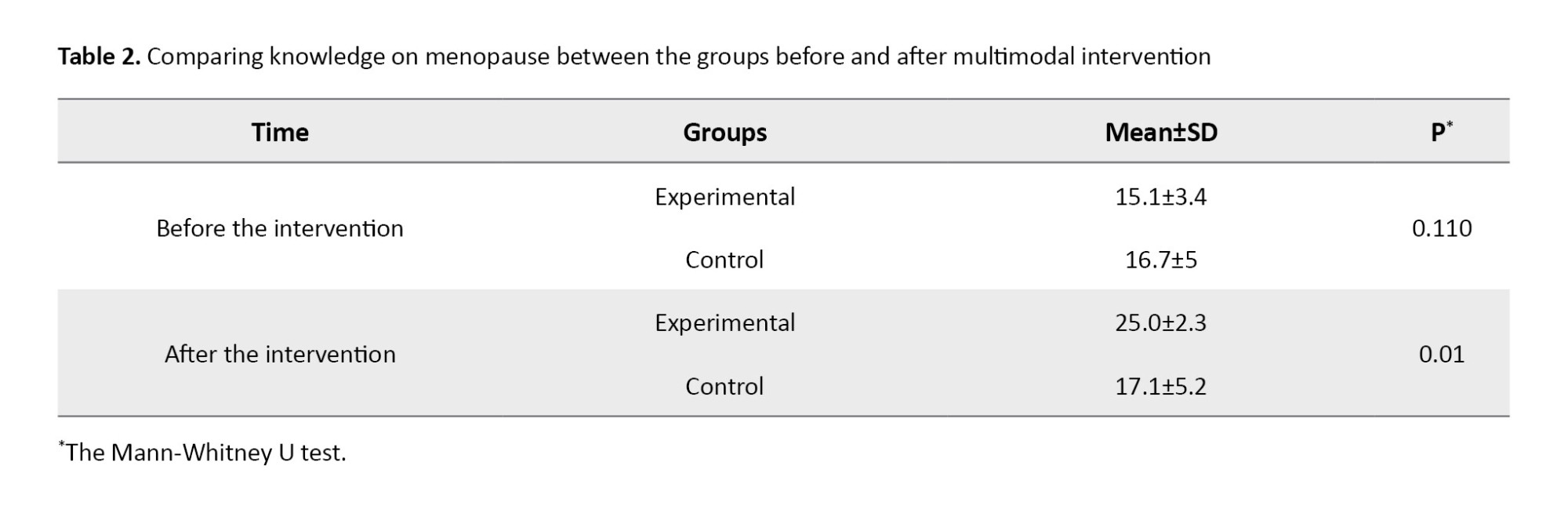
The comparison of knowledge on menopause groups before and after multimodal intervention revealed a significant change (P=0.01) between the knowledge scores of menopause women between the groups (Table 2).
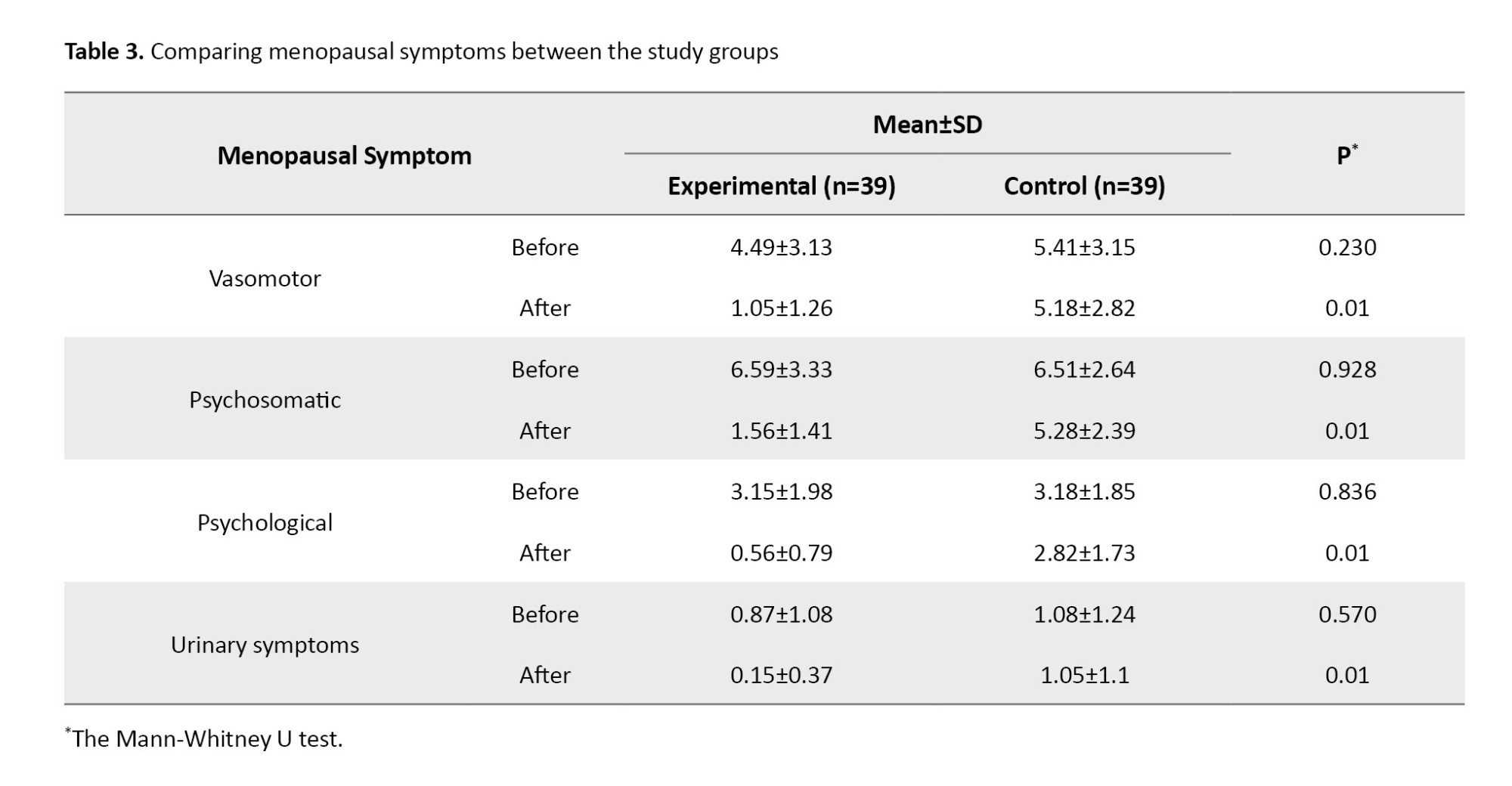
A comparison of menopausal symptoms between the groups shows a significant difference (P=0.01) in menopausal symptoms in the experimental group after the intervention (Table 3).
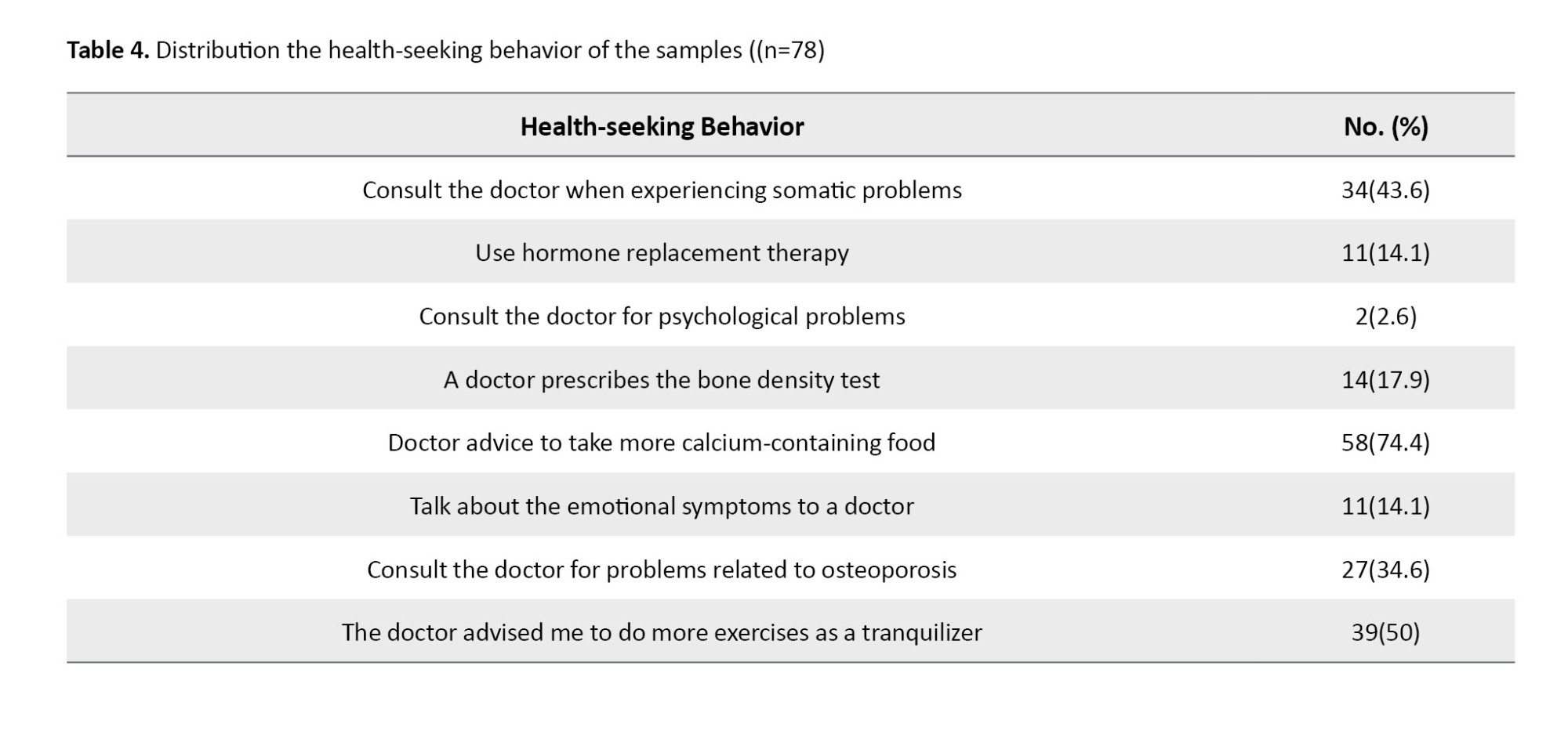
The distribution of women’s health-seeking behavior at menopause in two groups is given in Table 4. Based on this Table, the health-seeking behavior is most related to the phrases “doctor advised to take more calcium-containing food” (74.4%) and “doctor suggested to do more exercises as a tranquilizer” (50%).
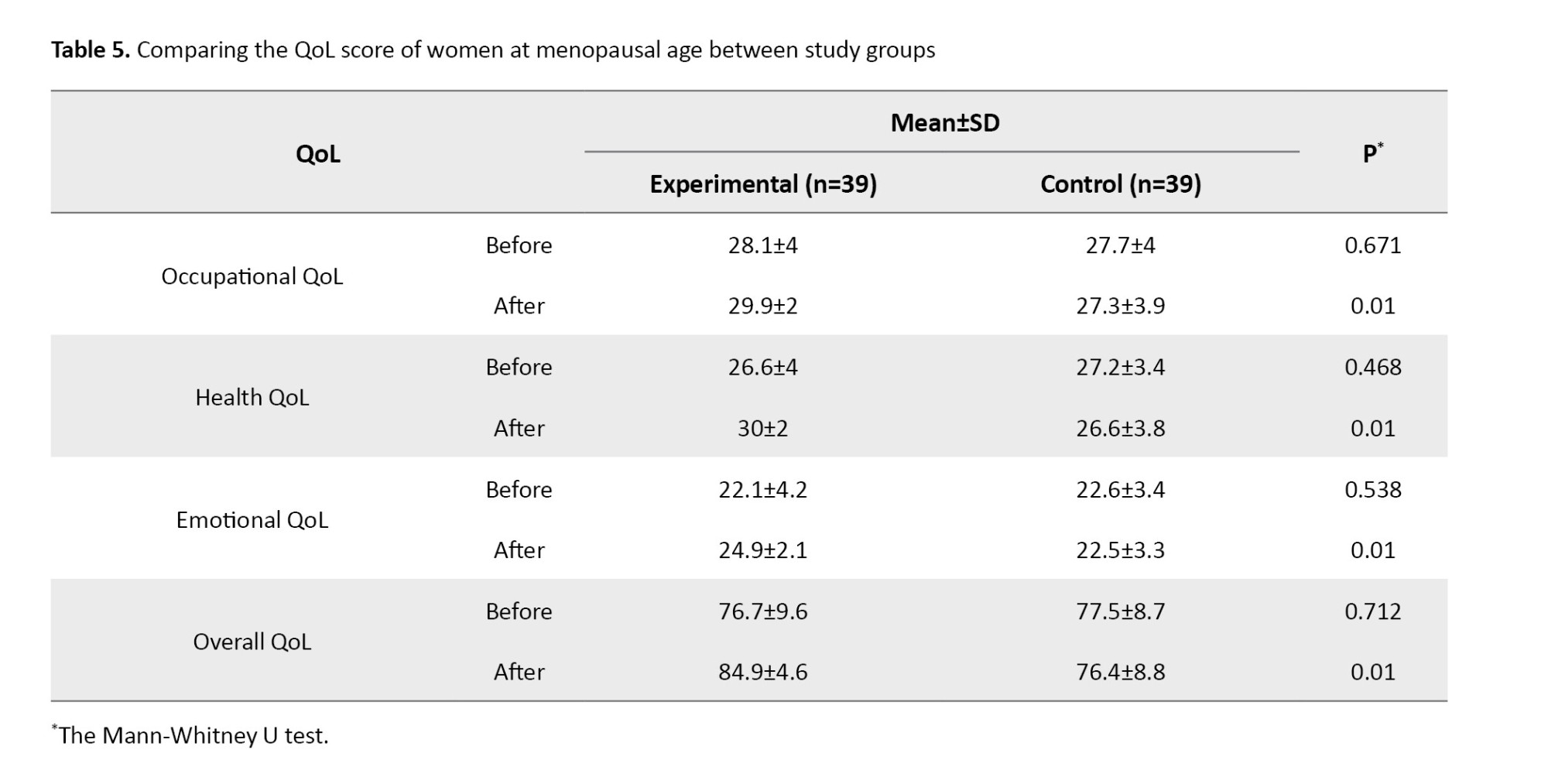
The QoL of women at menopausal age is shown in Table 5. It shows that intervention effectively improved the QoL of women at menopausal age, and the average QoL score in the two study groups after the intervention had a statistically significant difference based on the Mann-Whitney U test (P=0.01).
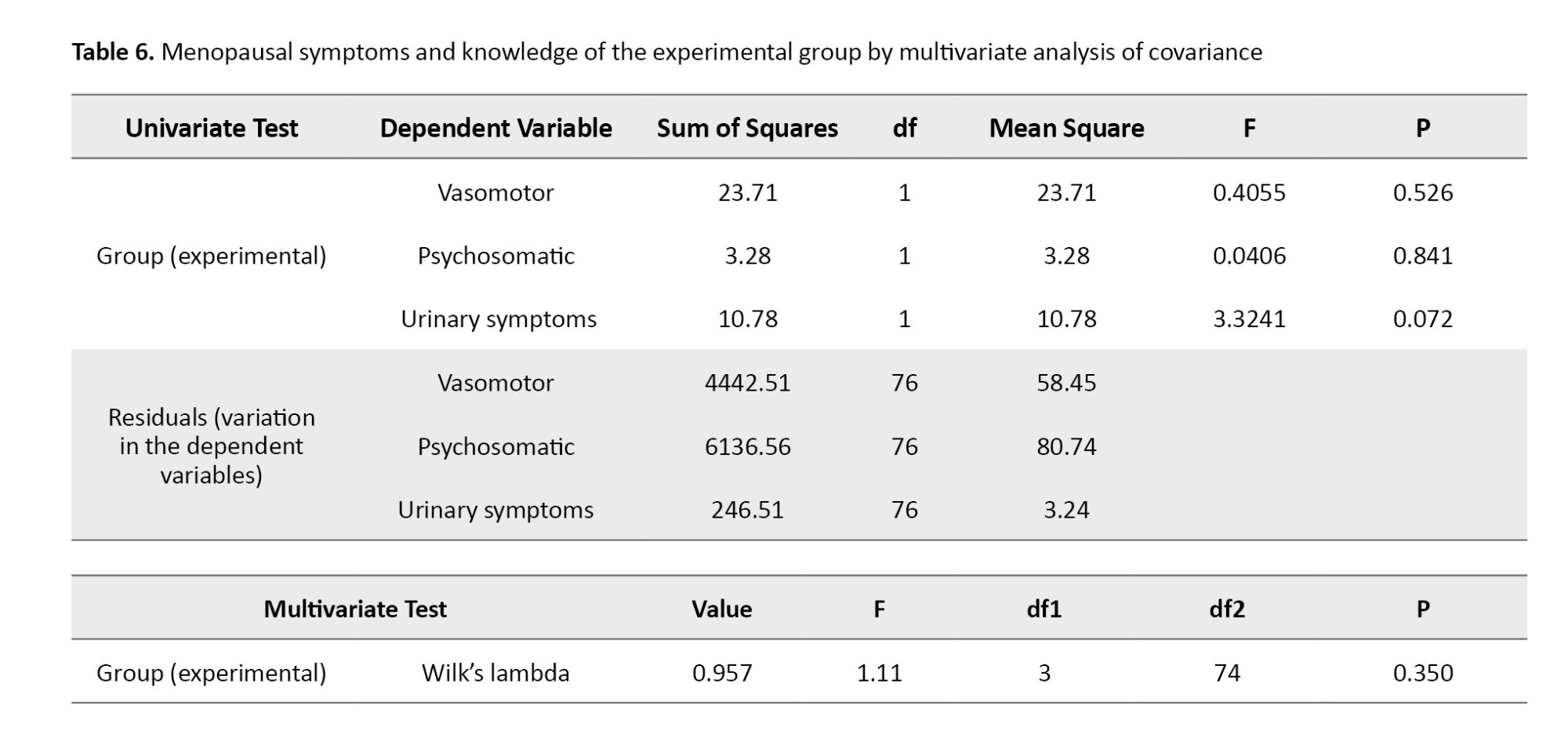
One-way MANCOVA was done with the respondents’ vasomotor, psychosomatic, and urinary symptoms as dependent variables and knowledge levels of the respondents versus low, moderate, and high as independent variables and their psychological core as a covariate. Since the P of Pillai’s Trace as per the multivariate test is <0.01, the null hypothesis is rejected at a 1% significance level. Hence, the respondents’ knowledge levels significantly influence their vasomotor, psychosomatic, and urinary symptoms (Table 6).
Similarly, the level of health and QoL of the respondents and the occupational level of the respondents significantly influence their vasomotor, psychosomatic, and urinary symptoms.
Discussion
The multimodal intervention was an effective strategy to increase the knowledge of women at menopausal age regarding menopause. The findings revealed reduced menopausal symptoms, improved QoL, and health-seeking behavior. A booklet on menopause, a video on pranayama, and relaxation techniques were the interventions provided to the participants. A positive result was seen in the knowledge, reduced symptoms, improved QoL, and health-seeking behavior.
A cluster randomized trial study was done in Iran among 68 women to assess the impact of multimedia intervention on the uncertainty about menopause. Implementing the education program helped improve knowledge and decrease uncertainty scores [9]. A quasi-experimental study among 99 middle-aged elementary, junior, and secondary teachers to determine the impact of health education on knowledge and attitude toward menopause. The multimodal intervention included lectures, leaflets, booklets, and group discussions. The study findings showed a significant increase in their knowledge and positive attitude towards menopause, which helped the women handle the symptoms of menopause [10]. A study in France on 5004 postmenopausal women shows that vaginal dryness and urinary urgency were the commonly reported symptoms and suggested the need for the education of the public through various educational programs [11]. Another study shows regular physical exercise intervention helps postmenopausal women to improve their vasomotor symptoms and overall wellbeing [12]. Multidisciplinary health education is effective in enhancing the menopausal syndrome and healthy lifestyle behavior of menopausal women [13], and the another study results show that the age of the women is not significantly correlated with QoL as the women did not find much difference in post menopause which contradict the present study [14].
According to the World Health Organization (WHO), menopausal symptoms can be managed with proper information. Researchers have emphasized that menopausal symptoms can be best handled by appropriate education, counseling, and symptom management. However, it is ineffective in practice because of the lack of proper resources and medical professionals [15]. Regarding the broad impact of social determinants of health on menopause, education and counseling are necessary to improve women’s attitudes towards menopause. Besides, improving emotional and social support, planning for lifestyle enhancement, and improving socioeconomic status are needed, which results in promoting women’s health during menopause [16]. Depression and urinary incontinence in menopausal women are related to each other, indicating the need for screening postmenopausal women with urinary incontinence and depression. Then, timely treatment and proper management can be given to improve their QoL [17].
Technological advancements such as music therapy are important in reducing menopausal symptoms. This therapy assists in achieving positive health outcomes by helping to alleviate issues during the menopausal period [18]. In the realm of menopausal women’s wellbeing, it is evident that they are frequently entangled in a web of physical symptoms and depressive states. This condition highlights the need for educational interventions, integrating cognitive behavioral therapy and tailored education addressing the physical aspects of menopausal transition. Therefore, it is necessary to develop and implement more comprehensive programs that consider lifestyle management and psychological support for menopausal women [19]. A balanced diet has a positive effect on the quality of sleep. Foods and meals containing sufficient protein, carbohydrates, and fats are also essential for good sleep quality. Scientific evidence indicates that good nutrition and quality sleep help maintain better health during menopause and perimenopause [20].
Based on the study results, intervention can be given to all menopausal women through mass media, drama, puppet shows, and role-play to improve knowledge, reduce menopausal symptoms, and improve the QoL.
The study was confined to a limited number of women at menopausal age and was organized in selected institutions, which limited the generalization of the study. A structured knowledge questionnaire was used for data collection, limiting the information that respondents could obtain.
The knowledge of women at menopausal age about menopause was low, and experience of menopausal symptoms was more. There is a need to educate menopausal women to improve their knowledge, reduce the symptoms experienced, and maintain a good QoL and health-seeking behavior.
Ethical Considerations
Compliance with ethical guidelines
The study was approved by the Kasturba Medical College and Kasturba Hospital Institutional Ethics Committee (Code: IEC 499/2020) and was registered at the Clinical Trial Registry of India (CTRI), New Delhi, India (Code: CTRI 2020/11/038529). Informed consent was acquired from all study participants.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
All authors contributed equally to the conception and design of the study, data collection and analysis, interception of the results and drafting of the manuscript. Each author approved the final version of the manuscript for submission.
Conflict of interest
All authors declared no conflict of interest.
Acknowledgments
The authors thank the research samples for their participation.
References
In women, menopause is the phase of ending of menstruation. Many women experience menopausal symptoms, which are not life-threatening but self-recovering. At the same time, it leads to vasomotor, somatic, sexual, and psychological symptoms that decrease the overall Quality of Life (QoL) of women [1]. The “menopausal transition” causes various bodily and mental changes for women. Many of them experience different symptoms, like irregular menstrual cycles, sleep disturbance, and vaginal dryness [2]. The association between menopause and menopausal symptoms appears transient, showing an increase in perimenopause and a compensatory decrease during the post-menopause [3].
Symptoms of menopause due to hormonal changes may greatly affect various organ systems, including the musculoskeletal and cardiovascular systems, affecting QoL [4]. A noticeable negative correlation to the QoL indicates symptoms for both users and nonusers of hormonal therapy, except for stress and frequency of symptoms for users [5]. A study on menopause showed a notable difference in vasomotor symptoms in the perimenopausal and postmenopausal groups. The prevalence of postmenopausal symptoms, health-seeking behavior, and associated factors were explored in postmenopausal women. The study shows a high range of physical and vasomotor symptoms. Most participants did not seek treatment for their problems [4]. The study reiterated the need for behavior change in communication toward healthcare practices [6]. An 8-week exercise program for postmenopausal women revealed an expressive decline in menopausal symptoms other than urogenital manifestations, and it was found that there was a powerful rise in lumbar strength and flexibility after 8 weeks of the Pilates exercise program [7].
Menopause is the edge of women’s reproducing action, but it proposes them to a new phase of life. The challenge is facilitated by the culture of silence that shrouds this phase. During menopause, women undergo many changes in their bodies. It can be taken in a positive or negative aspect. Many women are not aware of the symptoms that can occur and how they can be managed. Hence, teaching menopausal women about managing menopausal symptoms helps improve their QoL [1, 2].
Nuns often live in a unique cultural and social context. The study can explore the effectiveness of multimodal interventions, contributing to a more nuanced understanding of healthcare practices in this demographic. Our study findings can have implications for public health policies aimed at improving the health and well-being of nuns. It may guide the development of targeted interventions and support systems for this demographic. It provides valuable insights that can apply to nuns and other populations, contributing to advancing scientific understanding of women’s health. Multimodal interventions often involve a holistic approach, addressing physical, emotional, and spiritual aspects. The study may highlight the importance of comprehensive care, promoting empowerment and well-being among menopausal nuns. Thus, this study was done to assess the knowledge on menopause nuns, analyze the symptoms, understand the health-seeking behavior, describe the QoL, and evaluate the effect of multimodal intervention on the knowledge, symptoms, health-seeking behavior, and QoL among nuns at menopausal age.
Materials and Methods
This study used a quantitative experimental pre-test-post-test design. The present study assessed the knowledge, symptoms, health-seeking behavior, and QoL of nuns at menopausal age in 2020.
Kerala has 14 districts, and Kottayam District was selected using purposive sampling. There are 26 convents under St. Mathew’s Province in Kottayam District in India 20 were selected using the chit method. The St. Mathew’s Province consists of 437 sisters. An enumeration sampling technique was used to recruit women of menopausal age (nuns) residing in those selected convents. A pilot study was conducted in a subset of convents before the full-scale study, which allowed for the refinement of intervention protocols, assessment tools, and sampling strategies based on feedback from the pilot phase. The baseline characteristics such as health status, educational background, and previous exposure to menopause-related information can be used to assess the homogeneity or heterogeneity of the sample.
A total of 78 women of menopausal age who fulfilled the inclusion criteria (women in the menopausal period who are religious nuns) were selected. Women with serious medical illnesses like stroke and musculoskeletal problems were not included in the study. These respondents were divided into experimental and control groups. Accordingly, 39 subjects were designated to the experimental group, and the remaining 39 were treated as the control group. To facilitate the experiment’s smooth conducting, the experimental group was chosen from the first 10 convents and the control group from the remaining 10 (Figure 1). The sample size was calculated based on the findings of the pilot study.
The datasets include sociodemographic proforma. The tool consisted of age, educational status, occupation, information regarding menopause, attainment of menopause, and type of menopause. The structured knowledge questionnaire on menopause was developed based on definition, incidence, causes, physiology, symptoms, management, and complications. This tool’s validity (Content Validity Index [CVI]=0.747) and reliability (Intraclass Correlation [ICC]=0.877) were confirmed.
The menopausal symptoms were assessed using the modified menopause rating scale. It is a validated questionnaire comprising 25 items grouped into four categories: Vasomotor, psychosomatic, psychological, and urinary symptoms. Each item is a menopausal symptom, which is graded on a 4-point rating scale with a minimum score of 1 and a maximum of 4. The tool’s validity (CVI) and reliability (Cronbach α) were 0.876 and 0.877, respectively.
The QoL of menopausal-aged women is assessed by the modified 5-point Utian QoL (UQoL) scale [8]. The scale consists of 20 items and three domains: Occupation (7 items numbered 2, 3, 4, 14, 15, 16, 20), health (7 items numbered 5, 6, 7, 8, 13, 18, 19), emotional (6 items numbered 1, 9, 10, 11, 12, 17). Every item in the UQoL scale is scored using a 5-point Likert scale. The validity and reliability of the tool were 0.890 and 0.863, respectively.
The health-seeking behavior questionnaire had 9 questions that assessed the individuals in maintaining and improving their health and wellbeing. In the context of menopausal women, it could involve seeking medical advice, adopting healthy lifestyle practices, undergoing screenings, or following recommended healthcare guidelines. The approach involved using straightforward, dichotomous, and close-ended questions to gather specific and structured information about the health-seeking behavior of women in the menopausal age group. The minimum score was 0, and the maximum score was 9. The higher score is interpreted as good health-seeking behaviors.
Multimodal intervention includes a booklet on menopause and a video on pranayama and relaxation techniques. A booklet on menopause was given to the experimental group with a one-to-one teaching. The researcher demonstrated pranayama and relaxation techniques and a video to the participants. Instructed the participants to practice pranayama and relaxation techniques for 10 minutes daily for one month and to maintain a logbook. A post-test was conducted after one month to understand the effectiveness of multimodal interventions. After this, multimodal interventions were given to the control group as well.
The study was conducted among religious nuns who know how to read and write English. The participants were identified directly by the principal investigator. Written consent was obtained from the institution’s authority. Women at menopausal age who fulfilled the inclusion criteria were selected. Twenty institutions (convents) were chosen from the Kottayam District and divided into two groups of 10 each. Thirty-nine participants were selected from 10 convents and assigned as an experimental group; another 39 were selected from the other 10 convents and assigned as the control group. The researcher gave a self-introduction to the participants.
An explanation of the study and its confidentiality was provided. A pre-test on a structured knowledge questionnaire on menopause, a rating scale on symptoms experienced by women at menopausal age, a questionnaire on health-seeking behavior, and a modified Utian 5-point scale on QoL were administered to the experimental and control group, and the resulting data were collected. A booklet on menopause was given to the experimental group, and one-to-one teaching was given. The researcher underwent training on premenopausal exercise at the Punarjani School of Yoga. The researcher conducted one hour of training for the participants on pranayama and relaxation techniques, along with a video. Instructions were given to the participants on how to practice pranayama. Relaxation techniques of 10 minutes daily in the morning and evening for one month and maintaining a logbook are also included. The training was conducted at their respective convents. An information booklet on menopause was prepared for the participants by the researcher based on the literature review and suggestions from the experts. It briefly described the definition, incidence, causes, physiology, symptoms, management, and complications. A post-test was conducted after one month to understand the effectiveness of multimodal interventions, and the resulting data were collected.
Sample characteristics based on demographic variables, knowledge of menopause, menopausal symptoms, health-seeking behavior, and QoL among menopausal-age women were described using frequency and percentage. Effectiveness of multimodal intervention on knowledge, menopausal symptoms, and QoL assessed by Mann-Whitney U test. The association between knowledge, symptoms, and QoL among menopausal women was assessed by the chi-square test. The correlation between the score of symptoms and health-seeking behavior, QoL, and health-seeking behavior was evaluated using the Spearman rank correlation, and the Multivariate Analysis of covariance (Mancova) test was also used for the study.
Results
The study’s findings showed that most participants (48.7%) were 54-58 years in the experimental group and 45-48 years old in the control group (Table 1).
The comparison of knowledge on menopause groups before and after multimodal intervention revealed a significant change (P=0.01) between the knowledge scores of menopause women between the groups (Table 2).
A comparison of menopausal symptoms between the groups shows a significant difference (P=0.01) in menopausal symptoms in the experimental group after the intervention (Table 3).
The distribution of women’s health-seeking behavior at menopause in two groups is given in Table 4. Based on this Table, the health-seeking behavior is most related to the phrases “doctor advised to take more calcium-containing food” (74.4%) and “doctor suggested to do more exercises as a tranquilizer” (50%).
The QoL of women at menopausal age is shown in Table 5. It shows that intervention effectively improved the QoL of women at menopausal age, and the average QoL score in the two study groups after the intervention had a statistically significant difference based on the Mann-Whitney U test (P=0.01).
One-way MANCOVA was done with the respondents’ vasomotor, psychosomatic, and urinary symptoms as dependent variables and knowledge levels of the respondents versus low, moderate, and high as independent variables and their psychological core as a covariate. Since the P of Pillai’s Trace as per the multivariate test is <0.01, the null hypothesis is rejected at a 1% significance level. Hence, the respondents’ knowledge levels significantly influence their vasomotor, psychosomatic, and urinary symptoms (Table 6).
Similarly, the level of health and QoL of the respondents and the occupational level of the respondents significantly influence their vasomotor, psychosomatic, and urinary symptoms.
Discussion
The multimodal intervention was an effective strategy to increase the knowledge of women at menopausal age regarding menopause. The findings revealed reduced menopausal symptoms, improved QoL, and health-seeking behavior. A booklet on menopause, a video on pranayama, and relaxation techniques were the interventions provided to the participants. A positive result was seen in the knowledge, reduced symptoms, improved QoL, and health-seeking behavior.
A cluster randomized trial study was done in Iran among 68 women to assess the impact of multimedia intervention on the uncertainty about menopause. Implementing the education program helped improve knowledge and decrease uncertainty scores [9]. A quasi-experimental study among 99 middle-aged elementary, junior, and secondary teachers to determine the impact of health education on knowledge and attitude toward menopause. The multimodal intervention included lectures, leaflets, booklets, and group discussions. The study findings showed a significant increase in their knowledge and positive attitude towards menopause, which helped the women handle the symptoms of menopause [10]. A study in France on 5004 postmenopausal women shows that vaginal dryness and urinary urgency were the commonly reported symptoms and suggested the need for the education of the public through various educational programs [11]. Another study shows regular physical exercise intervention helps postmenopausal women to improve their vasomotor symptoms and overall wellbeing [12]. Multidisciplinary health education is effective in enhancing the menopausal syndrome and healthy lifestyle behavior of menopausal women [13], and the another study results show that the age of the women is not significantly correlated with QoL as the women did not find much difference in post menopause which contradict the present study [14].
According to the World Health Organization (WHO), menopausal symptoms can be managed with proper information. Researchers have emphasized that menopausal symptoms can be best handled by appropriate education, counseling, and symptom management. However, it is ineffective in practice because of the lack of proper resources and medical professionals [15]. Regarding the broad impact of social determinants of health on menopause, education and counseling are necessary to improve women’s attitudes towards menopause. Besides, improving emotional and social support, planning for lifestyle enhancement, and improving socioeconomic status are needed, which results in promoting women’s health during menopause [16]. Depression and urinary incontinence in menopausal women are related to each other, indicating the need for screening postmenopausal women with urinary incontinence and depression. Then, timely treatment and proper management can be given to improve their QoL [17].
Technological advancements such as music therapy are important in reducing menopausal symptoms. This therapy assists in achieving positive health outcomes by helping to alleviate issues during the menopausal period [18]. In the realm of menopausal women’s wellbeing, it is evident that they are frequently entangled in a web of physical symptoms and depressive states. This condition highlights the need for educational interventions, integrating cognitive behavioral therapy and tailored education addressing the physical aspects of menopausal transition. Therefore, it is necessary to develop and implement more comprehensive programs that consider lifestyle management and psychological support for menopausal women [19]. A balanced diet has a positive effect on the quality of sleep. Foods and meals containing sufficient protein, carbohydrates, and fats are also essential for good sleep quality. Scientific evidence indicates that good nutrition and quality sleep help maintain better health during menopause and perimenopause [20].
Based on the study results, intervention can be given to all menopausal women through mass media, drama, puppet shows, and role-play to improve knowledge, reduce menopausal symptoms, and improve the QoL.
The study was confined to a limited number of women at menopausal age and was organized in selected institutions, which limited the generalization of the study. A structured knowledge questionnaire was used for data collection, limiting the information that respondents could obtain.
The knowledge of women at menopausal age about menopause was low, and experience of menopausal symptoms was more. There is a need to educate menopausal women to improve their knowledge, reduce the symptoms experienced, and maintain a good QoL and health-seeking behavior.
Ethical Considerations
Compliance with ethical guidelines
The study was approved by the Kasturba Medical College and Kasturba Hospital Institutional Ethics Committee (Code: IEC 499/2020) and was registered at the Clinical Trial Registry of India (CTRI), New Delhi, India (Code: CTRI 2020/11/038529). Informed consent was acquired from all study participants.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
All authors contributed equally to the conception and design of the study, data collection and analysis, interception of the results and drafting of the manuscript. Each author approved the final version of the manuscript for submission.
Conflict of interest
All authors declared no conflict of interest.
Acknowledgments
The authors thank the research samples for their participation.
References
- Lu J, Liu J, Eden J. The experience of menopausal symptoms by Arabic women in Sydney. Climacteric. 2007; 10(1):72-9.[DOI:10.1080/13697130601159649] [PMID]
- Potter B, Schrager S, Dalby J, Torell E, Hampton A. Menopause. Prim Care. 2018; 45(4):625-41. [DOI:10.1016/j.pop.2018.08.001] [PMID]
- McKinlay SM, Brambilla DJ, Posner JG. The normal menopause transition. Maturitas. 2008; 61(1-2):4-16. [DOI:10.1016/j.maturitas.2008.09.005] [PMID]
- Santoro N, Epperson CN, Mathews SB. Menopausal symptoms and their management. Endocrinol Metab Clin North Am. 2015; 44(3):497-515. [DOI:10.1016/j.ecl.2015.05.001] [PMID]
- Twiss JJ, Wegner J, Hunter M, Kelsay M, Rathe-Hart M, Salado W. Perimenopausal symptoms, quality of life, and health behaviors in users and nonusers of hormone therapy. J Am Acad Nurse Pract. 2007; 19(11):602-13. [DOI:10.1111/j.1745-7599.2007.00260.x] [PMID]
- Ahlawat P, Singh MM, Garg S, Mala YM. Prevalence of depression and its association with sociodemographic factors in postmenopausal women in an urban resettlement colony of Delhi. J Midlife Health. 2019; 10(1):33-6. [DOI:10.4103/jmh.JMH_66_18] [PMID]
- Lee H, Caguicla JM, Park S, Kwak DJ, Won DY, Park Y, et al. Effects of 8-week Pilates exercise program on menopausal symptoms and lumbar strength and flexibility in postmenopausal women. J Exerc Rehabil. 2016; 12(3):247-51. [DOI:10.12965/jer.1632630.315] [PMID]
- Utian WH, Janata JW, Kingsberg SA, Schluchter M, Hamilton JC. The Utian quality of life (UQoL) scale: Development and validation of an instrument to quantify quality of life through and beyond menopause. Menopause. 2002; 9(6):402-10. [PMID]
- Afshari F, Bahri N, Sajjadi M, Mansoorian MR, Tohidinik HR. Menopause uncertainty: The impact of two educational interventions among women during menopausal transition and beyond. Prz Menopauzalny. 2020; 19(1):18-24. [DOI:10.5114/pm.2020.95305] [PMID]
- Gebretatyos H, Ghirmai L, Amanuel S, Gebreyohannes G, Tsighe Z, Tesfamariam EH. Effect of health education on knowledge and attitude of menopause among middle-age teachers. BMC Womens Health. 2020; 20(1):232. [DOI:10.1186/s12905-020-01095-2] [PMID]
- Trémollieres FA, André G, Letombe B, Barthélemy L, Pichard A, Gelas B, et al. Persistent gap in menopause care 20 years after the WHI: A population-based study of menopause-related symptoms and their management. Maturitas. 2022; 166:58-64. [PMID]
- Berin E, Spetz Holm AC, Hammar M, Lindh-Åstrand L, Berterö C. Postmenopausal women's experiences of a resistance training intervention against vasomotor symptoms: A qualitative study. BMC Womens Health. 2022 ; 22(1):320. [DOI:10.1186/s12905-022-01900-0] [PMID]
- Li Y, He H, Wang J, Chen Y, Wang C, Li X, et al. Effect of multidisciplinary health education based on lifestyle medicine on menopausal syndrome and lifestyle behaviors of menopausal women: A clinical controlled study. Front Public Health. 2023; 11:1119352. [DOI:10.3389/fpubh.2023.1119352] [PMID]
- Kafaei-Atria M, Nasiri S, Izadi-Avanji FS, Abbaszadeh F. Quality of life and its relevant factors in menopausal women. J Holistic NursMidwifery. 2022; 32(2):109-15. [DOI:10.32598/jhnm.32.2.2143]
- WHO. Menopause. Geneva: WHO; 2024. [Link]
- Namazi M, Sadeghi R, Behboodi Moghadam Z. Social determinants of health in menopause: An integrative review. Int J Womens Health. 2019; 11:637-47. [DOI:10.2147/IJWH.S228594] [PMID]
- Mansour Ghanaie M, Abdolahi E, Kazemnezhad Leili E, Hojat Ansari R, Asgari Galebin S M. Comparing the prevalence of depression in postmenopausal women with and without urinary incontinence. J Holistic NursMidwifery. 2020; 30(2):86-92 [DOI:10.32598/jhnm.30.2.86]
- Ugurlu M, Şahin MV, Oktem OH. The effect of music on menopausal symptoms, sleep quality,and depression: A randomized controlled trial. Rev Assoc Med Bras (1992). 2024;7 0(2):e20230829. [DOI:10.1590/1806-9282.20230829] [PMID]
- Kim JH, Yu HJ. The effectiveness of cognitive behavioral therapy on depression and sleep problems for climacteric women: A systematic review and meta-analysis. J Clin Med. 2024; 13(2):412. [DOI:10.3390/jcm13020412] [PMID]
- Erdélyi A, Pálfi E, Tűű L, Nas K, Szűcs Z, Török M, et al. The importance of nutrition in menopause and perimenopause-A review. Nutrients. 2023; 16(1):27. [DOI:10.3390/nu16010027] [PMID]
Article Type : Research |
Subject:
Special
Received: 2023/04/11 | Accepted: 2024/03/12 | Published: 2025/06/10
Received: 2023/04/11 | Accepted: 2024/03/12 | Published: 2025/06/10
Send email to the article author
| Rights and permissions | |
 | This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
