Wed, Apr 24, 2024
Volume 29, Issue 3 (6-2019)
JHNM 2019, 29(3): 167-175 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Jalali N, Hadavand S, Jafari F, Rabiee M, Khajavi Shojaie K. Pregnant Women’s Views on the Type of Delivery: Determinants and Relationships. JHNM 2019; 29 (3) :167-175
URL: http://hnmj.gums.ac.ir/article-1-1079-en.html
URL: http://hnmj.gums.ac.ir/article-1-1079-en.html



1- Medical Student, School of Medicine, Shahed University, Tehran, Iran
2- Assistant Professor, Gynecologist and Obstetrician, Department of Obstetrics and gynecology, School of Medicine, Shahed University, Tehran, Iran.
3- Associate Professor, Department of Health and Social Medicine, School of Medicine, Shahed University, Tehran, Iran
4- Assistant Professor, Gynecologist and Obstetrician, Department of Obstetrics and gynecology, School of Medicine, Shahed University, Tehran, Iran
5- Instructor, Department of Health and Social Medicine, School of Medicine, Shahed University, Tehran, Iran , prskhajavi@yahoo.com
2- Assistant Professor, Gynecologist and Obstetrician, Department of Obstetrics and gynecology, School of Medicine, Shahed University, Tehran, Iran.
3- Associate Professor, Department of Health and Social Medicine, School of Medicine, Shahed University, Tehran, Iran
4- Assistant Professor, Gynecologist and Obstetrician, Department of Obstetrics and gynecology, School of Medicine, Shahed University, Tehran, Iran
5- Instructor, Department of Health and Social Medicine, School of Medicine, Shahed University, Tehran, Iran , prskhajavi@yahoo.com
Full-Text [PDF 449 kb]
(703 Downloads)
| Abstract (HTML) (2453 Views)
Full-Text: (998 Views)
Introduction
Maternity delivery is one of the most important health care services in all countries [1], and the increase in unnecessary or elective Cesarean Section (CS) is not a good indicator for countries’ health care systems. The World Health Organization (WHO) recommended a maximum CS of 15% with good indication up to 2010 [1-5]. In recent years, CS rates have risen rapidly in all countries, reaching from 20.7% in 1996 to 31.1% in 2006 in the US; while in 2004, the CS rate was 37% in Italy, 35% in Korea, and 25% in Canada [6].
According to 2010 WHO report, the rate of CS in Iran was 41.9% of the total number of deliveries in 2008, which is the second highest growth rate in the world after Brazil [7]. In 2009, the CS rate in Iran was 47.9% [8, 9] and in 2013 it reached 52-54% (second in the world) which indicates its unfavorable situation [10, 11]. Evidence has shown that the CS rate increase greater than 15% have not led to a reduction in the mortality of the mother and the baby [12]. Previous studies have highlighted potential causes for the increasing CS rate, including mother’s request [12, 13], legal and ethical issues [13-15], obesity [16, 17], and increased maternal age [18-20].
Elective CS has advantages such as decreased stillbirth, reduced cerebral palsy, reduced bone fractures, delivery schedules, and shorter labor. However, like any operation it has complications such as wound site infection, pelvic infections, pulmonary infection, urinary tract infection, pulmonary embolism, vein thrombosis, and some complications of anesthesia; so maternal and neonatal mortality and morbidity in CS is more than in normal delivery [21, 22]. Studies also show that financial costs, length of hospital stay, drug use, and possible side effects of drugs are significantly higher in CS than in normal delivery [23-25]. Furthermore, recent studies have shown that CS has an adverse effect on fertility, weight of the neonates, and early neonatal injuries. It also causes postpartum depression [26-28].
The lack of knowledge of women about the complementary ways of normal delivery and the fear of labor pain are the main reasons women refuse to have a normal delivery. Today CS is not used only in emergencies and for saving the lives of the mother and the baby, but in some societies, it is gradually becoming a luxury gesture [25, 29, 30]. According to the theory of reasoned action, the intention is the main determinant of behavior which is a combination of mental attitudes and norms toward behavior. Each person’s attitude to personal experiences is created by different situations which determine the person’s perspective on the world and him/herself. It also determines the type of person’s behavior in different situations, which can be changed from negative to positive by study, knowledge, and practice [31, 32].
Considering what was discussed, we aimed to determine the factors associated with the preference for the delivery mode in pregnant women referred to prenatal care clinic of a hospital in Tehran towards the type of delivery.
Materials and Methods
This study was an analytical cross-sectional study conducted in one of the hospitals in Tehran City, Iran. The study population consisted of all pregnant women referred to the prenatal care clinic of the hospital. Of them, 400 samples including nulliparous and multiparous pregnant women in their third trimester without any obstetric diseases were selected using convenience sampling method. According to sample size formula at 95% confidence interval (z1-α/2=1.96, α=0.05) and considering error (d)=0.05 and the variance of the mean score for the viewpoints of pregnant women about the type of delivery (s2=0.25) obtained based on the preliminary study on 30 subjects, the sample size was determined as 385. To be on the safe side, the number increased to 400.
The study data were collected in 2016 using a questionnaire based on the one designed by Mohammadpourasl et al. [5]. This questionnaire has been used in other studies, too [33]. It has questions about demographic and obstetric characteristics and the preference of pregnant women for delivery mode. The preference part has been rated based on a 5-point Likert-type scale ranged from “completely agree” to “completely disagree”. In positive questions, the scoring is as following: “completely agree” +2, “agree” +1, “disagree” -1, “completely disagree” -2, and “no idea” 0. For negative questions, reverse scoring was used. The total score ranged from +44 to -44.
To determine the validity of the questionnaire, it was sent to the faculty members of the School of Social Medicine, and necessary corrections were made based on their opinions in terms of face and content validity. For its internal consistency, a Cronbach alpha of 0.7 was obtained. For estimating the reliability of the questionnaire, test-retest reliability was performed on 20 samples, and a correlation coefficient of 0.82 was obtained. To analyze the scores, the total score obtained from the participants was divided into four levels of very good, good, fair, and unfavorable based on a mean and Standard Deviation (SD) of ±2. Two SDs higher than the mean denoted very good level, one SD greater than the mean referred to good level, equal to the mean was moderate level, and less than the mean was unfavorable level. It should be mentioned that, before collecting data, verbal consent was obtained from the participants. The collected data were analyzed in SPSS V. 16 using the Pearson correlation, the Chi-squared test and t-test. The ethical code for this study was obtained from the Research Ethics Committee (IR.shahed.REC.1394.104).
Results
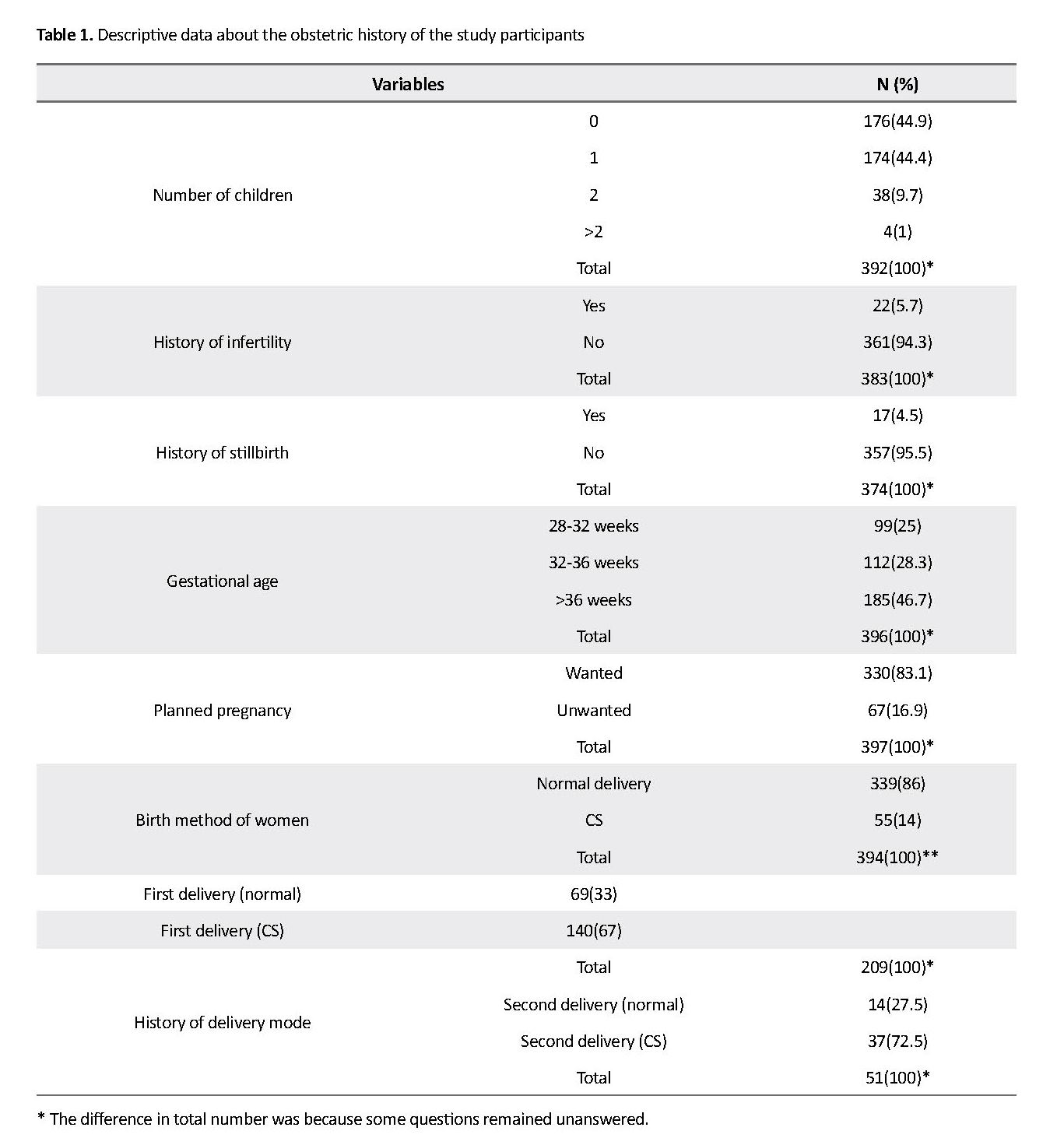
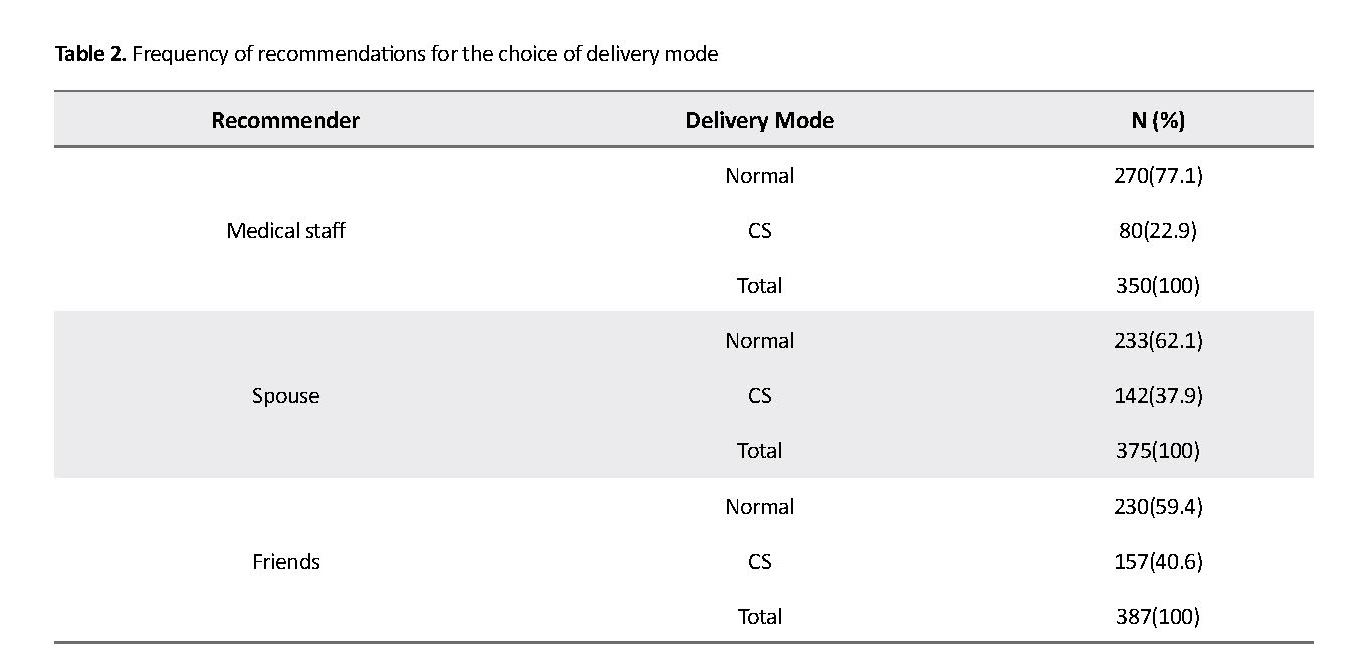
The Mean±SD age of the women was 30.43±4.93 years ranging between 18 and 43 years. Regarding occupation, 17.2% were employee, 65.8% housewives, 7.8% students, and 9% other occupations. Regarding education, 55.2% had a university education, 43.2% high school education; 1% middle school education, and 0.2% elementary education. Regarding income, 17.2% earned over $600 monthly, 61.8% between $300 and $600 monthly, and 17.5% less than $300. Table 1 presents descriptive data about the obstetric history of the study participants. The collected data showed that 59% (n=198) preferred normal delivery and 41% (n=136) CS. In 77.1% of samples, the medical staff recommended natural childbirth, and the most recommendations for CS (40.6%) was from friends.
Maternity delivery is one of the most important health care services in all countries [1], and the increase in unnecessary or elective Cesarean Section (CS) is not a good indicator for countries’ health care systems. The World Health Organization (WHO) recommended a maximum CS of 15% with good indication up to 2010 [1-5]. In recent years, CS rates have risen rapidly in all countries, reaching from 20.7% in 1996 to 31.1% in 2006 in the US; while in 2004, the CS rate was 37% in Italy, 35% in Korea, and 25% in Canada [6].
According to 2010 WHO report, the rate of CS in Iran was 41.9% of the total number of deliveries in 2008, which is the second highest growth rate in the world after Brazil [7]. In 2009, the CS rate in Iran was 47.9% [8, 9] and in 2013 it reached 52-54% (second in the world) which indicates its unfavorable situation [10, 11]. Evidence has shown that the CS rate increase greater than 15% have not led to a reduction in the mortality of the mother and the baby [12]. Previous studies have highlighted potential causes for the increasing CS rate, including mother’s request [12, 13], legal and ethical issues [13-15], obesity [16, 17], and increased maternal age [18-20].
Elective CS has advantages such as decreased stillbirth, reduced cerebral palsy, reduced bone fractures, delivery schedules, and shorter labor. However, like any operation it has complications such as wound site infection, pelvic infections, pulmonary infection, urinary tract infection, pulmonary embolism, vein thrombosis, and some complications of anesthesia; so maternal and neonatal mortality and morbidity in CS is more than in normal delivery [21, 22]. Studies also show that financial costs, length of hospital stay, drug use, and possible side effects of drugs are significantly higher in CS than in normal delivery [23-25]. Furthermore, recent studies have shown that CS has an adverse effect on fertility, weight of the neonates, and early neonatal injuries. It also causes postpartum depression [26-28].
The lack of knowledge of women about the complementary ways of normal delivery and the fear of labor pain are the main reasons women refuse to have a normal delivery. Today CS is not used only in emergencies and for saving the lives of the mother and the baby, but in some societies, it is gradually becoming a luxury gesture [25, 29, 30]. According to the theory of reasoned action, the intention is the main determinant of behavior which is a combination of mental attitudes and norms toward behavior. Each person’s attitude to personal experiences is created by different situations which determine the person’s perspective on the world and him/herself. It also determines the type of person’s behavior in different situations, which can be changed from negative to positive by study, knowledge, and practice [31, 32].
Considering what was discussed, we aimed to determine the factors associated with the preference for the delivery mode in pregnant women referred to prenatal care clinic of a hospital in Tehran towards the type of delivery.
Materials and Methods
This study was an analytical cross-sectional study conducted in one of the hospitals in Tehran City, Iran. The study population consisted of all pregnant women referred to the prenatal care clinic of the hospital. Of them, 400 samples including nulliparous and multiparous pregnant women in their third trimester without any obstetric diseases were selected using convenience sampling method. According to sample size formula at 95% confidence interval (z1-α/2=1.96, α=0.05) and considering error (d)=0.05 and the variance of the mean score for the viewpoints of pregnant women about the type of delivery (s2=0.25) obtained based on the preliminary study on 30 subjects, the sample size was determined as 385. To be on the safe side, the number increased to 400.
The study data were collected in 2016 using a questionnaire based on the one designed by Mohammadpourasl et al. [5]. This questionnaire has been used in other studies, too [33]. It has questions about demographic and obstetric characteristics and the preference of pregnant women for delivery mode. The preference part has been rated based on a 5-point Likert-type scale ranged from “completely agree” to “completely disagree”. In positive questions, the scoring is as following: “completely agree” +2, “agree” +1, “disagree” -1, “completely disagree” -2, and “no idea” 0. For negative questions, reverse scoring was used. The total score ranged from +44 to -44.
To determine the validity of the questionnaire, it was sent to the faculty members of the School of Social Medicine, and necessary corrections were made based on their opinions in terms of face and content validity. For its internal consistency, a Cronbach alpha of 0.7 was obtained. For estimating the reliability of the questionnaire, test-retest reliability was performed on 20 samples, and a correlation coefficient of 0.82 was obtained. To analyze the scores, the total score obtained from the participants was divided into four levels of very good, good, fair, and unfavorable based on a mean and Standard Deviation (SD) of ±2. Two SDs higher than the mean denoted very good level, one SD greater than the mean referred to good level, equal to the mean was moderate level, and less than the mean was unfavorable level. It should be mentioned that, before collecting data, verbal consent was obtained from the participants. The collected data were analyzed in SPSS V. 16 using the Pearson correlation, the Chi-squared test and t-test. The ethical code for this study was obtained from the Research Ethics Committee (IR.shahed.REC.1394.104).
Results
The Mean±SD age of the women was 30.43±4.93 years ranging between 18 and 43 years. Regarding occupation, 17.2% were employee, 65.8% housewives, 7.8% students, and 9% other occupations. Regarding education, 55.2% had a university education, 43.2% high school education; 1% middle school education, and 0.2% elementary education. Regarding income, 17.2% earned over $600 monthly, 61.8% between $300 and $600 monthly, and 17.5% less than $300. Table 1 presents descriptive data about the obstetric history of the study participants. The collected data showed that 59% (n=198) preferred normal delivery and 41% (n=136) CS. In 77.1% of samples, the medical staff recommended natural childbirth, and the most recommendations for CS (40.6%) was from friends.
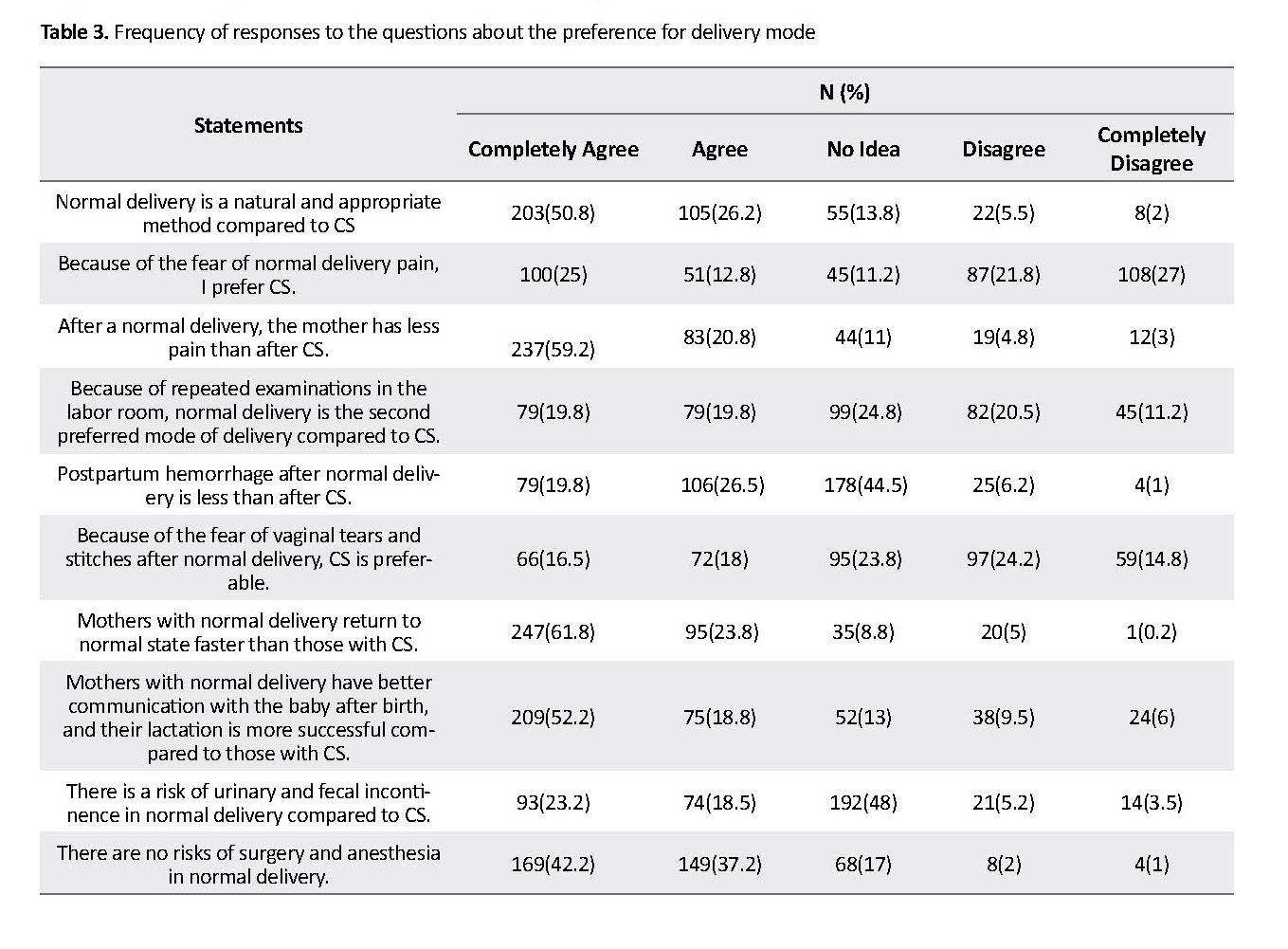
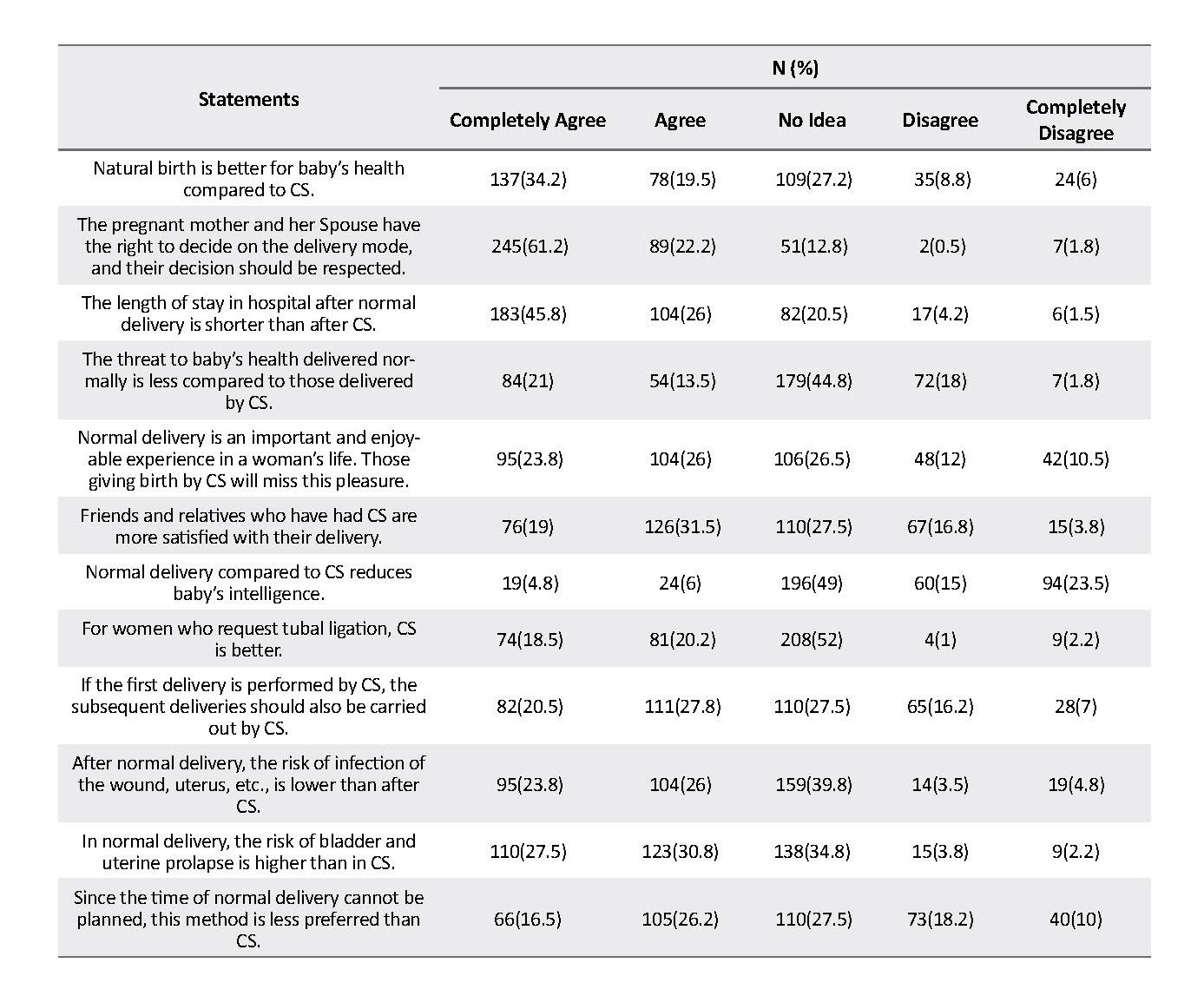
Table 2 presents information about the recommendations for the choice of delivery mode. Only 13.5% of participants completed childbirth education classes; 22.8% had incomplete participation, and 63.5% had not participated in these classes. Of those who took part in these classes, 40.2% considered these training effective, and 59.8% considered it useless. In response to the question: “if there was a better method to reduce or eliminate normal labor pain, would you prefer this method to CS?” 67.5% answered “yes”, and 28.5% said “no”. Table 3 presents the frequency of responses to the questions about the preference for delivery mode.
The mean score of the pregnant women participated in this study was 9.7±1.2 with a maximum score of 34 and a minimum of -19. The Kolmogorov-Smirnov test results showed that the scores had a normal distribution. By using the Pearson correlation test, a negative correlation was observed between the mothers’ scores (P=0.001, r=-0.6) and delivery mode, i.e. those with higher scores did not prefer CS. The t-test results showed a difference between the two groups with a tendency towards normal delivery and CS (P<0.05).
The mean score of the pregnant women participated in this study was 9.7±1.2 with a maximum score of 34 and a minimum of -19. The Kolmogorov-Smirnov test results showed that the scores had a normal distribution. By using the Pearson correlation test, a negative correlation was observed between the mothers’ scores (P=0.001, r=-0.6) and delivery mode, i.e. those with higher scores did not prefer CS. The t-test results showed a difference between the two groups with a tendency towards normal delivery and CS (P<0.05).
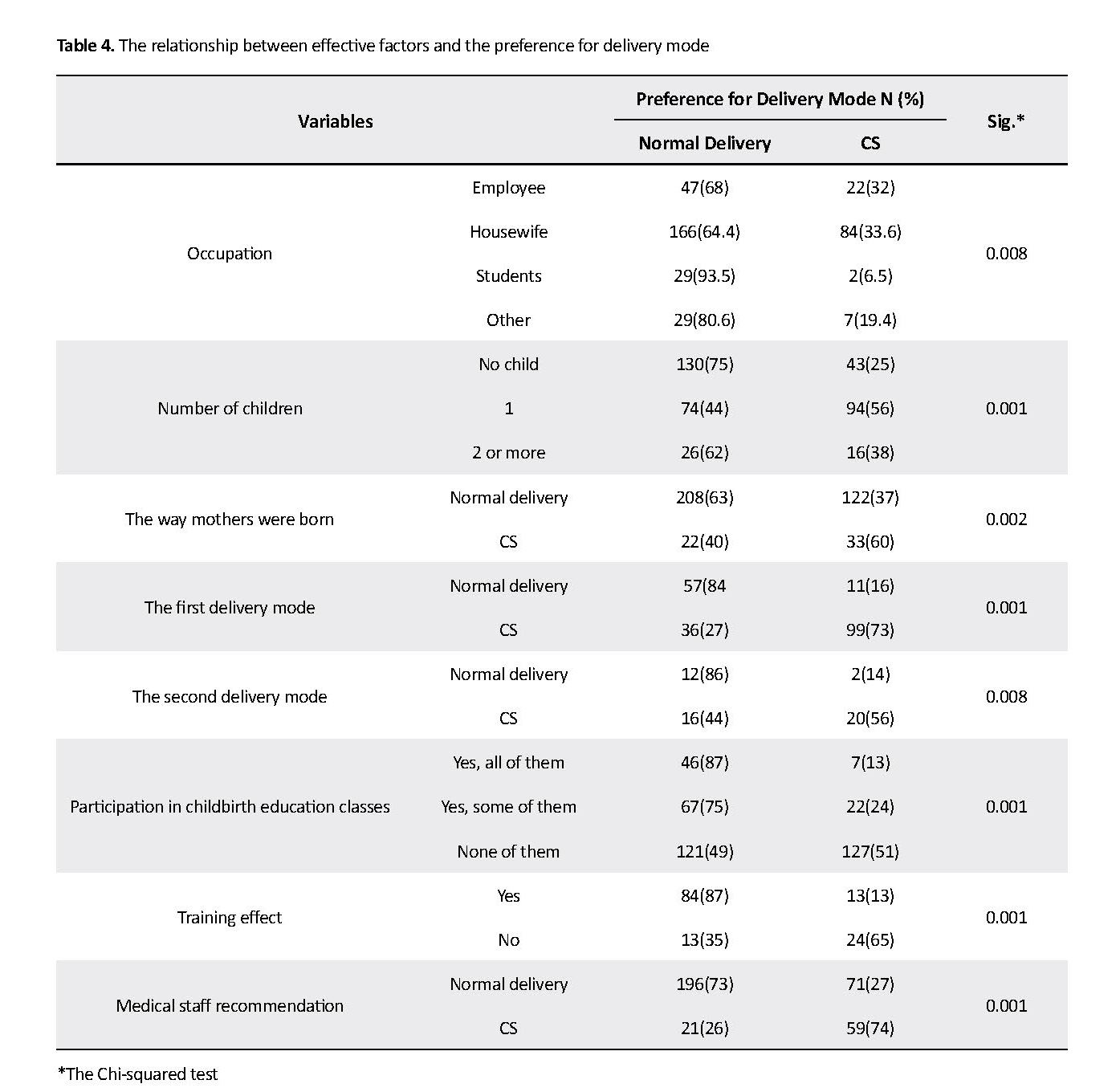
The history of infertility, the wanted or unwanted pregnancy, and the history of stillbirth had no relationship with the preference of delivery mode in the participants. However, the mother’s preference for delivery mode had a significant correlation with their occupation, education, number of children, method of their birth, first delivery method, second delivery method, participation in childbirth education classes, training effect, medical staff recommendation, Spouse’s recommendation, and advice of friends and relatives (Table 4).
Discussion
Based on the findings of this study, the CS preference rate in this study was about 41% which is relatively high. In the study of Pourheydari et al., and Fathollahi et al. these rates were reported 63.2% and 47%, respectively [34, 35]. The lower rate reported in our study can be due to changes in the health policies of the country and planning to reduce the rate of CS. According to Leone et al. study, social interaction and exchanging reproductive health information can reduce the rate of CS [36]. This result is impressive concerning the theory of social propagation about accepting peers behaviors. Our study showed that the majority of pregnant women had a positive attitude towards normal delivery and earned higher scores and thus preferred normal delivery which is consistent with the findings of Pourheydari et al. [34], but different from the results of Shahraki-Sanavi et al. [4]. This difference can be attributed to the time interval between two studies, cultural differences, or the experiences of samples from their previous delivery.
Based on the findings of this study, the CS preference rate in this study was about 41% which is relatively high. In the study of Pourheydari et al., and Fathollahi et al. these rates were reported 63.2% and 47%, respectively [34, 35]. The lower rate reported in our study can be due to changes in the health policies of the country and planning to reduce the rate of CS. According to Leone et al. study, social interaction and exchanging reproductive health information can reduce the rate of CS [36]. This result is impressive concerning the theory of social propagation about accepting peers behaviors. Our study showed that the majority of pregnant women had a positive attitude towards normal delivery and earned higher scores and thus preferred normal delivery which is consistent with the findings of Pourheydari et al. [34], but different from the results of Shahraki-Sanavi et al. [4]. This difference can be attributed to the time interval between two studies, cultural differences, or the experiences of samples from their previous delivery.
Pregnant women who were employees or university students preferred normal delivery compared to those who were housewives. Moreover, this study showed that occupation could determine the choice of delivery mode. Results of Safari-Moradabadi et al. confirmed this result and concluded that employed women preferred normal delivery more than unemployed women [11]. However, in some studies, employed women requested CS more [4-6, 37].
The study found that women with primary education and less than high school eduction preferred CS, while those with high school diploma as well as college-educated women preferred to have normal delivery. Safari-Moradabadi et al. also found similar results and showed that with the increase in educational level, the preference for normal delivery has also increased [11]. Many studies contradict this conclusion and have reported that women with higher education prefer CS [1, 4-6, 25, 38]. Considering the date of many studies carried out in Iran, it can be argued that the results of the present study contradict some of the previous studies due to change in the country’s policies in promoting normal delivery.
Our study results indicate a significant relationship between the preference of the delivery mode and the previous delivery method, where pregnant women preferred to give birth by the same method they used for their previous delivery. This result has also been reported in other studies [33, 39]. Preference for the delivery mode in this study was also correlated to the method by which the participants themselves were born which can be attributed to the influence of their mothers, although a similar study was not found for comparison. The findings of this study showed that the preference for delivery mode could be influenced by the inductions and claims of people around such as doctors, mothers, friends and relatives, social media, and national plans. This finding is consistent with the results of Kashfi et al. study [32].
These inductions and claims can be right or wrong, but what’s important is that national policies and comprehensive plans in this area can affect all these inductions. For this reason, further studies should be conducted to examine the impact of a national comprehensive plan to reduce the rate of CS and promote normal delivery in different cities.
The limitation of the present study was using a questionnaire to determine the views of pregnant mothers about their preferred type of delivery, which may have failed to unravel all the facts in this issue.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of Shahed University (Code: IR.shahed.REC.1394.104).
Funding
The present paper was extracted from the MSN thesis of the first author, in Department of Obstetric and Gynecologic, School of Medicine, Shahed University and has received support from the Deputy of Research of this university.
Authors' contributions
Conceptualization, funding acquisition: Shahrzad Hadavand, Maryam Rabiee; Data collection, preparing the draft: Nooshin Jalali; Data analysis: Farhad Jafari; and Reviewing and editing: Kobra Khajavi Shojaie.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgements
Authors would like to thank the Deputy of Research and staff of Mostafa Khomeini Hospital for their valuable cooperation.
References
MiriFarahani L, AbbasiShavazi MJ. [Caesarean section change trends in Iran and some demographic factors associated with them in the past three decades (Persian)]. Journal of Fasa University of Medical Sciences. 2012; 2(3):127-34.
Chaillet N, Dubé E, Dugas M, Francoeur D, Dubé J, Gagnon S, et al. Identifying barriers and facilitators towards implementing guidelines to reduce caesarean section rates in Quebec. Bulletin of the World Health Organization. 2007; 85(10):791-7. [DOI:10.2471/BLT.06.039289] [PMID] [PMCID]
MacDorman MF, Menacker F, Declercq E. Cesarean birth in the United States: epidemiology, trends, and outcomes. Clinics in Perinatology. 2008; 35(2):293-307. [DOI:10.1016/j.clp.2008.03.007] [PMID]
Shahraki-Sanavi F, Rakhshani F, Navidiyan A, Ansari-Moghaddam A. A study on attitude of pregnant women with intention of elective cesarean based on theory of planned behavior. Zahedan Journal of Research in Medical Sciences. 2012; 14(9):95-7.
Mohammadpourasl A, Rostami F, Torabi S. [Prevalence of Cesarean Section and its demographic correlates in Tabriz (Persian)]. medical Journal of Tabriz University of Medical Sciences. 2006; 28(3):101-5.
Shams-Ghahfarokhi Z, Khalajabadi-Farahani F. Intention for Cesarean Section versus vaginal delivery among pregnant women in Isfahan: Correlates and determinants. Journal of Reproduction & Infertility. 2016; 17(4):230-9. [PMID] [PMCID]
Radnia N, Otogara M, Shahnavazian S, Jafarian F, Khaled Noori M, Yoosefi Z, et al. Comparison of quality of life between mothers with cesarean or vaginal delivery. Health Research Journal. 2017; 2(3):177-84. [DOI:10.18869/acadpub.hrjbaq.2.3.177]
Bahadori F, Hakimi S, Heidarzade M. The trend of caesarean delivery in the Islamic Republic of Iran. Eastern Mediterranean Health Journal. 2013; 19(Suppl. 2):S67-S70. [DOI:10.26719/2013.19.Supp3.S67]
Azami-Aghdash S, Ghojazadeh M, Dehdilani N, Mohammadi M. Prevalence and causes of Cesarean Section in Iran: Systematic review and meta-analysis. Iranian Journal of Public health. 2014; 43(5):545-55. [PMID] [PMCID]
Althabe F, Sosa C, Belizán JM, Gibbons L, Jacquerioz F, Bergel E. Cesarean Section rates and maternal and neonatal mortality in low‐, medium‐, and high‐income countries: An ecological study. Birth. 2006; 33(4):270-7. [DOI:10.1111/j.1523-536X.2006.00118.x] [PMID]
Safari-Moradabadi A, Alavi A, Pormehr-Yabandeh A, Eftekhaari TE, Dadipoor S. Factors involved in selecting the birth type among primiparous women. Journal of Education and Health Promotion. 2018; 7:55. [DOI:10.4103/jehp.jehp_150_17] [PMID] [PMCID]
Robson S, Carey A, Mishra R, Dear K. Elective caesarean delivery at maternal request: A preliminary study of motivations influencing women’s decision‐making. Australian and New Zealand Journal of Obstetrics and Gynaecology. 2008; 48(4):415-20. [DOI:10.1111/j.1479-828X.2008.00867.x] [PMID]
Minkoff H, Chervenak FA. Elective primary cesarean delivery. New England Journal of Medicine. 2003; 348(10):946-50. [DOI:10.1056/NEJMsb022734] [PMID]
Hannah ME. Planned elective Cesarean Section: A reasonable choice for some women? Canadian Medical Association Journal. 2004; 170(5):813-4. [DOI:10.1503/cmaj.1032002] [PMID] [PMCID]
Robson MS. Can we reduce the caesarean section rate? Best Practice & Research Clinical Obstetrics & Gynaecology. 2001; 15(1):179-94. [DOI:10.1053/beog.2000.0156] [PMID]
Poobalan AS, Aucott LS, Gurung T, Smith WCS, Bhattacharya S. Obesity as an independent risk factor for elective and emergency caesarean delivery in nulliparous women-systematic review and meta‐analysis of cohort studies. Obesity Reviews. 2009; 10(1):28-35. [DOI:10.1111/j.1467-789X.2008.00537.x] [PMID]
Roman H, Goffinet F, Hulsey TF, Newman R, Yves Robillard P, Hulsey TC. Maternal body mass index at delivery and risk of caesarean due to dystocia in low risk pregnancies. Acta Obstetricia et Gynecologica Scandinavica. 2008; 87(2):163-70. [DOI:10.1080/00016340701762975] [PMID]
Bell JS, Campbell DM, Graham WJ, Penney GC, Ryan M, Hall MH. Do obstetric complications explain high caesarean section rates among women over 30? A retrospective analysis. Bmj. 2001; 322(7291):894-5. [DOI:10.1136/bmj.322.7291.894] [PMID] [PMCID]
Callaway LK, Lust K, McIntyre HD. Pregnancy outcomes in women of very advanced maternal age. Australian and New Zealand Journal of Obstetrics and Gynaecology. 2005; 45(1):12-6. [DOI:10.1111/j.1479-828X.2005.00333.x] [PMID]
Lin HC, Sheen TC, Tang CH, Kao S. Association between maternal age and the likelihood of a Cesarean Section: A population‐based multivariate logistic regression analysis. Acta Obstetricia et Gynecologica Scandinavica. 2004; 83(12):1178-83. [DOI:10.1111/j.0001-6349.2004.00506.x] [PMID]
Cunningham F, Leveno K, Bloom S, Spong CY, Dashe J. Williams obstetrics, 24e. New York: McGraw-Hill Education; 2014.
Shellhaas CS, Gilbert S, Landon MB, Varner MW, Leveno KJ, Hauth JC, et al. The frequency and complication rates of hysterectomy accompanying cesarean delivery. Obstetrics and Gynecology. 2009; 114(2 Pt 1):224-9. [DOI:10.1097/AOG.0b013e3181ad9442] [PMID] [PMCID]
Amu O, Rajendran S, Bolaji II. Maternal choice alone should not determine method of delivery. BMJ. 317(7156): 463-465.
Jorfi M, Afshari P, Zaheri H, Jahandideh M. The relationship between health promotion lifestyle and type of delivery in reproductive aged women in Ahvaz, Iran. International Journal of Bioassays. 2015; 4(6):3958-63. [DOI:10.21746/ijbio.2015.06.004]
Shariat M, Majlesi F, Azari S, Mahmoudi M. [Cesaren section in maternity hospitals in Tehran, Iran (Persian)]. Payesh. 2002; 1(3):5-10.
Dahifar H. [Early weight loss of breast-fed neonates born under C-section in their first 48 hours of life (Persian)]. Journal of Para Mdedical Sciences. 2003; 1(4):203-10.
Esmailpour N, Asgharnia M. [Early neonatal injuries in normal vaginal and cesarean deliveries (Persian)]. Journal of Guilan University of Medical Sciences. 2005; 14(54):76-84.
Hadizadeh F, Bahri N, Tavakolizadeh J. [Postpartum depression after vaginal delivery and emergency Cesarean Section(CS) in primigravida women (Persian)]. Journal of Kermanshah University of Medical Sciences. 2005; 8(4):21-30.
Nieminen K, Stephansson O, Ryding EL. Women’s fear of childbirth and preference for Cesarean Section-a cross‐sectional study at various stages of pregnancy in Sweden. Acta obstetricia et Gynecologica Scandinavica. 2009; 88(7):807-13. [DOI:10.1080/00016340902998436] [PMID]
Vahid Dastjerdi M. [A survey of indications, outcome and complications of Cesarean Section (Persian)]. Tehran University Medical Journal TUMS Publications. 1998; 56(1):42-5.
Kanani S, Allahverdipour H, AsghariJafarabadi M. Modeling the intention to choose natural vaginal delivery: Using reasoned action and social cognitive theories. Health promotion perspectives. 2015; 5(1):24-33. [DOI:10.15171/hpp.2015.004] [PMID] [PMCID]
Kashfi SM, Heydarabadi AB, Hafez AA, Rezaianzadeh A, Shahidi F. Effect of behavioral intention model-based education on decrease the rate of caesarean delivery among pregnant women. Journal of Paramedical Sciences. 2014; 5(1):16-23. [DOI:10.22037/jps.v5i1.5045]
Nouri Zadeh R, Kazempour R, Mohammadpour Asl A, Bakhtari Aghdam F. [Selection of mode of delivery and its related factors in pregnant women in Marand (Persian)]. The Journal of Urmia Nursing and Midwifery Faculty. 2009; 7(1):50-7.
Pourheydari M, Souzani A, Kasaeyan A. [The survey of knowledge and attitude of pregnant women referred to medical centers of Qom towards type of delivery (Persian)]. knowledge and health. 2007; 2(2):28-34.
Fathollahi Z, Hasanpour S, Mirghafourvand M, Bani S. Predictors of choice of childbirth in primiparous women in islamshahr. Advances in Environmental Biology. 2014:21-7.
Leone T, Padmadas SS, Matthews Z. Community factors affecting rising caesarean section rates in developing countries: An analysis of six countries. Social science & medicine. 2008; 67(8):1236-46. [DOI:10.1016/j.socscimed.2008.06.032] [PMID]
Alimohamadian M, Shariat M, Mahmoodi M, Ramezanzadeh F. [The influence of maternal request on the elective Cesarean Section rate in maternity hospitals in Tehran, Iran. Payesh. 2003; 2(2):133-9.
Wu E, Kaimal AJ, Houston K, Yee LM, Nakagawa S, Kuppermann M. Strength of preference for vaginal birth as a predictor of delivery mode among women who attempt a vaginal delivery. American Journal of Obstetrics and Gynecology. 2014; 210(5):440-e1. [DOI:10.1016/j.ajog.2013.11.021] [PMID] [PMCID]
Faraji DR, Zahiri SZ, Farjad BF. [A survey of knowledge and attitude of pregnant women about delivery methods (Persian)]. Journal of Guilan University of Medical Sciences. 2003; 12(46):69-75.
The study found that women with primary education and less than high school eduction preferred CS, while those with high school diploma as well as college-educated women preferred to have normal delivery. Safari-Moradabadi et al. also found similar results and showed that with the increase in educational level, the preference for normal delivery has also increased [11]. Many studies contradict this conclusion and have reported that women with higher education prefer CS [1, 4-6, 25, 38]. Considering the date of many studies carried out in Iran, it can be argued that the results of the present study contradict some of the previous studies due to change in the country’s policies in promoting normal delivery.
Our study results indicate a significant relationship between the preference of the delivery mode and the previous delivery method, where pregnant women preferred to give birth by the same method they used for their previous delivery. This result has also been reported in other studies [33, 39]. Preference for the delivery mode in this study was also correlated to the method by which the participants themselves were born which can be attributed to the influence of their mothers, although a similar study was not found for comparison. The findings of this study showed that the preference for delivery mode could be influenced by the inductions and claims of people around such as doctors, mothers, friends and relatives, social media, and national plans. This finding is consistent with the results of Kashfi et al. study [32].
These inductions and claims can be right or wrong, but what’s important is that national policies and comprehensive plans in this area can affect all these inductions. For this reason, further studies should be conducted to examine the impact of a national comprehensive plan to reduce the rate of CS and promote normal delivery in different cities.
The limitation of the present study was using a questionnaire to determine the views of pregnant mothers about their preferred type of delivery, which may have failed to unravel all the facts in this issue.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of Shahed University (Code: IR.shahed.REC.1394.104).
Funding
The present paper was extracted from the MSN thesis of the first author, in Department of Obstetric and Gynecologic, School of Medicine, Shahed University and has received support from the Deputy of Research of this university.
Authors' contributions
Conceptualization, funding acquisition: Shahrzad Hadavand, Maryam Rabiee; Data collection, preparing the draft: Nooshin Jalali; Data analysis: Farhad Jafari; and Reviewing and editing: Kobra Khajavi Shojaie.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgements
Authors would like to thank the Deputy of Research and staff of Mostafa Khomeini Hospital for their valuable cooperation.
References
MiriFarahani L, AbbasiShavazi MJ. [Caesarean section change trends in Iran and some demographic factors associated with them in the past three decades (Persian)]. Journal of Fasa University of Medical Sciences. 2012; 2(3):127-34.
Chaillet N, Dubé E, Dugas M, Francoeur D, Dubé J, Gagnon S, et al. Identifying barriers and facilitators towards implementing guidelines to reduce caesarean section rates in Quebec. Bulletin of the World Health Organization. 2007; 85(10):791-7. [DOI:10.2471/BLT.06.039289] [PMID] [PMCID]
MacDorman MF, Menacker F, Declercq E. Cesarean birth in the United States: epidemiology, trends, and outcomes. Clinics in Perinatology. 2008; 35(2):293-307. [DOI:10.1016/j.clp.2008.03.007] [PMID]
Shahraki-Sanavi F, Rakhshani F, Navidiyan A, Ansari-Moghaddam A. A study on attitude of pregnant women with intention of elective cesarean based on theory of planned behavior. Zahedan Journal of Research in Medical Sciences. 2012; 14(9):95-7.
Mohammadpourasl A, Rostami F, Torabi S. [Prevalence of Cesarean Section and its demographic correlates in Tabriz (Persian)]. medical Journal of Tabriz University of Medical Sciences. 2006; 28(3):101-5.
Shams-Ghahfarokhi Z, Khalajabadi-Farahani F. Intention for Cesarean Section versus vaginal delivery among pregnant women in Isfahan: Correlates and determinants. Journal of Reproduction & Infertility. 2016; 17(4):230-9. [PMID] [PMCID]
Radnia N, Otogara M, Shahnavazian S, Jafarian F, Khaled Noori M, Yoosefi Z, et al. Comparison of quality of life between mothers with cesarean or vaginal delivery. Health Research Journal. 2017; 2(3):177-84. [DOI:10.18869/acadpub.hrjbaq.2.3.177]
Bahadori F, Hakimi S, Heidarzade M. The trend of caesarean delivery in the Islamic Republic of Iran. Eastern Mediterranean Health Journal. 2013; 19(Suppl. 2):S67-S70. [DOI:10.26719/2013.19.Supp3.S67]
Azami-Aghdash S, Ghojazadeh M, Dehdilani N, Mohammadi M. Prevalence and causes of Cesarean Section in Iran: Systematic review and meta-analysis. Iranian Journal of Public health. 2014; 43(5):545-55. [PMID] [PMCID]
Althabe F, Sosa C, Belizán JM, Gibbons L, Jacquerioz F, Bergel E. Cesarean Section rates and maternal and neonatal mortality in low‐, medium‐, and high‐income countries: An ecological study. Birth. 2006; 33(4):270-7. [DOI:10.1111/j.1523-536X.2006.00118.x] [PMID]
Safari-Moradabadi A, Alavi A, Pormehr-Yabandeh A, Eftekhaari TE, Dadipoor S. Factors involved in selecting the birth type among primiparous women. Journal of Education and Health Promotion. 2018; 7:55. [DOI:10.4103/jehp.jehp_150_17] [PMID] [PMCID]
Robson S, Carey A, Mishra R, Dear K. Elective caesarean delivery at maternal request: A preliminary study of motivations influencing women’s decision‐making. Australian and New Zealand Journal of Obstetrics and Gynaecology. 2008; 48(4):415-20. [DOI:10.1111/j.1479-828X.2008.00867.x] [PMID]
Minkoff H, Chervenak FA. Elective primary cesarean delivery. New England Journal of Medicine. 2003; 348(10):946-50. [DOI:10.1056/NEJMsb022734] [PMID]
Hannah ME. Planned elective Cesarean Section: A reasonable choice for some women? Canadian Medical Association Journal. 2004; 170(5):813-4. [DOI:10.1503/cmaj.1032002] [PMID] [PMCID]
Robson MS. Can we reduce the caesarean section rate? Best Practice & Research Clinical Obstetrics & Gynaecology. 2001; 15(1):179-94. [DOI:10.1053/beog.2000.0156] [PMID]
Poobalan AS, Aucott LS, Gurung T, Smith WCS, Bhattacharya S. Obesity as an independent risk factor for elective and emergency caesarean delivery in nulliparous women-systematic review and meta‐analysis of cohort studies. Obesity Reviews. 2009; 10(1):28-35. [DOI:10.1111/j.1467-789X.2008.00537.x] [PMID]
Roman H, Goffinet F, Hulsey TF, Newman R, Yves Robillard P, Hulsey TC. Maternal body mass index at delivery and risk of caesarean due to dystocia in low risk pregnancies. Acta Obstetricia et Gynecologica Scandinavica. 2008; 87(2):163-70. [DOI:10.1080/00016340701762975] [PMID]
Bell JS, Campbell DM, Graham WJ, Penney GC, Ryan M, Hall MH. Do obstetric complications explain high caesarean section rates among women over 30? A retrospective analysis. Bmj. 2001; 322(7291):894-5. [DOI:10.1136/bmj.322.7291.894] [PMID] [PMCID]
Callaway LK, Lust K, McIntyre HD. Pregnancy outcomes in women of very advanced maternal age. Australian and New Zealand Journal of Obstetrics and Gynaecology. 2005; 45(1):12-6. [DOI:10.1111/j.1479-828X.2005.00333.x] [PMID]
Lin HC, Sheen TC, Tang CH, Kao S. Association between maternal age and the likelihood of a Cesarean Section: A population‐based multivariate logistic regression analysis. Acta Obstetricia et Gynecologica Scandinavica. 2004; 83(12):1178-83. [DOI:10.1111/j.0001-6349.2004.00506.x] [PMID]
Cunningham F, Leveno K, Bloom S, Spong CY, Dashe J. Williams obstetrics, 24e. New York: McGraw-Hill Education; 2014.
Shellhaas CS, Gilbert S, Landon MB, Varner MW, Leveno KJ, Hauth JC, et al. The frequency and complication rates of hysterectomy accompanying cesarean delivery. Obstetrics and Gynecology. 2009; 114(2 Pt 1):224-9. [DOI:10.1097/AOG.0b013e3181ad9442] [PMID] [PMCID]
Amu O, Rajendran S, Bolaji II. Maternal choice alone should not determine method of delivery. BMJ. 317(7156): 463-465.
Jorfi M, Afshari P, Zaheri H, Jahandideh M. The relationship between health promotion lifestyle and type of delivery in reproductive aged women in Ahvaz, Iran. International Journal of Bioassays. 2015; 4(6):3958-63. [DOI:10.21746/ijbio.2015.06.004]
Shariat M, Majlesi F, Azari S, Mahmoudi M. [Cesaren section in maternity hospitals in Tehran, Iran (Persian)]. Payesh. 2002; 1(3):5-10.
Dahifar H. [Early weight loss of breast-fed neonates born under C-section in their first 48 hours of life (Persian)]. Journal of Para Mdedical Sciences. 2003; 1(4):203-10.
Esmailpour N, Asgharnia M. [Early neonatal injuries in normal vaginal and cesarean deliveries (Persian)]. Journal of Guilan University of Medical Sciences. 2005; 14(54):76-84.
Hadizadeh F, Bahri N, Tavakolizadeh J. [Postpartum depression after vaginal delivery and emergency Cesarean Section(CS) in primigravida women (Persian)]. Journal of Kermanshah University of Medical Sciences. 2005; 8(4):21-30.
Nieminen K, Stephansson O, Ryding EL. Women’s fear of childbirth and preference for Cesarean Section-a cross‐sectional study at various stages of pregnancy in Sweden. Acta obstetricia et Gynecologica Scandinavica. 2009; 88(7):807-13. [DOI:10.1080/00016340902998436] [PMID]
Vahid Dastjerdi M. [A survey of indications, outcome and complications of Cesarean Section (Persian)]. Tehran University Medical Journal TUMS Publications. 1998; 56(1):42-5.
Kanani S, Allahverdipour H, AsghariJafarabadi M. Modeling the intention to choose natural vaginal delivery: Using reasoned action and social cognitive theories. Health promotion perspectives. 2015; 5(1):24-33. [DOI:10.15171/hpp.2015.004] [PMID] [PMCID]
Kashfi SM, Heydarabadi AB, Hafez AA, Rezaianzadeh A, Shahidi F. Effect of behavioral intention model-based education on decrease the rate of caesarean delivery among pregnant women. Journal of Paramedical Sciences. 2014; 5(1):16-23. [DOI:10.22037/jps.v5i1.5045]
Nouri Zadeh R, Kazempour R, Mohammadpour Asl A, Bakhtari Aghdam F. [Selection of mode of delivery and its related factors in pregnant women in Marand (Persian)]. The Journal of Urmia Nursing and Midwifery Faculty. 2009; 7(1):50-7.
Pourheydari M, Souzani A, Kasaeyan A. [The survey of knowledge and attitude of pregnant women referred to medical centers of Qom towards type of delivery (Persian)]. knowledge and health. 2007; 2(2):28-34.
Fathollahi Z, Hasanpour S, Mirghafourvand M, Bani S. Predictors of choice of childbirth in primiparous women in islamshahr. Advances in Environmental Biology. 2014:21-7.
Leone T, Padmadas SS, Matthews Z. Community factors affecting rising caesarean section rates in developing countries: An analysis of six countries. Social science & medicine. 2008; 67(8):1236-46. [DOI:10.1016/j.socscimed.2008.06.032] [PMID]
Alimohamadian M, Shariat M, Mahmoodi M, Ramezanzadeh F. [The influence of maternal request on the elective Cesarean Section rate in maternity hospitals in Tehran, Iran. Payesh. 2003; 2(2):133-9.
Wu E, Kaimal AJ, Houston K, Yee LM, Nakagawa S, Kuppermann M. Strength of preference for vaginal birth as a predictor of delivery mode among women who attempt a vaginal delivery. American Journal of Obstetrics and Gynecology. 2014; 210(5):440-e1. [DOI:10.1016/j.ajog.2013.11.021] [PMID] [PMCID]
Faraji DR, Zahiri SZ, Farjad BF. [A survey of knowledge and attitude of pregnant women about delivery methods (Persian)]. Journal of Guilan University of Medical Sciences. 2003; 12(46):69-75.
Article Type : Research |
Subject:
General
Received: 2019/06/18 | Accepted: 2019/06/18 | Published: 2019/06/18
Received: 2019/06/18 | Accepted: 2019/06/18 | Published: 2019/06/18
Send email to the article author
| Rights and permissions | |
 | This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Articles Copyright © The Author(s).
Owned by Guilan University of Medical Sciences.
Co-published by Negah Institute for Scientific Communication.
Contact Information
JHNM Office, Guilan University of Medical Sciences P.O.Box 41635-1873, Rasht, Iran
Journal Tel: +9813 33553202
Publisher Tel: +9821 453 55 555; +9821 453 55 000
Email: holisticnmj@gmail.com, nursjournal@gums.ac.ir
