

BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
URL: http://hnmj.gums.ac.ir/article-1-1387-en.html



2- Instructor, Department of Nursing, School of Nursing and Midwifery, Guilan University of Medical Sciences, Rasht, Iran , f.hasavari@gmail.com
3- Assistant Professor, Digestive and Liver Diseases Research Center of Guilan, Department of Nursing, School of Nursing and Midwifery, Guilan University of Medical Sciences, Rasht, Iran
4- Associate Professor, Social Determinants of Health Research Center (SDHRC), Biostatistics, Guilan University of Medical Sciences, Rasht, Iran
Introduction
he evolution of human life on earth suggests that the occurrence of most disasters is inevitable. Besides, environmental, demographic changes and manipulations have made this planet increasingly vulnerable to disasters [1]. Disasters are the serious disruption of the functioning of a society that results in widespread human, economic, or environmental damages; managing those is beyond the capacity of the community affected by reliance on domestic resources [2]. According to the Centre for Research on the Epidemiology of Disasters, 6873 natural disasters occurred between 1994 and 2013 worldwide [3].
Natural disasters have killed ≥3 million people worldwide and costed 500 billion dollars over the last 20 years [4]. Asia accounts for 40.7% of all natural disaster types and 90% of total casualties [5]. Iran, located in the Central Asian region with a population of >70 million, is also exposed to extensive natural and human-made crises [6].What matters most at the time of disaster is its management, a process that contributes to the preservation of human life, property, environmental stability, and the economic and political situation of the affected region, before and after the disaster.
The 4 main components of emergency management include mitigation, readiness, response, and recovery [7]. Amongmany disaster management agencies, the most crucial role is played by the healthcare centers. They are the main organization that a significantly impact disaster reduction by presenting disaster readiness strategies [8]. The nurses have always been a part of the disaster service provider team; thus, being prepared to provide different care at disasters tailored to its different stages is a nursing necessity [9-11].
Studies have highlighted the insufficient readiness of nurses to cope with disasters in Texas, USA [12], and their moderate readiness in Japan [13]. Another study exploring 757 nurses in the Asia-Pacific region indicated their poor readiness for disasters [14]. Numerous studies reflected the inadequatereadinessof nurses to manage disasters; however, the rate varies in different centers depending on the available resources and the management method [15-19]. Iran is among the world’s most disaster-prone countries, and few studies have been conducted in this filed in Iran. Accordingly, this study aimed to assess the disaster readiness of nurses in hospitals affiliated to Guilan University of Medical Sciences (GUMS) in North of Iran, Iran. The results may help to manage crisis and plan for greater readiness more accurately.
Materials and Methods
This across-sectional study was conducted from January to February 2018. The study population consisted of all nurses in 7 hospitals affiliated to GUMS in Rasht, Iran (N=1580). The sampling was conducted using a systematic stratified random sampling technique and based on the study inclusion criteria (working full-time as a nurse and having at least a bachelor’s degree). The sample size was determined as 187 according to the mean level of disaster readiness (36.88) reported in the study of Maeda et al. and considering the relative error of 2.5% and 95% confidence interval [13].
The required data were collected using a two-part questionnaire: the first part was a demographic/occupational form surveying age, gender, education level, marital status, work sector, employment status, work experience, job position, willingness to dispatch, disaster care delivery experience, a history of attendance in a disaster management course, the number of attendances in a disaster management course, the time of attendance in a disaster management course, a history of participation in maneuvers related to the training course, and the duration of participation in maneuvers. The second part was Readiness Estimate & Deployability Index (READI).
It is a self-report scale that measures the level of individual deployment readiness. It was first designed by Reineck in 1996 to assess deployment readiness in US Army Nurse Corps officers. Later, its’ Japanese version was designed by Maeda et al. to measure the disaster readiness of nurses working in hospitals [13, 15]. It has 48 items and 7 subscales of clinical competency (29 items), operational competence (3 items), survival skills (2 items), stress coping (4 items), leadership and administrative support (2 items), mental attitude (6 items), as well as group integration and identification (2 items). The items are rated on a 5-point Likert-type scale, where the total score ranges 48-240.
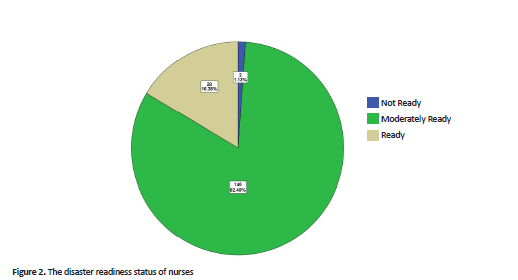
For overall preparation and preparation in each domain, the mean score was calculated. To determine the status of preparation, the total score of the questions was divided by the number of questions that ranged 1-5. Then, the samples were categorized based on the obtained scores in three levels: not ready (score 1-2), moderately ready (score 2-4), and ready (score 4-5).
Due to the lack of the Persian version of READI, it was translated to Persian using a back-translation method according to the opinions of 15 Academic members. Then, its Content Validity Ratio (CVR) and Content Validity Index (CVI) were calculated. To evaluate the tool’s reliability, a 2-week pilot study was conducted on 20 nurses with similar characteristics to the study samples. The total Intra class Correlation Coefficient (ICC) was obtained at to be 0.96. For clinical competency, ICC=0.96; operational competency, ICC=0.94; survival skills, ICC=0.94; stress coping, ICC=0.96; leadership and administrative support, ICC=0.99; mental attitude, ICC=0.96; as well as group integration and identification, ICC=0.92 were considered.
After reviewing the professors' opinions, the lowest CVR value was 0.6 and the highest value was 1, which according to the Lavasheh table (0.49) in terms of necessity, all expressions had the necessary validity. The CVI index was used to check the simplicity, relevance, and clarity of the questions; the CVI ranged from 0.73 to 1. Regarding the questions 2, 21, 46, their CVI was between 0.7 and 0.8, which were seriously reviewed. For questions 1, 3, 6, 7, 9, 15, 17, 25, 30, 40, the obtained CVI was calculated between 0.8 and 0.9, which were reviewed in detail. For the rest of the questions, the CVI obtained was above 0.9, which was used directly in the questionnaire.
Of 187 distributed questionnaires, 10 returned incomplete; thus, there were excluded from the study. The collected data were analyzed in SPSS using descriptive statistics (frequency, mean, & standard deviation).
Results
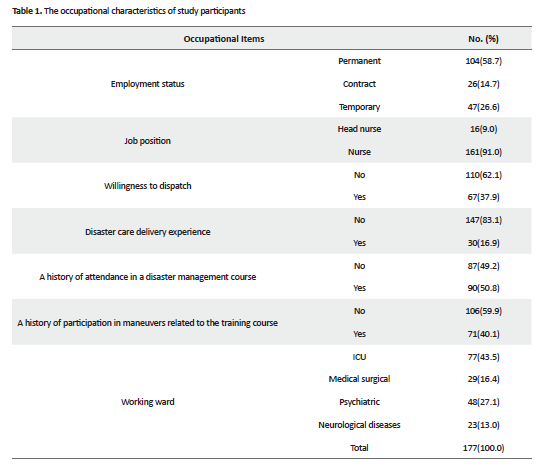
Most of the study participants were female (95.5%), aged 31-40 years (41.2%), with a Mean±SD age of 33.77±7.70 years. Moreover, 65% of them were married, with a bachelor’s degree (90.4%), work experience of 6-15 years (47.5%) with a Mean±SD value of 9.92±6.96 years, and weekly working hours of 40-60 hours (45.8%) with a mean value of 50.02±19.51 hours. The occupational characteristics of the study participants are presented in Table 1.
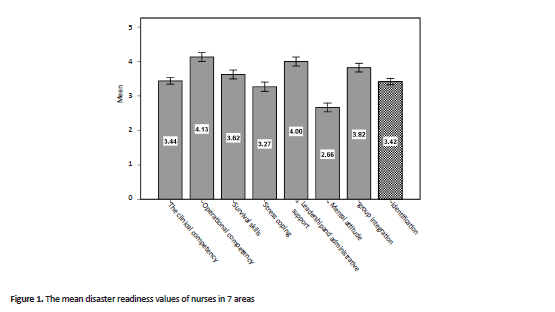
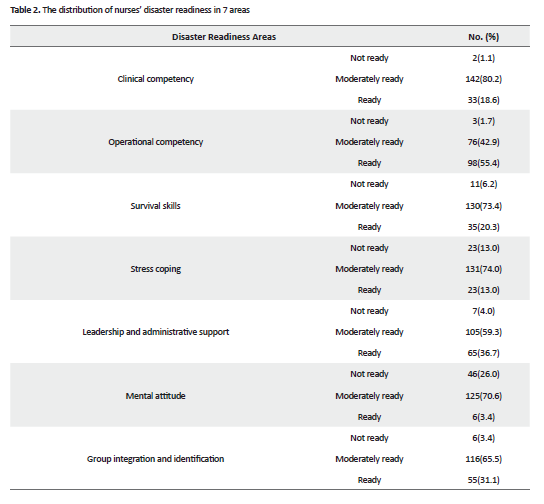
To the obtained READI data revealed that the Mean±SD score of total disaster readiness for the study samples was 3.42±0.60 (Figure 1). Furthermore, the majority of samples were moderately ready in this regard (Figure 2). The Mean±SD scores of READI dimensions for disaster readiness in the areas of clinical competency, operational ompetency, survival skills, stress coping, leadership and administrative support, mental attitude, as well as group integration and identification were 3.44±0.65, 4.13±0.87, 3.62±0.87, 3.27±0.91, 4±0.88, 2.66±0.85, and, 3.82±0.85, respectively. In addition, the highest readiness level of nurses was in the area of operational competency, and the lowest level belonged to their mental attitude. In all areas, the disaster readiness of nurses was at a moderate level, except for the area of operational competency, which was high (sufficient) (Table 2). Moreover, the highest mean values of disaster readiness were related to correctly placing the ECG leads on patients’ chest (4.45±0.90) belonged to the subscale of operational competence; however, the lowest mean score was related to caring the patient with chemical, biological, radiological, nuclear, and explosive damage (2.23±1.04) belonged to the subscale of clinical competency.
Discussion
The obtained data suggested that the studied nurses’ preparedness for disasters was at a moderate level. This finding is consistent with those of Maeda et al. [13] in Japan, Tabiee et al. [20] in Iran, Yana et al. [21] in China, and Xu et al. [22] in Taiwan. However, our finding was inconsistent with those of Matlock [23] in Arkansas, USA, and Whetzel et al. [24]. This discrepancy may be due to the differences in measurement tools.
The highest mean score of nurses’ disaster readiness was in the aspect of operational competence; therefore, they were appropriately ready to respond to disasters in this area. According to Tabiee et al. [20], nurses’ disaster readinessin this area was at a moderate level. The low readiness level in this area has also been reported in some other studies [24, 25]. Such data differences and the higher mean score achieved in the present study might be due to the employment of a large number of nurses in the Intensive Care Units (ICUs). This is because it is a specialized area where patients with life-threatening acute diseases are treated by the most skilled treatment staff [26].
Nurses working in the ICUs have adequate knowledge and awareness of the physiological warning signs. Besides, they could respond to rapid changes in the patient’s condition. They are also skilled in clinical practice, strong in teamwork, and confident in their actions to evaluate patient data and enhance interventions required for care [27, 28].
In terms of READI components, the highest mean value of readiness level was related to correctly placing the ECG leads on patients’ chest belonged to the operational competence subscale, i.e., in agreement with the study of Maeda et al. [13]. This procedure seems to be among the most frequently repeated measures of nursing, and the highest mean score in this area was expected. The lowest mean of disaster readiness was observed in caring for the patient with chemical, biological, radiological, nuclear, and explosive damage that belonged to the clinical competency.
Maeda et al. [13] also reported the lowest score of disaster readiness in this area; however, in the study of Wilmoth et al. [29], the disaster readiness level of samples was higher in this aspect. This discrepancy might be due to the differences in the study samples. The current study samples were only nurses, while in their study, the disaster readiness of physicians was examined in addition to nurses. Furthermore, patients presenting chemical, biological, radiological, nuclear, and explosive damage are rare to be encountered by a nurse during employment.
Additionally, the studied nurses had the lowest mean of disaster readiness in the area of mental attitude, where they were moderately ready. This is consistent with the study of Rivers et al. [26] but against the results of Stevenson et al. [15]. This discrepancy might be because, in our study, most of the studied samples had no experience of providing disaster care, while in the study of Stevenson et al., samples were air-force nurse anesthetists who had experiences of stressful situations. The present study addressed providing nursing care to terrorists, having tedious shifts, bad weather, and the ability of nurses to adapt to sleeping in times of disaster with mass casualties. According to Usuzawa et al. [30], repeated exposure to a stimulus affects the attitude towards it. Therefore, the lack of disaster care experience has influenced the disaster readiness of nurses in our study.
The study questionnaires were completed in the wards and during the nursing service; therefore, location, time, and environmental stressors may have affected their response as a study limitation. Although the present study examined the status of nurses’ preparedness to cope with the disaster, the involvement of all affiliated groups in the medical profession is required. In this regard, more studies are recommended for disaster readiness assessment of all medical staff using the READI tool.
Ethical Considerations
Compliance with ethical guidelines
This study was extracted from a Master’s thesis approved by the Research Ethics Committee of GUMS (code: IR.GUMS.REC.1396.397). Before collecting the required data, the study objectives and methods were explained to the study participants, and they all signed an informed consent form. They were assured of the confidentiality of their achieved information.
Funding
This study received financial support from the Social Determinants of Health Research Center.
Authors contributions
Conceptualization: Maryam Jamaili, Farideh Hasavari, and Farahnaz Jokar; Writing and Data Analysis: Farideh Hasavari; Investigation and Data Analysis: Maryam Jamaili; Data Analysis: Farahnaz Jokar and Ehsan Kazemnezhad Leili. Confirmation of this manuscription was done by all authors
Conflict of interest
The authors declared no conflicts of interest.
Acknowledgements
The authors would like to thank the Deputy for Research and Technology of GUMS, Social Determinants of Health Research Center, Shahid Beheshti School of Nursing and Midwifery, and all study participants for their valuable support and cooperation.
References
- Koenig KL, Schultz CH, editors. Koenig and Schultz’s disaster medicine: Comprehensive principles and practices. Cambridge: Cambridge University Press; 2011. [DOI:10.1017/CBO9780511902482]
- Ardalan A, Rajaei MH, Azin A, Zenoubi V, Sarband H. [Terminology of disaster risk reduction (Persian)]. Tehran: Ministry of Health and Medical Education, Department of Health; 2013.
- Hossain A, Ray SK, Sinha R. A smartphone-assisted post-disaster victim localization method. Paper presented at: 18th International Conference on High Performance Computing and Communications; IEEE 14th International Conference on Smart City; IEEE 2nd International Conference on Data Science and Systems (HPCC/SmartCity/DSS). 12-14 December 2016; Sydney, NSW, Australia. [DOI:10.1109/HPCC-SmartCity-DSS.2016.0164]
- Gladston S, Nayak R. Disaster preparedness among nurses working in a paediatric acute care setting of a tertiary hospital, South India. Journal of Nursing and Health Science. 2017; 6(2):55-9.
- Berhanu N, Abrha H, Ejigu Y, Woldemichael K. Knowledge, experiences, and training needs of health professionals about disaster preparedness and response in southwest Ethiopia: A cross sectional study. Ethiopian Journal of Health Sciences. 2016; 26(5):415-26. [DOI:10.4314/ejhs.v26i5.3] [PMID] [PMCID]
- Bahrami M, Aliakbari F, Aein F. [Team work competence in disaster response: An explorative study about emergency nurses experiences: A qualitative content analysis study (Persian)]. Journal of Clinical Nursing and Midwifery. 2014; 2(4):26-36.
- Shahraki Vahed A, Abbaszadeh A, Ardalan A, Haghighi M. [Health management in disasters (Persian)]. Tehran: Jame-e-Negar; 2014.
- Daneshmandi M, Nezamzadeh M, Zareiyan A. [Assessment the preparedness of selected hospital to deal with disasters in Tehran (Persian)]. Journal of Military Caring Sciences. 2014; 1(1):28-35. [DOI:10.18869/acadpub.mcs.1.1.28]
- Usher K, Redman-MacLaren ML, Mills J, West C, Casella E, Hapsari ED, et al. Strengthening and preparing: Enhancing nursing research for disaster management. Nurse Education in Practice. 2015; 15(1):68-74. [DOI:10.1016/j.nepr.2014.03.006] [PMID]
- Ardalan A, Khankeh HR, Nejati A, Masoumi GR, Hajebi A, Mohammadi H, et al. [Textbook health in emergencies and disasters (Persian)]. Soorani M, Salemi S, Nasiri A, editors. Tehran: Mehr-e Ravash; 2016.
- Al Thobaity A, Plummer V, Innes K, Copnell B. Perceptions of knowledge of disaster management among military and civilian nurses in Saudi Arabia. Australasian Emergency Nursing Journal. 2015; 18(3):156-64. [DOI:10.1016/j.aenj.2015.03.001] [PMID]
- Baack S, Alfred D. Nurses’ preparedness and perceived competence in managing disasters. Journal of Nursing Scholarship. 2013; 45(3):281-7. [DOI:10.1111/jnu.12029] [PMID]
- Maeda T, Kotera S, Matsuda N, Edwards GD. Disaster readiness among nurses in Japan: Current status following the great east Japan earthquake. International Journal of Nursing. 2016; 3(1):15-28.
- Usher K, Mills J, West C, Casella E, Dorji P, Guo A, et al. Cross‐sectional survey of the disaster preparedness of nurses across the Asia-Pacific region. Nursing & Health Sciences. 2015; 17(4):434-43. [DOI:10.1111/nhs.12211] [PMID]
- Stevenson MA, Scholes RB, Dremsa TL, Austin PN. Readiness estimate and deployability index for air force nurse anesthetists. Military Medicine. 2007; 172(1):36-9. [DOI:10.7205/MILMED.172.1.36] [PMID]
- Tzeng WC, Feng HP, Cheng WT, Lin CH, Chiang LC, Pai L, et al. Readiness of hospital nurses for disaster responses in Taiwan: A cross-sectional study. Nurse Education Today. 2016; 47:37-42. [DOI:10.1016/j.nedt.2016.02.025] [PMID]
- Öztekin SD, Larson EE, Akahoshi M, Öztekin İ. Japanese nurses’ perception of their preparedness for disasters: Quantitative survey research on one prefecture in Japan. Japan Journal of Nursing Science. 2016; 13(3):391-401. [DOI:10.1111/jjns.12121] [PMID]
- Nash TJ. Unveiling the truth about nurses’ personal preparedness for disaster response: A pilot study. Medsurg Nursing. 2015; 24(6):425-31. [PMID]
- Alshehri B. Emergency nurses’ preparedness for disaster in the Kingdom of Saudi Arabia. Journal of Nursing Education and Practice. 2017; 7(3):101-14. [DOI:10.5430/jnep.v7n3p101]
- Tabiee Sh, Nakhaei M. Nurses’ preparedness for disaster in South Khorasan Province, Iran. Health in Emergencies & Disasters Quarterly. 2016; 2(1):13-8. [DOI:10.18869/nrip.hdq.2.1.13]
- Yana Y, Luo Y, Liu X. Investigation on disaster response capacity of community nurses and the influencing factors. Journal of Nursing Science. 2011; 1:007.
- Xu XH, Sheng Y, Li Z, Wang QY, Wang QB, Cai MX, et al. A cross-sectional survey of the disaster preparedness of nurses in China. Chinese Journal of Nursing. 2016; (8):002. http://en.cnki.com.cn/Article_en/CJFDTotal-ZHHL201608002.htm
- Matlock T. Emergency preparedness competencies among nurses in Northwest Arkansas [BSc. thesis]. Fayetteville, AR: University of Arkansas; 2017.
- Whetzel E, Walker-Cillo G, Chan GK, Trivett J. Emergency nurse perceptions of individual and facility emergency preparedness. Journal of Emergency Nursing. 2013; 39(1):46-52. [DOI:10.1016/j.jen.2011.08.005] [PMID]
- Kovats K, Morris M, Reineck C, Finstuen K. Nursing readiness: Active duty vs. army reserve. US Army Medical Department Journal PB 8-01-7/8. 2001; 9:30-8.
- Rivers FM, Wertenberger DH, Lindgren K. U.S. Army Professional Filler System nursing personnel: Do they possess competency needed for deployment? Military Medicine. 2006; 171(2):142-9. [DOI:10.7205/MILMED.171.2.142] [PMID]
- Rajkomar A, Blandford A. Understanding infusion administration in the ICU through distributed cognition. Journal of Biomedical Informatics. 2012; 45(3):580-90. [DOI:10.1016/j.jbi.2012.02.003] [PMID]
- Khoeiniha F, Sheikhi MR, Shokati Ahmadabad M, Mohammadpoor Asl A. [Nurses’ clinical performance assessment in critical care units in teaching and non-teaching hospitals in Qazvin City: Based on synergy model (Persian)]. Journal of Health Promotion Management. 2016; 5(3):28-36.
- Wilmoth MC, De Scisciolo S, Gilchrest LJ, Dmochowski J. The readiness estimate and deployability index and psychometric properties in army reserve nurses and medics. Military Medicine. 2007; 172(8):800-5. [DOI:10.7205/MILMED.172.8.800] [PMID]
- Usuzawa M, Telan EO, Kawano R, Dizon CS, Alisjahbana B, Ashino Y, et al. Awareness of disaster reduction frameworks and risk perception of natural disaster: A questionnaire survey among Philippine and Indonesian health care personnel and public healthstudents. The Tohoku Journal of Experimental Medicine. 2014; 233(1):43-8. [DOI:10.1620/tjem.233.43] [PMID]
Received: 2020/03/30 | Accepted: 2020/03/30 | Published: 2020/03/30
| Rights and permissions | |
 | This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Articles Copyright © The Author(s).
Owned by Guilan University of Medical Sciences.
Co-published by Negah Institute for Scientific Communication.
Contact Information
JHNM Office, Guilan University of Medical Sciences P.O.Box 41635-1873, Rasht, Iran
Journal Tel: +9813 33553202
Publisher Tel: +9821 453 55 555; +9821 453 55 000
Email: holisticnmj@gmail.com, nursjournal@gums.ac.ir
