Mon, Jul 22, 2024
Volume 33, Issue 4 (9-2023)
JHNM 2023, 33(4): 278-287 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Pourbayram N, Chehrzad M, Karkhah S, Kazemnezhad Leili E, Jafaraghaee F. Compliance With Safety in Nursing Care, Equipment, and Physical Setting in Pediatric Wards. JHNM 2023; 33 (4) :278-287
URL: http://hnmj.gums.ac.ir/article-1-1512-en.html
URL: http://hnmj.gums.ac.ir/article-1-1512-en.html
Nasrin Pourbayram1 

 , Minoomitra Chehrzad2 , Samad Karkhah1 , Ehsan Kazemnezhad Leili3 , Fateme Jafaraghaee * 4
, Minoomitra Chehrzad2 , Samad Karkhah1 , Ehsan Kazemnezhad Leili3 , Fateme Jafaraghaee * 4
, Minoomitra Chehrzad2 , Samad Karkhah1 , Ehsan Kazemnezhad Leili3 , Fateme Jafaraghaee * 4
1- Nursing (MSN), School of Nursing and Midwifery, Guilan University of Medical Sciences, Rasht, Iran.
2- Assistant Professor, Department of Nursing, School of Nursing and Midwifery, Guilan University of Medical Sciences, Rasht, Iran.
3- Associate Professor, Department of Biostatistics, School of Nursing and Midwifery, Guilan University of Medical Sciences, Rasht, Iran.
4- Associate Professor, Department of Nursing, School of Nursing and Midwifery, Guilan University of Medical Sciences, Rasht, Iran. ,fja_a80@yahoo.com
2- Assistant Professor, Department of Nursing, School of Nursing and Midwifery, Guilan University of Medical Sciences, Rasht, Iran.
3- Associate Professor, Department of Biostatistics, School of Nursing and Midwifery, Guilan University of Medical Sciences, Rasht, Iran.
4- Associate Professor, Department of Nursing, School of Nursing and Midwifery, Guilan University of Medical Sciences, Rasht, Iran. ,
Full-Text [PDF 513 kb]
(210 Downloads)
| Abstract (HTML) (584 Views)
Full-Text: (188 Views)
Introduction
Patient safety is among the most important medical issues and challenges in developed and developing countries [1, 2]. Patient safety is defined as protecting the patient from injury during health care [3]. Due to the economic crisis, many countries are paying attention to unsafe care because unsafe care significantly impacts the economy and imposes high costs on the medical system and patients [4]. Children are more vulnerable due to their low physical and cognitive development and continuous growth and development compared to other age groups. Therefore, it is inevitable to develop ways to prevent injuries during the hospitalization of children [5, 6]. Safety-related accidents of children are included in 28.3% of all safety accidents in the United States [7].
Due to the misconception that hospitals are the guarantors of children’s safety, discussions about children’s safety are often overlooked [8]. Therefore, assessing the safety of children in clinical settings in various dimensions, such as the safety of nursing care, physical settings, and equipment, is very important [9]. An Australian study found that children’s unfamiliarity with medical practices, physical settings, unsafe equipment, and reduced physical function due to illness often exposes them to various injuries, such as falls and trauma [10]. Also, a study in Iran shows that adherence to safety guidelines related to equipment, physical setting, and nursing care in pediatric wards are 77.6%, 45.6%, and 66.5%, respectively, indicating a moderate safety status level [11].
Meanwhile, pediatric nurses play a very important role in patient safety as the main member of the patient care system [12]. Missed nursing care is directly related to patient outcomes, and if continued, inefficient care could affect patient safety and quality of care [9].
Patient safety is affected by factors such as nurses’ education level, professional nursing commitment, high nursing duties, healthcare workers’ adequacy, and nurses’ burnout [9, 12]. In addition, nurses’ work setting and safety levels, proper communication, and teamwork of nurses with physicians can be effective for safe care [11]. Research on factors related to children’s safety has been different and limited based on differences in individual and occupational variables of nurses [9, 11, 12]. Therefore, compliance with safety in nursing care, equipment, and physical setting in pediatric wards is crucial.
Materials and Methods
In a cross-sectional study, 342 nursing care, equipment, and physical setting related to safety were assessed in three pediatric wards of pediatric education and treatment centers in Rasht City, Guilan Province, Iran. Ward 1 had 9 active beds where 7 nurses provided nursing care to patients. Ward 2 had 9 active beds where 7 nurses provided nursing care to patients. Ward 3 had 15 active beds where 11 nurses provided nursing care to patients. Data were collected via convenient sampling from May to July 2019. Nursing care was assessed among nurses with at least 6 months of work experience in pediatric wards. They had consented to participate in the study. Ultimately, 342 nursing care and 5 views of equipment and physical setting related to safety in pediatric wards were assessed.
Data were collected using 6 checklists: Safety-related individual, occupational and organizational factors, nursing care, equipment, and the physical setting. These checklists were developed by reviewing the literature on the safety of nursing care, physical setting, and equipment in pediatric wards [13, 14, 15].
Nurses’ safety-related factors consisted of age, sex, marital status, having children, and stress during shifts of nurses. Nurses’ organizational factors included the history of encouragement, the possibility of career advancement, and familiarity with the description of tasks in the organization was gathered. Nurses’ occupational factors were the level of education, years of overall working experience, number of patients monitored, shift work, overtime, participation in training-safety workshops, interest in the nursing profession, employment in the second job, clinical supervisor round in each shift, and sufficient time to perform tasks were gathered.
Safety adherence in nursing care was assessed by a 45-item scale, scored on a 3-point Likert-type scale. This tool has 9 subscales: Children’s identity control (4 items), shift change (5 items), record patient information (6 items), medicinal card writing (5 items), liquid and drug therapy (8 items), hand hygiene (5 items), respiratory care (4 items), peripheral venous catheter care (4 items), and fall prevention (4 items). The researcher has assessed the safety of nursing care through one observation at 3 levels: Undesirable (score of 0), moderate (score of 1), and desirable (score of 2). The minimum and maximum scores assigned to the items were 0 and 100, respectively. A higher score indicates greater safety in nursing care.
The safety of the physical setting was assessed by an 8-item scale, scored on a 3-point Likert-type scale. The items were as follows: The protection of outlets, the outlet is not damaged, the windows are protected, the windows have nets, the floor is not slippery, the nurse call is available, the possibility of free movement with wheelchairs through the ramp, parents have access to nurse call in the bathroom. The researcher assessed the safety physical setting through 5 observations at three levels: Undesirable (score of 0), moderate (score of 1), and desirable (score of 2). The minimum and maximum scores assigned to the items were 0 and 100, respectively. A higher score indicates greater safety in the physical setting. The mean score of 5 observations was used to detect the total score.
The safety of the equipment was assessed by an 18-item scale, scored on a 3-point Likert-type scale. The tool includes 4 subscales: Emergency boxes (5 items), general equipment (7 items), pharmaceutical refrigerators (3 items), and monitoring equipment (3 items). The researcher assessed the safety equipment through 5 observations at three levels: Undesirable (score of 0), moderate (score of 1), and desirable (score of 2). The minimum and maximum scores assigned to the items were 0 and 100, respectively. A higher score indicates greater safety of the equipment. The mean score of five observations was used to detect the total score.
Face and content validity of the researcher-made checklists was conducted by a 15-member panel of pediatric faculty members, nurses, and clinical instructors. These tools were approved and accepted with a content validity index and content validity ratio of 0. 91 and 0.83, respectively. The inter-rater reliability was used to determine the reliability of the instruments. These tools were provided to two observers (one of the researchers and a master’s student of pediatric nursing). Two observers completed the checklists simultaneously, in one ward, for 10 nursing care. Then, Cohen’s kappa coefficient between the obtained scores from the observation was calculated as 0.78.
The researcher assessed the safety of nursing care using a relatively invisible observation of nurses. For reassurance, the researcher completed checklists of physical setting and equipment safety in five observations at a 2-week interval.
SPSS software, version 16 (SPSS Inc., Chicago, IL, USA) was used for statistical analysis. Quantitative and qualitative variables were presented using Mean±SD and frequency (percentage). The Mann-Whitney and Kruskal-Wallis tests were used for data analysis. The significance level was considered 0.05.
Results
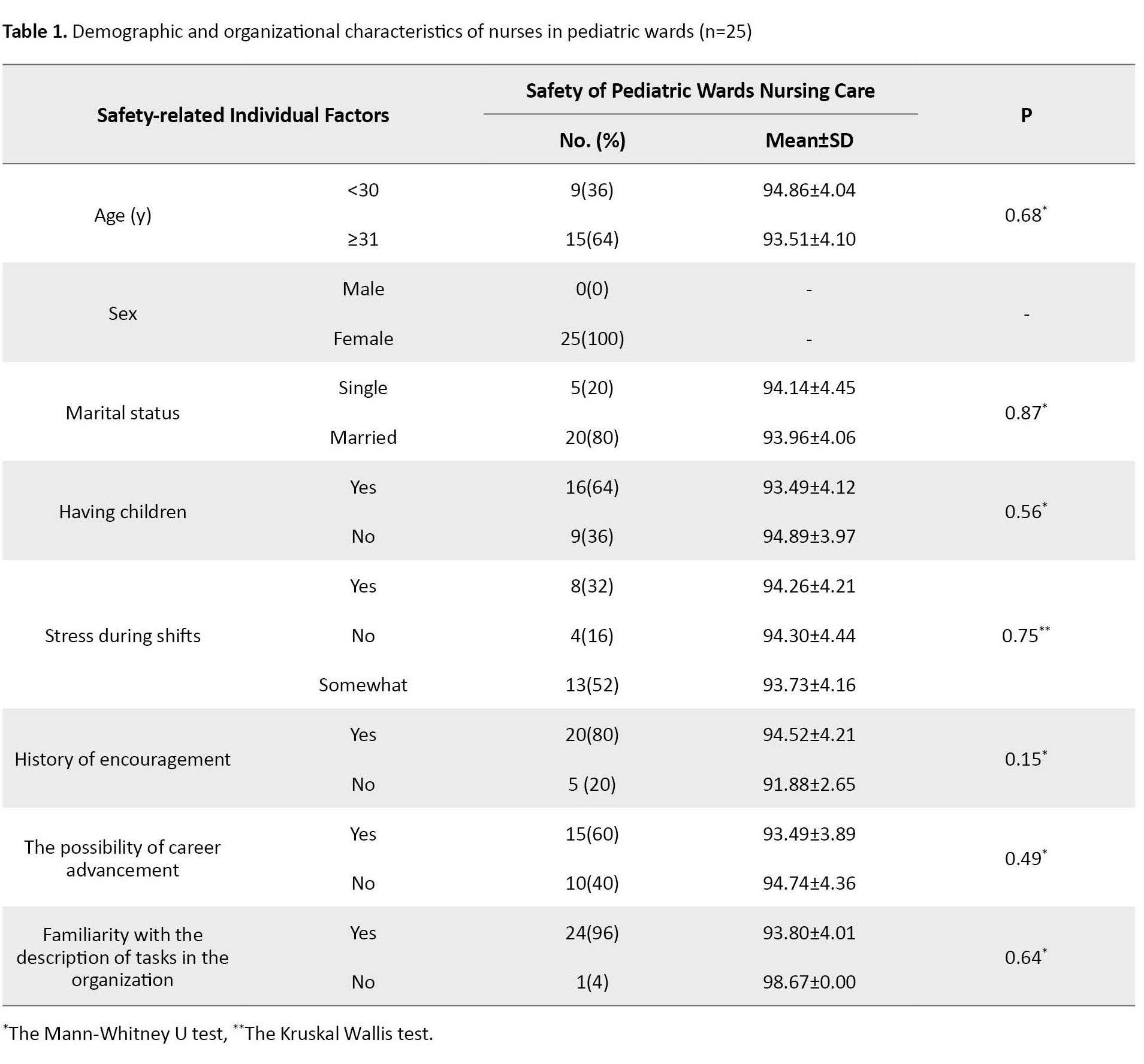
A total of 342 nursing care and 5 views of equipment and physical setting related to safety in pediatric wards were assessed. Of nurses, 36% were less than 30 years, 100% were female, 80% were married, and 88% had a BS in Nursing. The safety of nursing care in terms of individual and organizational factors was not significant (Table 1).
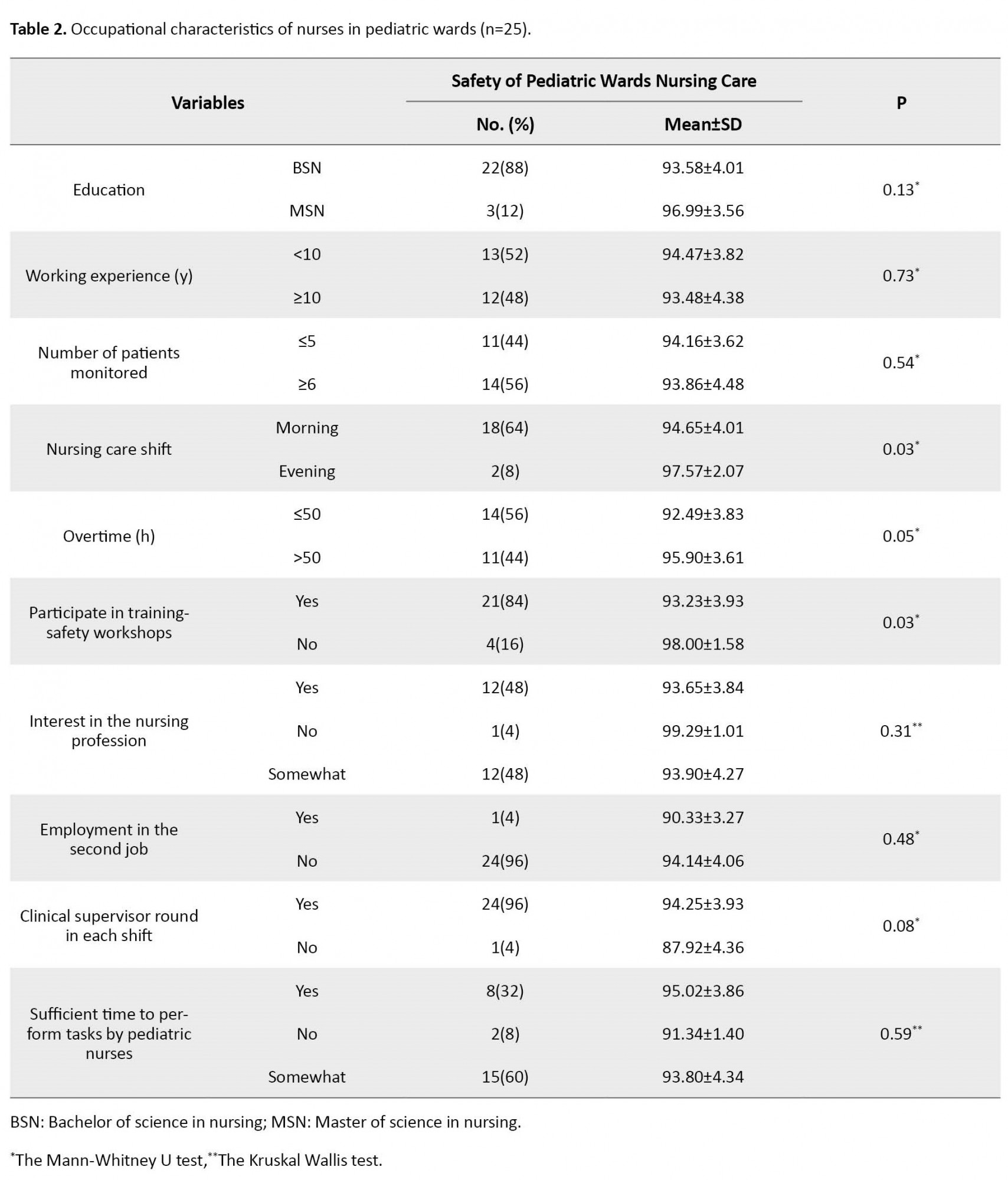
About 52% were less than 10 years of overall working experience, 44% had less than 5 patients under monitored, and 32% had a history of stress during shifts. Also, 80% of nurses had a history of encouragement, and 60% reported the possibility of career advancement. Based on the Mann-Whitney and Kruskal-Wallis tests, the safety of nursing care in terms of shift work (P=0.03), overtime (P<0.05), and participation in training-safety workshops (P=0.03) were significant (Table 2).
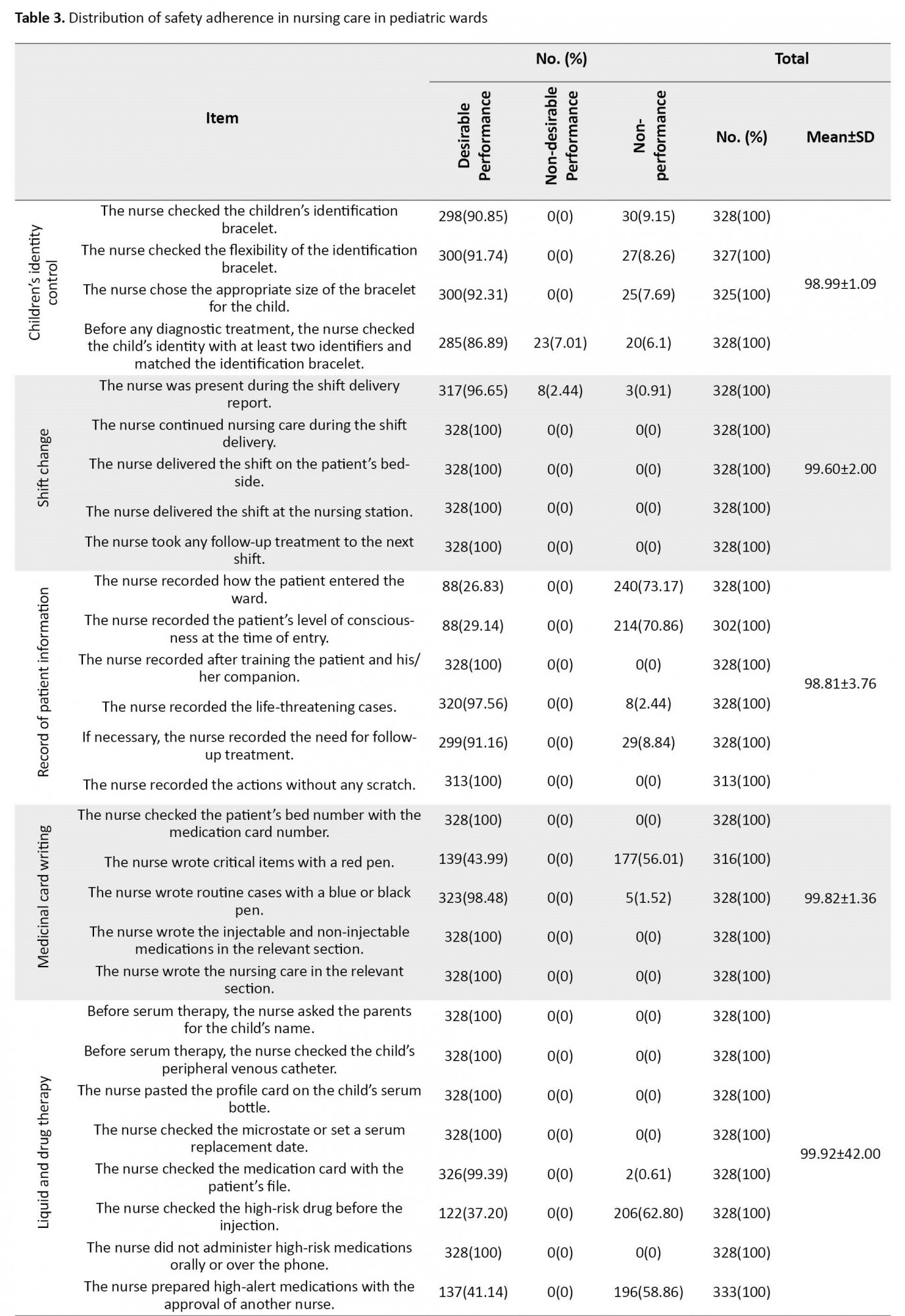
Also, 98.92% of nursing care in pediatric wards had a safety score above the mean score of the checklist. The safety of nursing care was higher in 1(95.75%), 2(93.42%), and 3 wards (91.80%), respectively. The highest and lowest safety of nursing care were related to medicinal card writing (100%) and hand hygiene (95.22%), respectively (Table 3).

About 93.75% of physical settings in pediatric wards had a safety score above the mean score. In the items of “the outlet is not damaged”(100%), “the windows of the children’s rooms are protected” (100%), “the windows of the children’s rooms have nets” (100%), “the floor is not slippery” (100%), “the nurse call is available” (100%), “the possibility of free movement with wheelchairs through the ramp” (100%), and “parents have access to nurse call in the bathroom” (100%), all pediatric wards had a safety score above the mean. However, only in the item “the protection of outlets” (10.23±1.3), all pediatric wards had a safety score lower than the mean.
The equipment of the pediatric wards had a safety score above the mean. The lowest mean score was related to “hand hygiene of nurses” (95.22±2.53), and the highest mean score was related to “peripheral venous catheter care” (99.89±56.00). In ward 2, the safety of pediatric wards equipment was more than in the other two wards. Also, in the subscale of monitoring equipment, ward 3 had a safety score lower than the mean.
Discussion
This study showed that nursing care, physical settings, and equipment in pediatric wards had a safety score above the mean. The safety of nursing care in terms of shift work, overtime, and participation in training-safety workshops was significant.
According to the obtained results in this study, nursing care in pediatric wards had a safety score above the mean. However, nurses lacked a desirable performance on items such as preparing high-alert medications with the approval of another nurse and writing special cases with a red pen. The findings of the present study were consistent with the results of studies in the Netherlands [16], Germany [17], Italy [18], and China [19], showing that activities such as identification, evaluation, and injection of high-risk drugs to patients, especially in children due to physiological limitations in them, have been associated with high-risk, and require special attention. In particular, when unsafe drug activity is a common mistake in the nursing system, it can affect patients’ safety [20]. Also, a systematic review and meta-analysis showed that medication errors are common in pediatric wards [21]. A study in Australia showed that three key factors are associated with nurses’ safety errors, including extensive duties of nurses, physical setting, and non-adherence to pharmaceutical and clinical policy guidelines [10]. In addition, studies have recently conducted interventions to improve drug safety and offer a variety of strategies to reduce medication errors, such as training, availability of scientific resources, and establishing a system-based quality committee. Also, studies have suggested creating a safe setting and non-distracting for drug use and appropriate technology, such as electronic drug warning systems [22, 23, 24]. According to the results of studies, medication error is one of the most important factors in reducing safety in pediatric wards. Therefore, various strategies can be used to reduce medication errors, including holding medication workshops for each ward nurse, having pharmacology books in the ward library, isolating and marking high-risk drugs, and reviewing and approving high-risk drugs by the second nurse.
Based on the results of the present study, physical settings in pediatric wards had a safety score above the mean. The physical setting in pediatric wards should be given special attention because the game is vital to children’s development [25]. Adherence to standards in the safety of the physical setting and implementing preventive measures such as adequate supervision and age-appropriate game equipment can reduce the potential risks to children’s safety.
Based on the result of the present study, the equipment in pediatric wards had a safety score above the mean. This finding is consistent with studies in the United States and Brazil [26, 27]. According to a study in the United States, safe equipment was an important factor in reducing accidents and increasing the safety of nurses and patients [26]. In addition, some equipment, such as the Broselow tape and smart injection pumps, are used to improve children’s safety [20]. Therefore, it is possible to equip pediatric wards with safe and standard equipment to increase the safety of nurses and children.
The safety of nursing care regarding shift work, overtime, and participation in training-safety workshops was significant. The results of studies in the United States [28] and Taiwan [29] showed that adequate income for nurses can increase job satisfaction and improve the quality of nursing care. In addition, some occupational variables, such as shift work, overtime, and participation in training-safety workshops, are predictors of nursing care safety. Improving employment status can increase the safety of nursing care. The results of a study in Iran show that high workload and overtime are directly related to increased medication errors in pediatric nurses [30]. A study in the United States shows that nurses’ working conditions are a major factor in patient safety [26]. In contrast, a study in Brazil shows that lack of proper management is a major factor in patient safety. Also, to prevent accidents, strengthening safety monitoring systems is effective in nursing care [27]. Also, studies in Iran and Canada have shown that implementing an empowerment program for nurses and head nurses can improve safety culture and their understanding of patient safety, safety in transfers, reduce medication errors, and improve teamwork among nurses [31, 32]. Overall, nurses are key players in the health care system, especially in the care of children. Paying attention to the factors affecting patient safety, emphasizing nurses, such as safe nursing care, physical setting, and equipment, especially in low- or middle-income countries, such as Iran, is important in-patient health and safety.
One of the strengths of this study is its inclusiveness in terms of the variables studied. In addition to the issues related to falling and accidents, which were the most common causes of poor safety, the impact of the physical setting and equipment was studied. On the other hand, the limitation of this study was related to its conduct in a single center.
On the whole, the safety of children can be improved by reducing work shifts and overtime of nurses, participating in training-safety workshops, and having an adequate supply of equipment to ensure safe practice in pediatric wards. Based on the findings of the present study, it is suggested that researchers in future studies assess the factors related to the adherence of pediatric nurses to safety guidelines about nursing care, physical setting, and equipment.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Institutional Ethics Committee of Guilan University of Medical Sciences (Code: IR.GUMS.REC.1398.040). Written informed consent was obtained from all participants after the researchers explained the aim of the study.
Funding
The paper was extracted from the MSc thesis of Nasrin Pourbayram, approved by Department of Pediatric Nursing, Guilan University of Medical Sciences.
Authors' contributions
Conceptualization, draft preparation, resources, investigation, editing, and review: All authors; Data analysis: Ehsan Kazemnejhad Leili, Nasrin Pourbayram, Fateme Jafaraghaee, and Samad Karkhah.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
We thank all those who cooperated with the research team in conducting the study.
References
Patient safety is among the most important medical issues and challenges in developed and developing countries [1, 2]. Patient safety is defined as protecting the patient from injury during health care [3]. Due to the economic crisis, many countries are paying attention to unsafe care because unsafe care significantly impacts the economy and imposes high costs on the medical system and patients [4]. Children are more vulnerable due to their low physical and cognitive development and continuous growth and development compared to other age groups. Therefore, it is inevitable to develop ways to prevent injuries during the hospitalization of children [5, 6]. Safety-related accidents of children are included in 28.3% of all safety accidents in the United States [7].
Due to the misconception that hospitals are the guarantors of children’s safety, discussions about children’s safety are often overlooked [8]. Therefore, assessing the safety of children in clinical settings in various dimensions, such as the safety of nursing care, physical settings, and equipment, is very important [9]. An Australian study found that children’s unfamiliarity with medical practices, physical settings, unsafe equipment, and reduced physical function due to illness often exposes them to various injuries, such as falls and trauma [10]. Also, a study in Iran shows that adherence to safety guidelines related to equipment, physical setting, and nursing care in pediatric wards are 77.6%, 45.6%, and 66.5%, respectively, indicating a moderate safety status level [11].
Meanwhile, pediatric nurses play a very important role in patient safety as the main member of the patient care system [12]. Missed nursing care is directly related to patient outcomes, and if continued, inefficient care could affect patient safety and quality of care [9].
Patient safety is affected by factors such as nurses’ education level, professional nursing commitment, high nursing duties, healthcare workers’ adequacy, and nurses’ burnout [9, 12]. In addition, nurses’ work setting and safety levels, proper communication, and teamwork of nurses with physicians can be effective for safe care [11]. Research on factors related to children’s safety has been different and limited based on differences in individual and occupational variables of nurses [9, 11, 12]. Therefore, compliance with safety in nursing care, equipment, and physical setting in pediatric wards is crucial.
Materials and Methods
In a cross-sectional study, 342 nursing care, equipment, and physical setting related to safety were assessed in three pediatric wards of pediatric education and treatment centers in Rasht City, Guilan Province, Iran. Ward 1 had 9 active beds where 7 nurses provided nursing care to patients. Ward 2 had 9 active beds where 7 nurses provided nursing care to patients. Ward 3 had 15 active beds where 11 nurses provided nursing care to patients. Data were collected via convenient sampling from May to July 2019. Nursing care was assessed among nurses with at least 6 months of work experience in pediatric wards. They had consented to participate in the study. Ultimately, 342 nursing care and 5 views of equipment and physical setting related to safety in pediatric wards were assessed.
Data were collected using 6 checklists: Safety-related individual, occupational and organizational factors, nursing care, equipment, and the physical setting. These checklists were developed by reviewing the literature on the safety of nursing care, physical setting, and equipment in pediatric wards [13, 14, 15].
Nurses’ safety-related factors consisted of age, sex, marital status, having children, and stress during shifts of nurses. Nurses’ organizational factors included the history of encouragement, the possibility of career advancement, and familiarity with the description of tasks in the organization was gathered. Nurses’ occupational factors were the level of education, years of overall working experience, number of patients monitored, shift work, overtime, participation in training-safety workshops, interest in the nursing profession, employment in the second job, clinical supervisor round in each shift, and sufficient time to perform tasks were gathered.
Safety adherence in nursing care was assessed by a 45-item scale, scored on a 3-point Likert-type scale. This tool has 9 subscales: Children’s identity control (4 items), shift change (5 items), record patient information (6 items), medicinal card writing (5 items), liquid and drug therapy (8 items), hand hygiene (5 items), respiratory care (4 items), peripheral venous catheter care (4 items), and fall prevention (4 items). The researcher has assessed the safety of nursing care through one observation at 3 levels: Undesirable (score of 0), moderate (score of 1), and desirable (score of 2). The minimum and maximum scores assigned to the items were 0 and 100, respectively. A higher score indicates greater safety in nursing care.
The safety of the physical setting was assessed by an 8-item scale, scored on a 3-point Likert-type scale. The items were as follows: The protection of outlets, the outlet is not damaged, the windows are protected, the windows have nets, the floor is not slippery, the nurse call is available, the possibility of free movement with wheelchairs through the ramp, parents have access to nurse call in the bathroom. The researcher assessed the safety physical setting through 5 observations at three levels: Undesirable (score of 0), moderate (score of 1), and desirable (score of 2). The minimum and maximum scores assigned to the items were 0 and 100, respectively. A higher score indicates greater safety in the physical setting. The mean score of 5 observations was used to detect the total score.
The safety of the equipment was assessed by an 18-item scale, scored on a 3-point Likert-type scale. The tool includes 4 subscales: Emergency boxes (5 items), general equipment (7 items), pharmaceutical refrigerators (3 items), and monitoring equipment (3 items). The researcher assessed the safety equipment through 5 observations at three levels: Undesirable (score of 0), moderate (score of 1), and desirable (score of 2). The minimum and maximum scores assigned to the items were 0 and 100, respectively. A higher score indicates greater safety of the equipment. The mean score of five observations was used to detect the total score.
Face and content validity of the researcher-made checklists was conducted by a 15-member panel of pediatric faculty members, nurses, and clinical instructors. These tools were approved and accepted with a content validity index and content validity ratio of 0. 91 and 0.83, respectively. The inter-rater reliability was used to determine the reliability of the instruments. These tools were provided to two observers (one of the researchers and a master’s student of pediatric nursing). Two observers completed the checklists simultaneously, in one ward, for 10 nursing care. Then, Cohen’s kappa coefficient between the obtained scores from the observation was calculated as 0.78.
The researcher assessed the safety of nursing care using a relatively invisible observation of nurses. For reassurance, the researcher completed checklists of physical setting and equipment safety in five observations at a 2-week interval.
SPSS software, version 16 (SPSS Inc., Chicago, IL, USA) was used for statistical analysis. Quantitative and qualitative variables were presented using Mean±SD and frequency (percentage). The Mann-Whitney and Kruskal-Wallis tests were used for data analysis. The significance level was considered 0.05.
Results
A total of 342 nursing care and 5 views of equipment and physical setting related to safety in pediatric wards were assessed. Of nurses, 36% were less than 30 years, 100% were female, 80% were married, and 88% had a BS in Nursing. The safety of nursing care in terms of individual and organizational factors was not significant (Table 1).
About 52% were less than 10 years of overall working experience, 44% had less than 5 patients under monitored, and 32% had a history of stress during shifts. Also, 80% of nurses had a history of encouragement, and 60% reported the possibility of career advancement. Based on the Mann-Whitney and Kruskal-Wallis tests, the safety of nursing care in terms of shift work (P=0.03), overtime (P<0.05), and participation in training-safety workshops (P=0.03) were significant (Table 2).
Also, 98.92% of nursing care in pediatric wards had a safety score above the mean score of the checklist. The safety of nursing care was higher in 1(95.75%), 2(93.42%), and 3 wards (91.80%), respectively. The highest and lowest safety of nursing care were related to medicinal card writing (100%) and hand hygiene (95.22%), respectively (Table 3).
About 93.75% of physical settings in pediatric wards had a safety score above the mean score. In the items of “the outlet is not damaged”(100%), “the windows of the children’s rooms are protected” (100%), “the windows of the children’s rooms have nets” (100%), “the floor is not slippery” (100%), “the nurse call is available” (100%), “the possibility of free movement with wheelchairs through the ramp” (100%), and “parents have access to nurse call in the bathroom” (100%), all pediatric wards had a safety score above the mean. However, only in the item “the protection of outlets” (10.23±1.3), all pediatric wards had a safety score lower than the mean.
The equipment of the pediatric wards had a safety score above the mean. The lowest mean score was related to “hand hygiene of nurses” (95.22±2.53), and the highest mean score was related to “peripheral venous catheter care” (99.89±56.00). In ward 2, the safety of pediatric wards equipment was more than in the other two wards. Also, in the subscale of monitoring equipment, ward 3 had a safety score lower than the mean.
Discussion
This study showed that nursing care, physical settings, and equipment in pediatric wards had a safety score above the mean. The safety of nursing care in terms of shift work, overtime, and participation in training-safety workshops was significant.
According to the obtained results in this study, nursing care in pediatric wards had a safety score above the mean. However, nurses lacked a desirable performance on items such as preparing high-alert medications with the approval of another nurse and writing special cases with a red pen. The findings of the present study were consistent with the results of studies in the Netherlands [16], Germany [17], Italy [18], and China [19], showing that activities such as identification, evaluation, and injection of high-risk drugs to patients, especially in children due to physiological limitations in them, have been associated with high-risk, and require special attention. In particular, when unsafe drug activity is a common mistake in the nursing system, it can affect patients’ safety [20]. Also, a systematic review and meta-analysis showed that medication errors are common in pediatric wards [21]. A study in Australia showed that three key factors are associated with nurses’ safety errors, including extensive duties of nurses, physical setting, and non-adherence to pharmaceutical and clinical policy guidelines [10]. In addition, studies have recently conducted interventions to improve drug safety and offer a variety of strategies to reduce medication errors, such as training, availability of scientific resources, and establishing a system-based quality committee. Also, studies have suggested creating a safe setting and non-distracting for drug use and appropriate technology, such as electronic drug warning systems [22, 23, 24]. According to the results of studies, medication error is one of the most important factors in reducing safety in pediatric wards. Therefore, various strategies can be used to reduce medication errors, including holding medication workshops for each ward nurse, having pharmacology books in the ward library, isolating and marking high-risk drugs, and reviewing and approving high-risk drugs by the second nurse.
Based on the results of the present study, physical settings in pediatric wards had a safety score above the mean. The physical setting in pediatric wards should be given special attention because the game is vital to children’s development [25]. Adherence to standards in the safety of the physical setting and implementing preventive measures such as adequate supervision and age-appropriate game equipment can reduce the potential risks to children’s safety.
Based on the result of the present study, the equipment in pediatric wards had a safety score above the mean. This finding is consistent with studies in the United States and Brazil [26, 27]. According to a study in the United States, safe equipment was an important factor in reducing accidents and increasing the safety of nurses and patients [26]. In addition, some equipment, such as the Broselow tape and smart injection pumps, are used to improve children’s safety [20]. Therefore, it is possible to equip pediatric wards with safe and standard equipment to increase the safety of nurses and children.
The safety of nursing care regarding shift work, overtime, and participation in training-safety workshops was significant. The results of studies in the United States [28] and Taiwan [29] showed that adequate income for nurses can increase job satisfaction and improve the quality of nursing care. In addition, some occupational variables, such as shift work, overtime, and participation in training-safety workshops, are predictors of nursing care safety. Improving employment status can increase the safety of nursing care. The results of a study in Iran show that high workload and overtime are directly related to increased medication errors in pediatric nurses [30]. A study in the United States shows that nurses’ working conditions are a major factor in patient safety [26]. In contrast, a study in Brazil shows that lack of proper management is a major factor in patient safety. Also, to prevent accidents, strengthening safety monitoring systems is effective in nursing care [27]. Also, studies in Iran and Canada have shown that implementing an empowerment program for nurses and head nurses can improve safety culture and their understanding of patient safety, safety in transfers, reduce medication errors, and improve teamwork among nurses [31, 32]. Overall, nurses are key players in the health care system, especially in the care of children. Paying attention to the factors affecting patient safety, emphasizing nurses, such as safe nursing care, physical setting, and equipment, especially in low- or middle-income countries, such as Iran, is important in-patient health and safety.
One of the strengths of this study is its inclusiveness in terms of the variables studied. In addition to the issues related to falling and accidents, which were the most common causes of poor safety, the impact of the physical setting and equipment was studied. On the other hand, the limitation of this study was related to its conduct in a single center.
On the whole, the safety of children can be improved by reducing work shifts and overtime of nurses, participating in training-safety workshops, and having an adequate supply of equipment to ensure safe practice in pediatric wards. Based on the findings of the present study, it is suggested that researchers in future studies assess the factors related to the adherence of pediatric nurses to safety guidelines about nursing care, physical setting, and equipment.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Institutional Ethics Committee of Guilan University of Medical Sciences (Code: IR.GUMS.REC.1398.040). Written informed consent was obtained from all participants after the researchers explained the aim of the study.
Funding
The paper was extracted from the MSc thesis of Nasrin Pourbayram, approved by Department of Pediatric Nursing, Guilan University of Medical Sciences.
Authors' contributions
Conceptualization, draft preparation, resources, investigation, editing, and review: All authors; Data analysis: Ehsan Kazemnejhad Leili, Nasrin Pourbayram, Fateme Jafaraghaee, and Samad Karkhah.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
We thank all those who cooperated with the research team in conducting the study.
References
- Donaldson LJ, Kelley ET, Dhingra-Kumar N, Kieny MP, Sheikh A. Medication without harm: WHO's third global patient safety challenge. Lancet. 2017; 389(10080):1680-1. [DOI:10.1016/S0140-6736(17)31047-4] [PMID]
- Michel P, Brami J, Chanelière M, Kret M, Mosnier A, Dupie I, et al. Patient safety incidents are common in primary care: A national prospective active incident reporting survey. PLoS One. 2017; 12(2):e0165455. [DOI:10.1371/journal.pone.0165455] [PMID]
- Farokhzadian J, Dehghan Nayeri N, Borhani F. The long way ahead to achieve an effective patient safety culture: Challenges perceived by nurses. BMC Health Serv Res. 2018; 18(1):654. [DOI:10.1186/s12913-018-3467-1] [PMID]
- Simou E, Koutsogeorgou E. Effects of the economic crisis on health and healthcare in Greece in the literature from 2009 to 2013: A systematic review. Health Policy. 2014; 115(2-3):111-9. [DOI:10.1016/j.healthpol.2014.02.002] [PMID]
- Oh WO, Kim E, Im Y, Han J, Kim M. Developing a conceptual model of pediatric inpatient safety accidents: A mixed methods approach. Nurs Health Sci. 2020; 22(3):777-86. [DOI:10.1111/nhs.12728] [PMID]
- Wegner W, Silva MUMD, Peres MA, Bandeira LE, Frantz E, Botene DZA, et al. Patient safety in the care of hospitalised children: Evidence for paediatric nursing. Rev Gaucha Enferm. 2017; 38(1):e68020. [DOI:10.1590/1983-1447.2017.01.68020] [PMID]
- Lee YS, Oh WO. Development of educational content for nurses to prevent safety accidents of hospitalized children: Delphi approach. Child Health Nurs Res. 2019; 25(1):74-84. [DOI:10.4094/chnr.2019.25.1.74] [PMID]
- Ghosh AK, Badillo-Urquiola K, Guha S, LaViola Jr JJ, Wisniewski PJ. Safety vs. surveillance: What children have to say about mobile apps for parental control. Proceedings of the 2018 CHI Conference on Human Factors in Computing Systems. 2018; 124:1-14. [Link]
- Kim KJ, Yoo MS, Seo EJ. Exploring the influence of nursing work environment and patient safety culture on missed nursing care in Korea. Asian Nurs Res. 2018; S1976-1317(17)30683-7. [DOI:10.1016/j.anr.2018.04.003] [PMID]
- Robinson S, Graham A. Feeling safe, avoiding harm: Safety priorities of children and young people with disability and high support needs. J Intellect Disabil. 2021; 25(4):583–602. [DOI:10.1177/17446295209174]
- Kord Z, Shahani P, Dibirian A, Rasuli M, Zayeri F. [An audit of safety measures of pediatric wards (Persian)]. J Health Care. 2015; 17(3):218-29. [Link]
- Brooks Carthon JM, Hatfield L, Plover C, Dierkes A, Davis L, Hedgeland T, et al. Association of nurse engagement and nurse staffing on patient safety. J Nurs Care Qual. 2019; 34(1):40. [DOI:10.1097/NCQ.0000000000000334] [PMID]
- Hockenberry MJ, Wilson D. Wong’s nursing care of infants and children-E-book. Amsterdam: Elsevier Health Sciences; 2018. [Link]
- Gillham B, Thompson J. Child safety: Problem and prevention from pre-school to adolescence: A handbook for professionals. Oxfordshire: Taylor & Francis; 2005. [Link]
- WHO. Promoting safety of medicines for children. Geneva: World Health Organization; 2007. [Link]
- McMahon AW, Dal Pan G. Assessing drug safety in children-the role of real-world data. N Engl J Med. 2018; 378(23):2155-7.[DOI:10.1056/NEJMp1802197] [PMID]
- Kaufmann J, Wolf AR, Becke K, Laschat M, Wappler F, Engelhardt T. Drug safety in paediatric anaesthesia. Br J Anaesth. 2017; 118(5):670-9. [DOI:10.1093/bja/aex072] [PMID]
- Moavero R, Pisani LR, Pisani F, Curatolo P. Safety and tolerability profile of new antiepileptic drug treatment in children with epilepsy. Expert Opin Drug Saf. 2018; 17(10):1015-28. [PMID]
- Wei R, Jia LL, Yu YC, Nie XL, Song ZY, Fan DF, et al. Pediatric drug safety signal detection of non-chemotherapy drug-induced neutropenia and agranulocytosis using electronic healthcare records. Expert Opin Drug Saf. 2019; 18(5):435-41. [DOI:10.1080/14740338.2019.1604682] [PMID]
- Stang A, Thomson D, Hartling L, Shulhan J, Nuspl M, Ali S. Safe care for pediatric patients: A scoping review across multiple health care settings. Clin Pediatr. 2018; 57(1):62-75. [DOI:10.1177/0009922817691820] [PMID]
- Gates PJ, Baysari MT, Gazarian M, Raban MZ, Meyerson S, Westbrook JI. Prevalence of medication errors among paediatric inpatients: Systematic review and meta-analysis. Drug Saf. 2019; 42(11):1329-42. [DOI:10.1007/s40264-019-00850-1] [PMID]
- Alomari A, Wilson V, Solman A, Bajorek B, Tinsley P. Pediatric nurses’ perceptions of medication safety and medication error: A mixed methods study. Compr Child Adolesc Nurs. 2018; 41(2):94-110. [DOI:10.1080/24694193.2017.1323977] [PMID]
- Larose G, Levy A, Bailey B, Cummins-McManus B, Lebel D, Gravel J. Decreasing prescribing errors during pediatric emergencies: A randomized simulation trial. Pediatrics. 2017; 139(3):e20163200. [DOI:10.1542/peds.2016-3200] [PMID]
- Walsh A, Booth R, Rajani K, Cochrane L, Peters M, du Pré P. Introduction of a prescribing ward round to reduce prescribing errors on a paediatric intensive care unit. Arch Dis Child Educ Pract Ed. 2021; 106(4):251-4. [DOI:10.1136/archdischild-2019-318732] [PMID]
- Mitchell R, Cavanagh M, Eager D. Not all risk is bad, playgrounds as a learning environment for children. Int J Inj Contr Saf Promot. 2006; 13(2):122-4. [DOI:10.1080/17457300500310269] [PMID]
- Clarke SP, Rockett JL, Sloane DM, Aiken LH. Organizational climate, staffing, and safety equipment as predictors of needlestick injuries and near-misses in hospital nurses. Am J Infect Control. 2002; 30(4):207-16. [DOI:10.1067/mic.2002.123392] [PMID]
- Ribeiro GDSR, Silva RCD, Ferreira MA, Silva GRD, Campos JF, Andrade BRP. Equipment failure: Conducts of nurses and implications for patient safety. Rev Bras Enferm. 2018; 71(4):1832-40. [DOI:10.1590/0034-7167-2016-0547] [PMID]
- Munnangi S, Dupiton L, Boutin A, Angus LDG. Burnout, perceived stress, and job satisfaction among trauma nurses at a level I safety-net trauma center. J Trauma Nurs. 2018; 25(1):4-13. [DOI:10.1097/JTN.0000000000000335] [PMID]
- Wang KY, Chou CC, Lai JC. A structural model of total quality management, work values, job satisfaction and patient-safety-culture attitude among nurses. J Nurs Manag. 2019; 27(2):225-32. [DOI:10.1111/jonm.12669] [PMID]
- Izadpanah F, Nikfar S, Bakhshi Imcheh F, Amini M, Zargaran M. Assessment of frequency and causes of medication errors in pediatrics and emergency wards of teaching hospitals affiliated to Tehran University of Medical Sciences (24 Hospitals). J Med Life. 2018; 11(4):299-305. [DOI:10.25122/jml-2018-0046] [PMID]
- Amiri M, Khademian Z, Nikandish R. The effect of nurse empowerment educational program on patient safety culture: A randomized controlled trial. BMC Med Educ. 2018; 18(1):158. [DOI:10.1186/s12909-018-1255-6] [PMID]
- Boamah SA, Spence Laschinger HK, Wong C, Clarke S. Effect of transformational leadership on job satisfaction and patient safety outcomes. Nurs Outlook. 2018; 66(2):180-9. [DOI:10.1016/j.outlook.2017.10.004] [PMID]
Article Type : Research |
Subject:
General
Received: 2020/11/27 | Accepted: 2023/06/26 | Published: 2023/06/20
Received: 2020/11/27 | Accepted: 2023/06/26 | Published: 2023/06/20
Send email to the article author
| Rights and permissions | |
 | This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
